

Clinically significant anxiety may be detected in patients with amyotrophic lateral sclerosis (ALS) Reference Kurt, Nijboer, Matuz and Kübler1 and may even precede the onset of motor symptoms. Reference Zucchi, Ticozzi and Mandrioli2
Current prevalence estimates for such a psychopathological feature in this population are highly heterogeneous – possibly due to the lack of large-scale studies on the topic and variability in the employment of psychometric outcome measures. Reference Kurt, Nijboer, Matuz and Kübler1,Reference Jellinger3 In fact, previous reviews on the topic Reference Kurt, Nijboer, Matuz and Kübler1,Reference Jellinger3 have pointed out that, within the relevant literature, the prevalence estimates of anxiety in ALS patients range from 0 to ∼63% – depending on the characteristics of the tools employed to assess these symptoms and the disease stage taken into consideration. Moreover, in this respect, evidence is conflicting on whether the rates of clinically significant anxiety are higher in ALS patients than in the general population. Reference Pagnini, Lunetta, Banfi, Rossi, Gorni and Castelnuovo4–Reference Benbrika, Doidy, Carluer, Mondou, Pélerin and Eustache6
Furthermore, it is currently under debate whether anxiety in ALS patients is of a psychogenic/reactive aetiology and thus possibly related to depressive symptoms, or falls within the spectrum of behavioural changes resulting from extra-motor, frontotemporal involvement. Reference Kurt, Nijboer, Matuz and Kübler1,Reference Benbrika, Doidy, Carluer, Mondou, Pélerin and Eustache6–Reference Faltracco, Pain, Dalla Bella, Riva, Telesca and Soldini9 For instance, Lillo et al Reference Lillo, Mioshi, Zoing, Kiernan and Hodges7 found that anxiety levels proved not be predictive of frontotemporal-spectrum behavioural changes in this population; by contrast, Siciliano et al Reference Siciliano, Trojano, Trojsi, Monsurro, Tedeschi and Santangelo8 detected a significant association between measures of anxiety and apathetic features. More recently, Faltracco et al Reference Faltracco, Pain, Dalla Bella, Riva, Telesca and Soldini9 replicated the findings of Siciliano et al Reference Siciliano, Trojano, Trojsi, Monsurro, Tedeschi and Santangelo8 by detecting significant correlations between anxiety levels and both depression and frontotemporal-spectrum behavioural changes in a fairly large cohort of ALS patients (N = 249).
In this respect, evidence on the association between anxiety and cognitive features in this population is likewise inconclusive. Reference Siciliano, Trojano, Trojsi, Monsurro, Tedeschi and Santangelo8,Reference Carelli, Solca, Faini, Madotto, Lafronza and Monti10,Reference Palumbo, Iazzolino, Callegaro, Canosa, Manera and Vasta11 In fact, Carelli et al Reference Carelli, Solca, Faini, Madotto, Lafronza and Monti10 failed to report any significant association between state- and trait-anxiety and a comprehensive measure of cognition, whereas Siciliano et al Reference Siciliano, Trojano, Trojsi, Monsurro, Tedeschi and Santangelo8 detected mild, albeit significant, associations between worse cognitive outcomes and higher state- and trait-anxiety levels. Moreover, Palumbo et al Reference Palumbo, Iazzolino, Callegaro, Canosa, Manera and Vasta11 showed that emotional disturbances (including anxiety) tend to become disentangled from social–cognitive deficits by being clustering together with behavioural changes – and, in particular, with apathetic features.
A further clinical domain whose association with anxiety has yet to be fully elucidated in ALS is the motor domain. Reference Benbrika, Doidy, Carluer, Mondou, Pélerin and Eustache6,Reference Siciliano, Trojano, Trojsi, Monsurro, Tedeschi and Santangelo8,Reference Faltracco, Pain, Dalla Bella, Riva, Telesca and Soldini9,Reference Larsson, Nordin and Nygren12 For instance, Siciliano et al Reference Siciliano, Trojano, Trojsi, Monsurro, Tedeschi and Santangelo8 found that a greater degree of bulbar involvement was associated with higher state- and trait-anxiety levels, with Benbrika et al Reference Benbrika, Doidy, Carluer, Mondou, Pélerin and Eustache6 replicating these findings with specific regard to trait-anxiety. Furthermore, Larsson et al Reference Larsson, Nordin and Nygren12 and Faltracco et al Reference Faltracco, Pain, Dalla Bella, Riva, Telesca and Soldini9 failed to report any significant association between measures of anxiety and motor-functional outcomes in their cohorts.
Taken together, the above research suggests that a comprehensive examination of the determinants of such a psychopathological feature in ALS should include measures of depression, cognition, behaviour and motor status.
Shedding further light on the above-mentioned matters is relevant to the care management of ALS patients: in fact, anxiety has been identified as a negative prognostic factor in this population by exerting a detrimental effect on both patients’ and carers’ quality of life. Reference Siciliano, Trojano, Trojsi, Monsurro, Tedeschi and Santangelo8,Reference Edge, Mills, Tennant, Diggle and Young13,Reference Vignola, Guzzo, Calvo, Moglia, Pessia and Cavallo14 Accordingly, its pharmacological and non-pharmacological treatment is a recognised clinical need. Reference Van Damme, Al-Chalabi, Andersen, Chiò, Couratier and De Carvalho15
Given the above proposals, this study aimed to (a) provide generalisable prevalence estimates of clinically significant anxiety levels from a large, retrospective cohort of ALS patients; (b) explore their motor, cognitive, behavioural and psychological underpinnings; and (c) compare anxiety levels between ALS patients and healthy controls.
Method
Participants
Data that were originally collected for clinical purposes on N = 433 ALS patients Reference Brooks, Miller, Swash and Munsat16 and consecutively referred to IRCCS Istituto Auxologico Italiano, Milano, Italy between 2016 and 2024, and having been administered the State- and Trait-Anxiety Inventory-Form Y (STAI-Y), Reference Spielberger, Gonzalez-Reigosa, Martinez-Urrutia, Natalicio and Natalicio17 were retrospectively retrieved. Patients did not present with comorbid frontotemporal dementia (FTD) according to current nosographic systems, Reference Rascovsky, Hodges, Knopman, Mendez, Kramer and Neuhaus18,Reference Gorno-Tempini, Hillis, Weintraub, Kertesz, Mendez and Cappa19 or with previously diagnosed psychiatric disorders traceable in medical history records. ALS patients with comorbid, full-blown FTD were not addressed within this study, in order to prevent the study sample from being phenotypically heterogeneous given that these patients, when compared with those without FTD, often display markedly distinct clinical features possibly rooted in different underlying neural vulnerabilities. Reference Beeldman, Raaphorst, Klein Twennaar, Govaarts, Pijnenburg and de Haan20–Reference De Marchi, Baj, Menegon, Caminiti, Sacchetti and Sarnelli22
Moreover, data on N = 313 healthy controls with available STAI-Y scores and no history of (a) neurological/psychiatric disorders, (b) active psychotropic medications or (c) severe, uncompensated general medical conditions were retrieved from the database of the above-mentioned institution. All healthy controls had a normal performance on Montreal Cognitive Assessment as per current Italian norms. Reference Aiello, Gramegna, Esposito, Gazzaniga, Zago and Difonzo23
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation, and with the Helsinki Declaration of 1975 as revised in 2013. All procedures involving human subjects/patients were approved by the Ethics Committee of IRCCS Istituto Auxologico Italiano (no. 2013_06_25).
Instruments
Both patients and healthy controls were administered STAI-Y – a 40-item, Likert-scaled, self-report questionnaire assessing both state- (STAI-Y1) and trait-anxiety (STAI-Y2) Reference Spielberger, Gonzalez-Reigosa, Martinez-Urrutia, Natalicio and Natalicio17 – and the Beck Depression Inventory (BDI) Reference Beck, Ward, Mendelson, Mock and Erbaugh24 – a 21-item, Likert-scaled, self-report questionnaire assessing cognitive–affective (BDI-CA) and somatic performance (BDI-SP) facets of depression.
Patients were further assessed for cognition via the cognitive section of the Edinburgh Cognitive and Behavioural ALS Screen (ECAS), Reference Poletti, Solca, Carelli, Madotto, Lafronza and Faini25 a performance-based battery (score range 0–136) including 5 subscales assessing language (ECAS-L, range 0–28); fluency (ECAS-F, range 0–24); executive functioning (ECAS-EF, range 0–48); memory (ECAS-M, range 0–24); and visuospatial abilities (ECAS-VS, range 0–12); as well as for behaviour via the Frontal Behavioural Inventory (FBI) Reference Alberici, Geroldi, Cotelli, Adorni, Calabria and Rossi26 – a 24-item, Likert-scaled, caregiver-reported questionnaire assessing ‘negative’ (FBI-A) and ‘positive’ (FBI-B) behavioural dysfunction of a dysexecutive nature.
With regard to motor status, disease severity was assessed via the ALS Functional Rating Scale Revised (ALSFRS-R), Reference Cedarbaum, Stambler, Malta, Fuller, Hilt and Thurmond27 progression rate (ΔFS) was computed according to Kimura et al’s Reference Kimura, Fujimura, Ishida, Nakajima, Furutama and Uehara28 formula and disease staging was retrieved via King’s staging system. Reference Roche, Rojas-Garcia, Scott, Scotton, Ellis and Burman29
Procedure
Within the clinical assessment session, patients were first assessed at our Institution for their motor functional status by a neurologist using ALSFRS-R, and subsequently assessed using ECAS for cognition by a psychologist with expertise in neuropsychology. Patients then completed STAI-Y and BDI so that their self-reported psychological status could be evaluated. During patients’ cognitive/psychological evaluation or at a separate juncture, a psychologist administered FBI to patients’ caregivers to enquire about behavioural changes. The multidimensional assessment of patients’ status could be subdivided into two or more sessions in the event of fatigue or distress.
Statistics
Prevalence of anxiety
The prevalence of clinically significant state- and trait-anxiety in both cohorts was determined by applying age-stratified, Italian cut-offs to t-scores on STAI-Y1 and -Y2, respectively. Reference Pedrabissi and Santinello30
Determinants of anxiety
Because STAI-Y scores proved to be distributed normally (skewness and kurtosis values < |1| and |3|, respectively Reference Kim31 (STAI-Y1: skewness 0.54, kurtosis −0.13; STAI-Y2: skewness 0.45, kurtosis −0.03)), the correlates of trait- and state-anxiety levels were explored via two linear models separately addressing STAI-Y1 and -Y2 scores as the outcomes and, as predictors, motor (i.e. disease duration in months, ALSFRS-R scores and ΔFS values), cognitive (i.e. ECAS-L/-EF/-F/-M and -VS scores), behavioural (i.e. FBI-A and -B scores) and depression (i.e. BDI-CA and -SP scores) measures. Within these models, age, education and gender were entered as covariates.
Similarly, two separate logistic models encompassing the same set of predictors and covariates were run on a below- versus above-cut-off score on STAI-Y1 and -Y2, in order to examine the determinants of clinically significant state- and trait-anxiety, respectively.
Within all models, collinearity was diagnosed in the presence of both a variance inflation factor (VIF) >10 and a tolerance index <0.10; Reference Midi, Sarkar and Rana32 a Bonferroni-adjusted significance threshold was addressed when selecting significant predictors (i.e. α adjusted = 0.05/numbers of target predictors (i.e. excluding covariates).
Between-group comparisons
Finally, in order to determine whether the prevalence of clinically significant state- and trait-anxiety differed between ALS patients and healthy controls, two separate logistic models were run by addressing group membership as the predictor and a below- versus above-cut-off score on STAI-Y1 and -Y2, respectively. Age, education and gender were entered as covariates within this mode, because the two groups were unmatched for these variables (age: t(744) = −7.78, p < 0.001; education: t(744) = 6.15, p < 0.001; gender: χ 2(1) = 32.42, p < 0.001).
Analyses were run using jamovi 2.3 (the jamovi project, Sydney, Australia; https://www.jamovi.org/). Missing data were excluded listwise within the regression models.
Results
Prevalence of anxiety
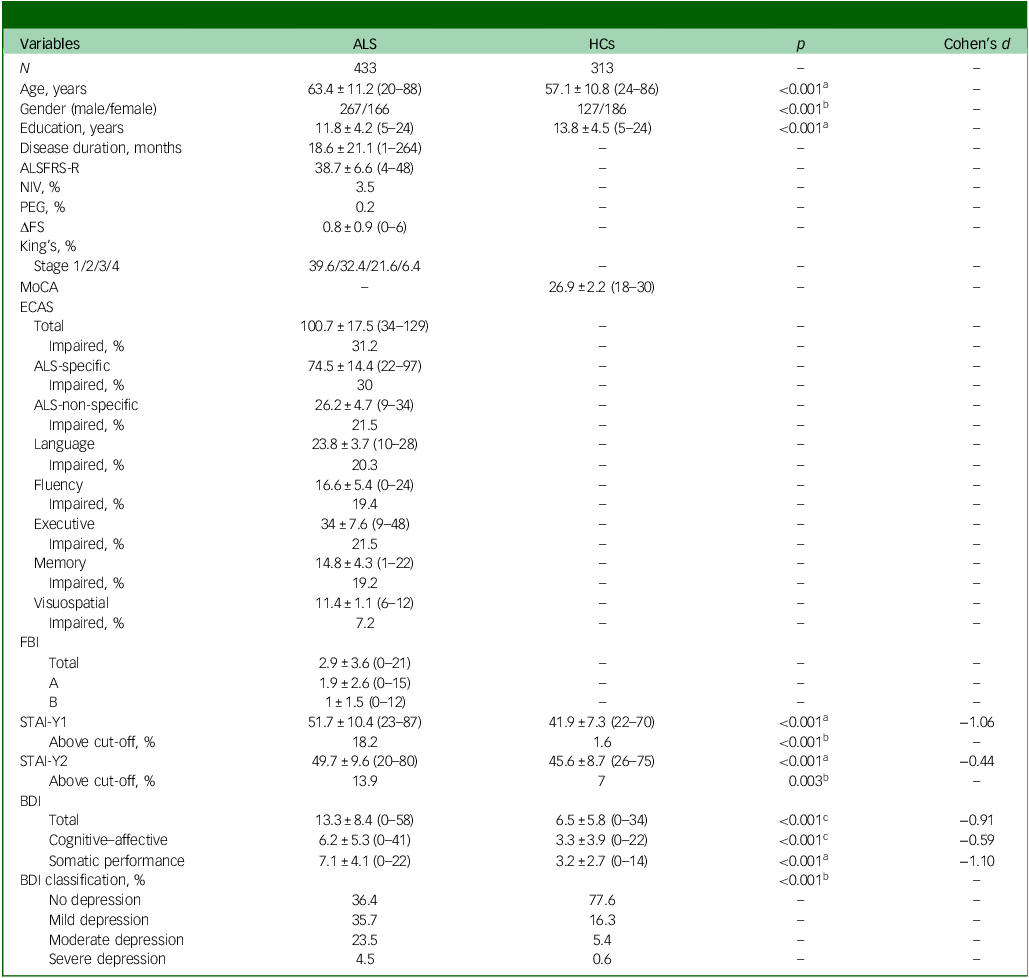
Table 1 summarises participants’ background and clinical features. The prevalence of clinically significant state-anxiety, as indicated by a STAI-Y1 score above cut-off, was 18.2% (79 of 433 patients), whereas that of trait-anxiety was 13.9% (60 of 433 patients). Moreover, patients exhibited higher levels of anxiety and depression than healthy controls, as reflected in continuous STAI-Y and BDI scores and clinical classification.
Participants’ background and clinical measures

ALS, amyotrophic lateral sclerosis; HCs, healthy controls; ALSFRS-R, Amyotrophic Lateral Sclerosis Functional Rating Scale-Revised; NIV, non-invasive ventilation; PEG, percutaneous endoscopic gastrostomy; ΔFS, progression rate; King’s, King’s College Staging System; MoCA, Montreal Cognitive Assessment; ECAS, Edinburgh Cognitive and Behavioural ALS Screen; FBI, Frontal Behavioural Inventory (A, negative subscale of the FBI; B, positive subscale of the FBI); STAI-Y1, State and Trait Anxiety Inventory Form Y – State-Anxiety; STAI-Y2, State and Trait Anxiety Inventory Form Y – Trait-Anxiety; BDI, Beck Depression Inventory. a.-statistic. b. χ 2-statistic. c. Mann–Whitney U-statistic. Continuous variables are reported as M ± s.d.; values within parentheses are empirical range; categorical variables are reported as either percentages or frequencies.
Determinants of anxiety
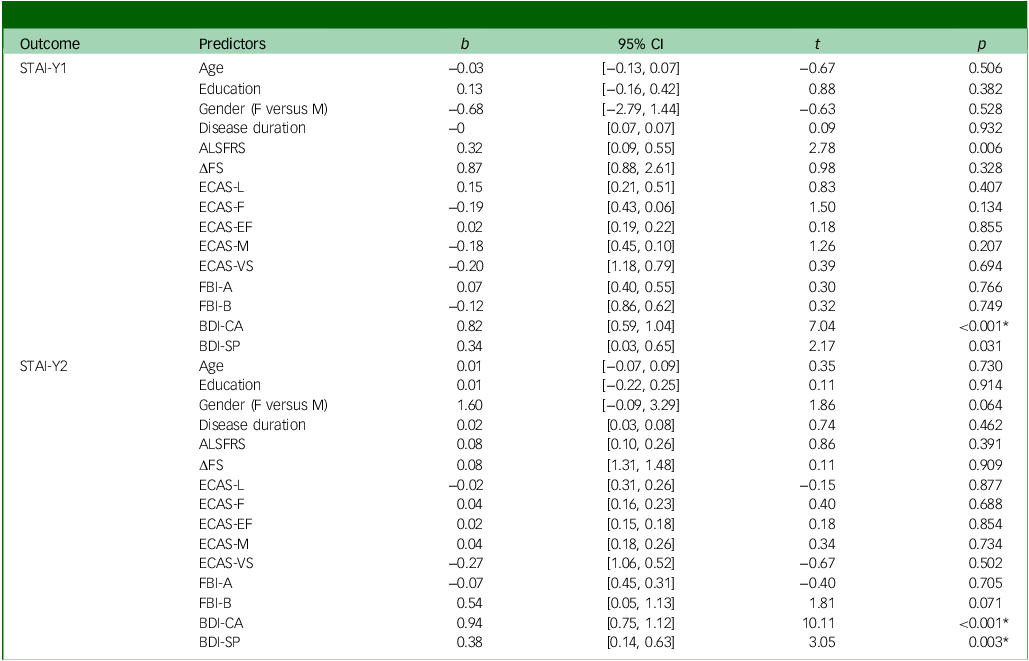
Tables 2 and 3 report the full results of linear and logistic models, respectively – which were run on N = 330 patients following the removal of missing data. No collinearity was recorded for any of the predictors of each model (VIF ≤ 2.72, tolerance index ≥ 0.37).
Effects of motor, cognitive, behavioural and depression measures on STAI-Y1 and STAI-Y2 as shown by multiple linear regression models

STAI-Y1, State and Trait Anxiety Inventory Form Y – State-Anxiety; STAI-Y2, State and Trait Anxiety Inventory Form Y – Trait-Anxiety; ALSFRS-R, ALS Functional Rating Scale-Revised; ΔFS, progression rate; ECAS, Edinburgh Cognitive and Behavioural ALS Screen (L, language; F, fluency; EF, executive functioning; M, memory; VS, visuospatial); FBI, Frontal Behavioural Inventory (A, negative subscale of the FBI; B, positive subscale of the FBI); BDI, Beck Depression Inventory (CA, Cognitive–Affective; SP, Somatic Performance). Age, education and gender were entered as covariates within these models. *Significant coefficient at α adjusted = 0.004.
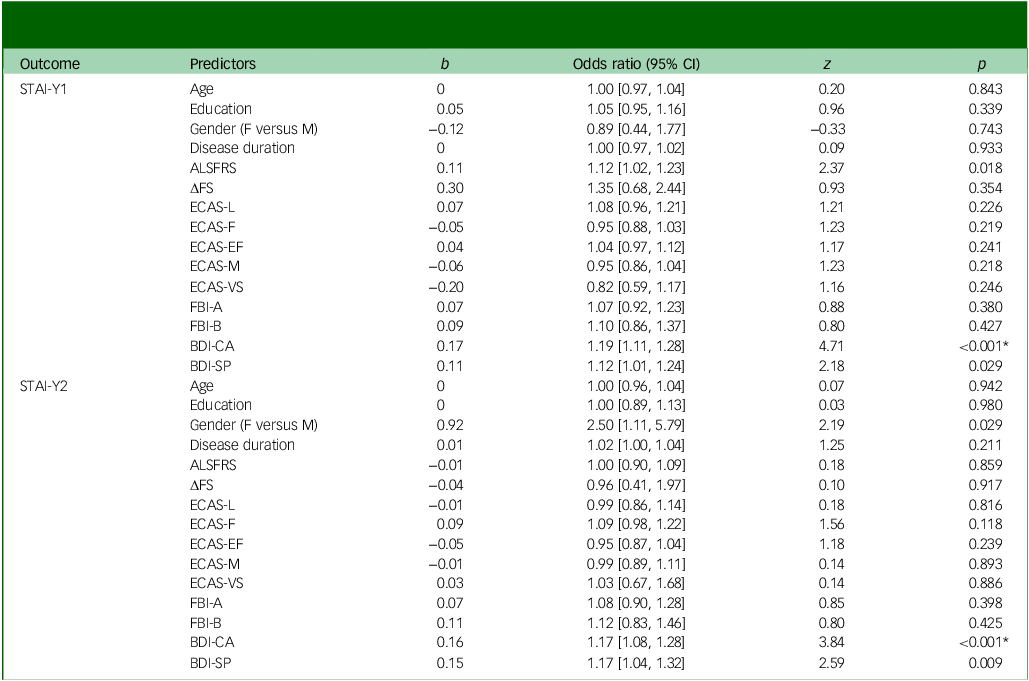
Effects of motor, cognitive, behavioural and depression measures on abnormal scores on STAI-Y1 and STAI-Y2 as shown by logistic regression models

STAI-Y1, State and Trait Anxiety Inventory Form Y – State-Anxiety; STAI-Y2, State and Trait Anxiety Inventory Form Y – Trait-Anxiety; ALSFRS-R, ALS Functional Rating Scale-Revised; ΔFS, progression rate; ECAS, Edinburgh Cognitive and Behavioural ALS Screen (L, language; F, fluency; EF, executive functioning; M, memory; VS, visuospatial); FBI, Frontal Behavioural Inventory (A, negative subscale of the FBI; B, positive subscale of the FBI); BDI, Beck Depression Inventory (CA, Cognitive–Affective; SP, Somatic Performance). Age, education and gender were entered as covariates within these models. *Significant coefficient at α adjusted = 0.004.
The linear model for STAI-Y1 scores explained 26.5% of variance (F(15, 314) = 7.54, p < 0.001), with only BDI-CA positively predicting these at α adjusted = 0.004 (β = 0.44, t(314) = 7.04, p < 0.001, η 2 = 0.12; Fig. 1). No other predictors indicated significance except for a marginally significant positive effect of ALSFRS-R scores (β = 0.21, t(314) = 2.78, p = 0.006, η 2 = 0.02). Analogous findings were derived from the logistic model on STAI-Y1 – with a higher score on BDI-CA predicting, at α adjusted = 0.004, a higher probability of a score above cut-off on this subscale (odds ratio 1.19, 95% CI [1.11, 1.28], z = 4.71, p < 0.001; Fig. 1).
Scatterplots for the association between STAI-Y1 (left) and STAI-Y2 (right) scores and BDI-CA. STAI-Y1, State and Trait Anxiety Inventory Form Y – State-Anxiety; STAI-Y2, State and Trait Anxiety Inventory Form Y – Trait-Anxiety. BDI-CA, Beck Depression Inventory Cognitive–Affective. The regression line is depicted along with its s.e. area.

The second linear model, addressing STAI-Y2, accounted for 45.4% of variance of the outcome (F(15, 314) = 17.44, p < 0.001), with BDI-CA and -SP as the only positive predictors at α adjusted = 0.004 (BDI-CA: β = 0.55, t(314) = 10.11, p < 0.001, η 2 = 0.18; BDI-SP: β = 0.17, t(314) = 3.05, p = 0.003, η 2 = 0.02). Similarly, within the logistic model addressing this STAI-Y subscale, only BDI-CA proved to be a positive predictor of clinically significant trait-anxiety at α adjusted = 0.004 (odds ratio 1.17, 95% CI [1.08, 1.28], z = 3.84, p < 0.001), with a marginally significant effect being found for BDI-SP (odds ratio 1.17, 95% CI [1.04, 1.32], z = 2.59, p = 0.009).
Between-group comparisons
Finally, net of age, education and gender, the probability of an abnormal score on both STAI-Y1 (odds ratio 12.80, 95% CI [5.52, 37.34], z = 5.34, p < 0.001) and STAI-Y2 (odds ratio 2.59, 95% CI [1.51, 4.59], z = 3.38, p < 0.001) was higher for ALS patients (STAI-Y1: M = 0.18, s.e. = 0.02; STAI-Y2: M = 0.14, s.e. = 0.02) when compared with healthy controls (STAI-Y1: M = 0.02, s.e. = 0.01; STAI-Y2: M = 0.06, s.e. = 0.01).
Discussion
This study provides clinicians and researchers with generalisable information on the prevalence and clinical correlates of state- and trait-anxiety in ALS from a retrospective cohort of non-demented patients. To the best of the authors’ knowledge, this is the largest report on the topic that employed a gold-standard, second-level questionnaire (i.e. STAI-Y) as the outcome measure, providing a sufficient degree of external validity to the current findings while also taking into account the crude prevalence estimate of ALS in the country where the study took place (Italy), which corresponds to 10.54 per 100 000 population (as evidenced by one of the largest epidemiological studies of ALS in Italy to date). Reference Chiò, Mora, Moglia, Manera, Canosa and Cammarosano33
Clinically significant state- and trait-anxiety levels (as assessed by STAI-Y1 and -Y2, respectively) proved not to be a ubiquitous finding in this population (≈18 and ≈14%, respectively). Such a finding substantially aligns with a previous report on a relatively large sample (N = 159), Reference Siciliano, Trojano, Trojsi, Monsurro, Tedeschi and Santangelo8 in which 19% of patients met the clinical criteria for anxiety-spectrum disorders; and with two studies on N = 631 Reference Larsson, Nordin and Nygren12 and 249 Reference Faltracco, Pain, Dalla Bella, Riva, Telesca and Soldini9 patients, respectively, completing a screening questionnaire – the Hospital Anxiety and Depression Scale, Reference Gibbons, Mills, Thornton, Ealing, Mitchell and Shaw34 with both reporting a 14% prevalence of clinically relevant anxiety. Of relevance, the current report indicates that the rate of clinically relevant anxiety levels is higher in ALS patients than in healthy controls. Reference Cui, Zhu, Zhou, Ren, Li and Li5
This study also sheds further light on the determinants of anxiety in ALS patients, showing that, in this population, such a psychopathological feature is solely driven by depressive symptoms and does not relate to cognitive and/or behavioural features. Although the close interplay between anxiety and depression is widely acknowledged and merely reflects the ‘physiological’ overlap between these two psychopathological clusters, Reference Kalin35 the present report thus aligns with those having previously forwarded the hypothesis of anxiety not falling within the spectrum of frontotemporal disorders in this population Reference Kurt, Nijboer, Matuz and Kübler1 – by, at variance, hinting at the fact that a psychogenic/reactive aetiology underlies this clinical manifestation. This complies with the finding of BDI-CA (assessing emotional and thinking pattern-related facets of depression) being the sole, systematic predictor of STAI-Y scores and classifications – at variance with BDI-SP (assessing neurovegetative components of depression), which showed either non-significant or smaller associations with STAI-Y. A further finding indirectly supporting the hypothesis of a psychogenic/reactive aetiology is the fact that a substantial degree of variance in STAI-Y scores was not accounted for by the present models – suggesting that individual, psychological determinants besides those herewith addressed play a non-negligible role in determining the emergence of anxiety. Among these putative variables, coping strategies towards the challenges faced when adjusting to the disease have been shown to significantly contribute to ALS patients’ psychological status. Reference Siciliano, Santangelo, Trojsi, Di Somma, Patrone and Femiano36
Moreover, this investigation did not report substantial associations between STAI-Y scores and motor-functional outcomes (i.e. disease duration, severity and progression rate). With regard to disease severity, this report is in agreement with previous investigations that likewise failed to link such a facet of motor status to anxiety levels in ALS. Reference Faltracco, Pain, Dalla Bella, Riva, Telesca and Soldini9,Reference Larsson, Nordin and Nygren12 At the same time, the marginally significant positive association between ALSFRS-R and STAI-Y1 scores detected in the present study deserves a potential explanation. Such a counterintuitive finding – enhanced motor status relating to higher levels of state-anxiety – might be accounted for by the fact that patients at the earlier stages of the disease (i.e. with high ALSFRS-R scores) are still within a phase of ‘emotional adjustment’. Reference Matuz, Birbaumer, Hautzinger and Kübler37 This hypothesis appears to be supported by a previous study showing that, in ALS patients, levels of psychological distress are higher during the diagnostic phase and decrease thereafter, Reference Vignola, Guzzo, Calvo, Moglia, Pessia and Cavallo14 as well as by a recent longitudinal investigation showing that patients’ anxiety levels decrease soon after diagnosis. Reference Larsson, Nordin and Nygren12
The above findings on the underpinnings of anxiety in this population may convey useful information regarding patients’ psychological well-being management. Indeed, assuming that patients’ anxiety is mostly driven by their depression levels, therapeutic approaches that target both these clusters would be appropriate for improving their well-being. Such a stance appears to be supported by a recent systematic review suggesting that interventions based on cognitive–behavioural and mindfulness might improve patients’ quality of life and psychological well-being, by also decreasing anxiety and depression levels. Reference Zarotti, Mayberry, Ovaska-Stafford, Eccles and Simpson38 It would thus be advisable that all ALS patients be screened for anxiety and depression using disease-specific scales, Reference Faltracco, Pain, Dalla Bella, Riva, Telesca and Soldini9,Reference Gibbons, Mills, Thornton, Ealing, Mitchell and Shaw34 so that those showing a clinically relevant level of psychological distress could be referred for further psychodiagnostic evaluation and, eventually, for possible psychological interventions tailored to their specific needs. Reference Kurt, Nijboer, Matuz and Kübler1 Such a diagnostic work-up appears to be even more relevant in light of the fact that, in the present cohort, the frequency of clinically significant anxiety levels was higher in ALS patients when compared with healthy controls from the general population.
This study is not free from limitations. First, as previously mentioned, no measures of coping strategies have been addressed – with the only psychological predictor taken into account being mood (i.e. BDI). Hence, further studies are needed aimed at replicating the current findings by the inclusion of measures of patients’ coping strategies within the context of disease adjustment. Second, depression in this study was measured by BDI, which includes certain items that do not account for motor disabilities. Future investigations should thus consider the employment of ALS-specific scales for depression. Reference Faltracco, Pain, Dalla Bella, Riva, Telesca and Soldini9,Reference Kim31,Reference Pain, Aiello, Gallucci, Miglioretti and Mora39 Third, this report did not include study-specific reliability measures for the instruments employed; hence, it cannot be ruled out that discrepancies between the present investigation and previous ones could be attributed, at least to some extent, to the varying degree of measurement error affecting test/questionnaire scores. Finally, this study did not include patients with comorbid FTD – thus not allowing inferences to be to drawn on the prevalence and determinants of anxiety in ALS patients with such a condition. This granted, at least to some extent, however, a greater level of phenotypic homogeneity in the sample – given that ALS patients with comorbid FTD display distinct clinical features when compared with both neuropsychologically unimpaired and cognitively and/or behaviourally impaired ALS patients. Reference Beeldman, Raaphorst, Klein Twennaar, Govaarts, Pijnenburg and de Haan20–Reference De Marchi, Baj, Menegon, Caminiti, Sacchetti and Sarnelli22 Future research is needed to explore the prevalence and correlates of anxiety in this specific population.
In conclusion, clinically significant levels of state- and trait-anxiety occurring in ≈18 and ≈14% of non-demented ALS patients, respectively, were mostly driven by cognitive and affective facets of depression, and were independent of motor and cognitive/behavioural features.
Data availability
Data-sets associated with the present study cannot be made publicly available on ethical–legal grounds but have been stored on an online repository (https://doi.org/10.5281/zenodo.19454469) and can be made available upon reasonable request of interested researchers to the corresponding author, B.P., who will forward a request for a data transfer agreement to the relevant Ethical Committee(s).
Acknowledgements
The authors thank the patients and their caregivers. The authors acknowledge the support of the Italian Ministry of Health (Ricerca Corrente/Ricerca Finalizzata) and the Italian Ministry of Education and Research (Dipartimenti di Eccellenza Programme 2023–2027 – Department of Pathophysiology and Transplantation, Dino Ferrari Centre, Università degli Studi di Milano). The authors also acknowledge ERN Euro-NMD for support.
Author contributions
E.N.A.: conceptualisation, analyses, drafting, revision; B.C., G.D.L.: analyses, drafting, revision; S.T., C.G., A.C., E.C., A.M.: data collection, revision; C.M., S.M., A.D., F.V., V.S.: resources, revision; A.D.S., D.M., R.F., S.B.: revision; B.P., N.T.: resources, drafting, revision.
Funding
This work was supported by BIBLIOSAN.
Declaration of interest
V.S. has received compensation for consulting services and/or speaking activities from AveXis, Cytokinetics, Italfarmaco, Liquidweb S.r.l., Novartis Pharma AG, Amylyx Pharmaceuticals, Biogen and Zambon Biotech SA; receives or has received research support from the Italian Ministry of Health, AriSLA and E-Rare Joint Transnational Call; is on the editorial board of Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration, European Neurology, American Journal of Neurodegenerative Diseases and Frontiers in Neurology. B.P. has received compensation for consulting services and/or speaking activities from Liquidweb S.r.l.; and is Associate Editor for Frontiers in Neuroscience. N.T. has received compensation for consulting services from Amylyx Pharmaceuticals and Zambon Biotech SA; and is Associate Editor for Frontiers in Aging Neuroscience. E.N.A. serves as an editorial board member for BMC Neurology and Journal of Alzheimer’s Diseaes. F.V. is Associate Editor for Journal of Alzheimer’s Disease.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation, and with the Helsinki Declaration of 1975 as revised in 2013. All procedures involving human subjects/patients were approved by the Ethics Committee of IRCCS Istituto Auxologico Italiano (no. 2013_06_25).


 Open access
Open access
eLetters
No eLetters have been published for this article.