


Introduction
The deinstitutionalization of chronically mentally ill individuals into community settings – alongside a shift in therapeutic outcome criteria toward incorporating patient-reported outcomes (PRO) – has increased focus on quality of life (QoL) assessment in schizophrenia (SZ) [Reference Awad and Voruganti1–Reference Lambert, Naber, Karow, Huber, Köhler and Heymann3]. In 1995, the World Health Organization Quality of Life Group articulated the most prevalent definition of QoL as an individual’s perception of their position in life in relation to cultural context, goals, expectations, and concerns, influenced in a complex way by the persons’ health, psychological state, level of independence, relationships, and environment [4].
QoL is broadly conceptualized as a multifaceted construct with four dimensions: general well-being, objective QoL (measurable welfare), subjective QoL (personal satisfaction), and health-related QoL (HRQoL) [Reference Eack and Newhill5]. Due to their broad applicability and cost-effectiveness, regulatory bodies in the US, UK, and France recommend generic QoL tools like the EQ-5D [Reference Rabin and de Charro6] or the 36-Item Short Form Health Survey (SF-36) [Reference Ware and Sherbourne7] in evaluating treatment outcomes for chronic health conditions [Reference Domenech, Pastore, Altamura, Bernasconi, Corral and Elkis8, Reference Patrick and Deyo9]. Of note, these assessment tools correlate well with schizophrenia-specific QoL scales [Reference Domenech, Pastore, Altamura, Bernasconi, Corral and Elkis8, Reference Auquier, Simeoni, Sapin, Reine, Aghababian and Cramer10].
Improving outcomes and QoL in chronic mental health disorders is nowadays a primary healthcare objective [11]. SZ, associated with markedly reduced QoL [Reference Bobes, Garcia-Portilla, Bascaran, Saiz and Bousoño12] has significant personal and societal costs [Reference Eack and Newhill5, Reference Jin and Mosweu13], thereby necessitating prolonged therapeutic intervention [Reference Ascher-Svanum, Faries, Zhu, Ernst, Swartz and Swanson14]. Notably, functional capacity and overall well-being exert a significant influence on treatment adherence and thus have a considerable impact on long-term outcomes [Reference Karow, Wittmann, Schöttle, Schäfer and Lambert15, Reference Ruggeri, Nosè, Bonetto, Cristofalo, Lasalvia and Salvi16]. In a pioneering 2015 meta-analysis comprising 19 studies (n = 5337), a substantial positive correlation was identified between QoL and satisfaction with therapy in individuals living with SZ, both of which may ultimately facilitate improved clinical outcomes and contribute to the mitigation of escalating healthcare costs [Reference Petkari and Pietschnig17]. In addition, earlier investigations have revealed a positive correlation between symptomatic remission and QoL [Reference Bodén, Sundström, Lindström and Lindström18–Reference Hofer, Mizuno, Wartelsteiner, Wolfgang Fleischhacker, Frajo-Apor and Kemmler20]. Our own previous studies have shown that symptomatic remission, resilience, and self-esteem impact SZ patients’ HRQoL [Reference Hofer, Mizuno, Wartelsteiner, Wolfgang Fleischhacker, Frajo-Apor and Kemmler20, Reference Wartelsteiner, Mizuno, Frajo-Apor, Kemmler, Pardeller and Sondermann21] and that emotional intelligence correlates with objective QoL [Reference Frajo-Apor, Pardeller, Kemmler, Mühlbacher, Welte and Hörtnagl22]. In addition, we have found that in terms of QoL, patients experiencing anxiety and depressive symptoms, parkinsonism, or unemployment, as well as those with negative feelings and attitudes toward antipsychotic medication, should be given special attention [Reference Hofer, Kemmler, Eder, Edlinger, Hummer and Fleischhacker23].
Antipsychotic treatment has the potential to alleviate the symptoms of SZ and improve overall QoL [Reference Bobes, Garcia-Portilla, Bascaran, Saiz and Bousoño12, Reference Leucht, Tardy, Komossa, Heres, Kissling and Salanti24, Reference Wehmeier, Kluge, Schneider, Schacht, Wagner and Schreiber25]; however, the variability in individual response and tolerability is significant [Reference Levine, Rabinowitz, Faries, Lawson and Ascher-Svanum26, Reference Wehmeier, Kluge, Schacht, Helsberg, Schreiber and Schimmelmann27]. A considerable number of patients discontinue pharmacotherapy prematurely [Reference Leucht, Cipriani, Spineli, Mavridis, Orey and Richter28, Reference Lieberman, Stroup, McEvoy, Swartz, Rosenheck and Perkins29], which is a significant factor in symptom recurrence [Reference Robinson, Woerner, Alvir, Bilder, Goldman and Geisler30]. In this context, the administration of long-acting injectable (LAI) antipsychotics represents an opportunity to support adherence and diminish the rates of discontinuation in comparison to treatment with oral drugs [Reference Citrome31, Reference Greene, Yan, Chang, Hartry, Touya and Broder32]. Earlier investigations have demonstrated that transitioning patients with SZ or schizoaffective disorder from oral formulations to LAI preparations has led to an improvement in HRQoL [Reference Macfadden, DeSouza, Crivera, Kozma, Dirani and Mao33, Reference Nasrallah, Duchesne, Mehnert, Janagap and Eerdekens34] and a decrease in hospitalization rates [Reference Macfadden, DeSouza, Crivera, Kozma, Dirani and Mao33, Reference Chue, Llorca, Duchesne, Leal, Rosillon and Montpied35]. However, in real-world settings, LAI treatment is often limited to a specific subset of patients characterized by inadequate adherence, a documented history of previous relapses, and/or a potential for self-harm or harm to others [Reference Sugawara, Kudo, Ishioka, Sato, Kubo and Yasui-Furukori36, Reference Keepers, Fochtmann, Anzia, Benjamin, Lyness and Mojtabai37]. The application of LAI antipsychotics in the treatment of early SZ may be even more contentious than their use in the maintenance phase of treatment [Reference Taylor and Ng38], although some clinical practice guidelines now recommend their use in patients experiencing a first episode of the illness [Reference Correll, Martin, Patel, Benson, Goulding and Kern-Sliwa39]. Yet, partial or non-adherence to antipsychotic treatment poses the most significant challenge during the early phases of schizophrenia [Reference Coldham, Addington and Addington40] and frequently results in incomplete symptom remission [Reference Andreasen, Carpenter, Kane, Lasser, Marder and Weinberger41], high relapse rates [Reference Robinson, Woerner, Alvir, Geisler, Koreen and Sheitman42], and self-harming behavior or suicide [Reference Correll, Solmi, Croatto, Schneider, Rohani-Montez and Fairley43]. However, the available literature comparing the impact of LAI and oral antipsychotics on patient outcomes in early-phase SZ is still characterized by contradictory statements in terms of treatment recommendations and different methodological conditions across studies [Reference Taylor and Ng38, Reference Fang, Huang and Shao44–Reference Winter-van Rossum, Weiser, Galderisi, Leucht, Bitter and Glenthøj47]. In consideration of this and focusing on subjective outcome, the current investigation aimed to evaluate possible differences in QoL among early-phase schizophrenia patients within the framework of the “European Long-acting Antipsychotics in Schizophrenia Trial” (EULAST) who were initiating treatment with either oral or LAI aripiprazole or paliperidone [Reference Winter-van Rossum, Weiser, Galderisi, Leucht, Bitter and Glenthøj47]. Furthermore, we investigated the degree to which sociodemographic factors, psychopathological symptoms, and medication side effects correlate with patient’s QoL in the course of treatment.
Methods
We refer to Winter-van Rossum et al. [Reference Winter-van Rossum, Weiser, Galderisi, Leucht, Bitter and Glenthøj47] and ClinicalTrials.gov, trial number NCT02146547 for an extensive description of the study design, the patient population, as well as the performed procedures.
Study design and patient population
Between 2015 and 2020, the EULAST, a large-scale, pragmatic, open-label, randomized clinical trial, was undertaken in 15 European nations and Israel across 50 general hospitals and psychiatric specialty clinics. Patients were randomly assigned to receive either LAI or oral formulations of aripiprazole or paliperidone and compared in regard to time to all-cause discontinuation during 19 months of treatment as the primary outcome. Eligible participants were 18 years or older, met DSM-IV criteria for SZ, and had an illness duration of 6 months to 7 years.
Procedures and clinical measurements
Following written informed consent (visit 1), baseline assessment occurred within 10 days (visit 2, week 0), after which participants were block randomized (1:1:1:1) to LAI aripiprazole, LAI paliperidone, oral aripiprazole, or oral paliperidone. Over 4 weeks, pre-study antipsychotics were tapered to the oral variant of the study drug. Patients assigned to LAI antipsychotic treatment initially commenced treatment with the oral formulation of the respective compound. At the 4-week interval following study initiation (visit 3, month 1), the pre-study antipsychotic was discontinued, and those assigned to LAI treatment received a first injection of the respective drug.
Considering that all treatment groups achieved a steady state by 8 weeks subsequent to the initiation of oral treatment, an extended visit with comprehensive assessments (visit 4, month 2) was performed, followed by similar evaluations every 3 to 4 months; monthly interim visits were minimized.
For the purpose of this publication, data that had been collected during visit 2 and across eight subsequent visits (visits 4, 5, 6, 7, 11, 15, 18, and 21) were analyzed as the EQ-5D-5L QoL score had been assessed at these visits.
EQ-5D-5L
QoL was assessed using the EQ-5D-5L, a patient-reported, generic, standardized instrument designed for the assessment of health outcomes [48, Reference Herdman, Gudex, Lloyd, Janssen, Kind and Parkin49], which has been empirically validated within patients diagnosed with SZ [Reference Prieto, Sacristán, Hormaechea, Casado, Badia and Gómez50]. It supplies a plain descriptive profile alongside a singular index value reflecting health status. The instrument is composed of the EQ-5D-5L descriptive system and a Visual Analogue Scale (VAS). The descriptive system covers five dimensions (mobility, self-care, usual activities, pain/discomfort, anxiety/depression) with five severity levels, generating an index score from 0 (death) to 1 (no problems). Utility scores were calculated using country-specific value sets [Reference Devlin, Parkin and Janssen51]. As some countries participating in the EULAST did not have published standard EQ-5D-5L value sets, comparable countries with established value sets were chosen instead (Germany for Austria, Romania for Bulgaria, Poland for Czechia, the USA for Israel [Reference Elsawy, Chavez, Avivi, Larouche, Wannesson and Cwynarski52, Reference Elsinga, Kuodi, Shibli, Gorelik, Zayyad and Wertheim53], and the UK for Greece [Reference Kontodimopoulos, Pappa, Niakas, Yfantopoulos, Dimitrakaki and Tountas54]). The EQ-5D-5L has demonstrated robust construct validity in the context of SZ and exhibits sensitivity to variations in HRQoL [Reference Prieto, Sacristán, Hormaechea, Casado, Badia and Gómez50, Reference Pitkänen, Välimäki, Endicott, Katajisto, Luukkaala and Koivunen55], even amidst differing degrees of illness severity within SZ patients [Reference Prieto, Sacristán, Hormaechea, Casado, Badia and Gómez50]. The VAS was not taken into account for our analyses.
Positive and Negative Syndrome Scale (PANSS)
The PANSS [Reference Kay, Fiszbein and Opler56] is the most widely used expert-rated scale for SZ symptoms, containing 30 items rated from 1 (absent) to 7 (extreme). Based on a publication by Leucht et al. [Reference Leucht, Kane, Kissling, Hamann, Etschel and Engel57], we used the following cut-offs to allow for a more clinical interpretation approach of the PANSS total score: mildly ill (PANSS total score ≤58), moderately ill (PANSS total score 59–75), and markedly/severely ill (PANSS total score >76). PANSS dimension analysis was based on the five-factor model by Marder et al. [Reference Marder, Davis and Chouinard58]: positive symptoms (PS; Items: P1, P3, P5, P6, N7, G1, G9, G12), negative symptoms (NS; Items: N1, N2, N3, N4, N6, G7, G16), disorganized thought (DT; Item: P2, N5, G5, G10, G11, G13, G15), anxiety/depression (AD; Items: G2, G3, G4, G6), and uncontrolled hostility/excitement (UHE; Items: P4, P7, G8, G14). In addition, adherence to the latest recommendations from the European Psychiatric Association (EPA) [Reference Galderisi, Mucci, Dollfus, Nordentoft, Falkai and Kaiser59] guided our operationalization of the negative symptom domain. Specifically, we restricted this dimension to the core items consistently shown to load onto the negative factor (NS: N1, N2, N3, N4, N6). The remaining PANSS symptom dimensions – positive symptoms (PS: P1, P3, P5, G9), Disorganized Thought(DT: P2, N5, G11), excited (EX: P4, P7, G8, G14), and depressed (DEP: G2, G3, G6) – were derived based on the factor structure proposed by Wallwork et al. [Reference Wallwork, Fortgang, Hashimoto, Weinberger and Dickinson60].
Systematic Monitoring of Adverse events Related to TreatmentS (SMARTS)
The SMARTS [Reference Haddad, Fleischhacker, Peuskens, Cavallaro, Lean and Morozova61] checklist has been developed by a consortium of twelve international experts to systematically evaluate whether patients diagnosed with SZ are presently experiencing a range of well-documented potential adverse effects associated with antipsychotic pharmacotherapy. Patients provide their feedback on eleven specific inquiries by indicating the pertinent side effects, while an additional open-ended question enables them to disclose any other conceivable side effects. It specifically appraises side effects that are experienced as troubling by the patient, including changes in weight and appetite, sexual dysfunction, hyperprolactinemia, gastrointestinal disturbances, urinary issues, postural hypotension, sedation, parkinsonism, tremor, akathisia, affective disturbances, and miscellaneous side effects.
St. Hans Rating Scale for extrapyramidal syndromes (SHRS)
The SHRS [Reference Gerlach, Korsgaard, Clemmesen, Lauersen, Magelund and Noring62] represents a multidimensional assessment tool devised to evaluate the severity of extrapyramidal symptoms, incorporating distinct sections for measuring parkinsonism (eight items), dyskinesia (eight items), akathisia (subjective and objective measures), and dystonia. A scale ranging from 0 to 6 is used to rate the critical components pertinent to a thorough evaluation of patients with dyskinesia. The dyskinesia sub-component is appraised in two distinct contexts: in a seated and relaxed state (“passive”) and during standardized voluntary movements, which frequently manifest dyskinesia (“active”). The SHRS has undergone testing to ascertain its reliability and validity, establishing itself as an easily administered, reliable, sensitive, and valid assessment tool [Reference Gerlach, Korsgaard, Clemmesen, Lauersen, Magelund and Noring62, Reference Nilsson, Hansen, Buchel, Gattaz and Gerlach63].
Statistical analysis
All statistical analyses were conducted with R Version 4.3.2 (The R Foundation for Statistical Computing, Vienna, Austria). In subgroup analyses, we corrected for multiple testing using the Bonferroni method. Consequently, p-values ≤ 0.005 are deemed statistically significant. For all other analyses, we used a significance level of 0.05. We restricted the study sample to participants who were included in the intention to treat (ITT) sample and had valid EQ-5D-5L data at any study visit.
We summarized continuous variables with mean and standard deviation (SD) for a normal distribution, and the median with the 25th and 75th percentiles otherwise. Categorical variables are presented with numbers and percentages.
In the primary analysis, we studied the relationships between oral versus LAI treatment and between treatment with paliperidone versus aripiprazole, respectively, with QoL assessed by the EQ-5D-5L. Due to the highly skewed distribution of the EQ-5D-5L, we compared individuals with an EQ-5D-5L score of 100% (i.e. ideal QoL) versus <100%. In secondary analyses, we investigated the individual dimensions of the EQ-5D-5L, including mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. We compared individuals who reported no problems (i.e. a value of 1) with those who reported any problems (i.e. a value between 2 and 5) in these sub-categories. For both the primary and the secondary analyses, we fitted generalized estimating equation (GEE) models with an exchangeable correlation structure using the R-package geepack [Reference Højsgaard, Halekoh and Yan64–Reference Yan and Fine66] and obtained odds ratios (OR) and 95% confidence intervals (CIs). We used the group indicator (i.e. LAI versus oral treatment and treatment with paliperidone versus aripiprazole) as the exposure variable and additionally adjusted for baseline values of the EQ-5D-5L or its individual dimensions, as appropriate. This allowed us to estimate the average treatment effect over time. In addition, we evaluated potential sex-specific QoL differences (EQ-5D-5L 100% versus <100% and having no problems in individual EQ-5D-5L dimensions) on average over time using the same methods.
In sensitivity analyses, we estimated the treatment effect at individual study visits at different points in time for both the primary and the secondary analyses. We additionally adjusted the GEE models for a variable indicating the study visits as well as for an interaction term between the treatment group and the study visits indicator. We used the R-package lsmeans [Reference Lenth67] to obtain predicted marginal means at the study visits. In another sensitivity analysis, we analyzed EQ-5D-5L as a continuous variable by implementing a GEE model similar to the primary analysis but using a Gaussian link function. Additionally, Mann–Whitney U test (continuous variable) and chi-squared test (categorical variable) were performed to detect possible differences regarding competitors between EQ-5D-5l as a continuous variable and EQ-5D-5L 100%.
In subgroup analyses of the primary analysis, we estimated the treatment effect on the EQ-5D-5L (100% versus <100%) across clinically relevant subgroups, including sex, age, the SMARTS checklist, the SHRS, and the PANSS (total score as well as PANSS dimensions based on the factor analyses by Marder et al., Wallwork et al., and EPA guidance). In addition to the variables included in the GEE model of the primary analysis, we included the subgroup variable of interest and an interaction term of the treatment group indicator with the subgroup variable of interest into the model. In terms of the SMARTS checklist, we compared the treatment effect between individuals with any side effects (SMARTS > 0) with those with no side effects (SMARTS = 0). In addition, we analyzed parkinsonism, dystonia, akathisia (subjective and objective), and dyskinesia (active and passive) using the SHRS and compared individuals with (SHRS > 0) and without these syndromes (SHRS = 0). In order to facilitate visualization of the results, we categorized the continuous variable age into thirds and psychopathology into mildly, moderately, and markedly/severely ill [Reference Leucht, Kane, Kissling, Hamann, Etschel and Engel57]. The corresponding p-values are from the GEE model that included the continuous variables.
Results
Study population
Of the 511 study participants included in the ITT sample, 492 had at least one valid EQ-5D-5L assessment (489 patients at visit 2 and 3 patients at another visit). Of those, 234 received oral and 258 received LAI antipsychotic treatment. There was a considerable decline in the study population from visit 2 through visit 21, at which 103 patients remained in the oral treatment group and 122 in the LAI treatment group. General characteristics and descriptive differences between the two treatment groups (LAI/oral) at baseline (visit 2) are depicted in Table 1. A table with descriptive statistics for the study population at visit 21, as well as a comparison of study completers versus non-completers (no data available at visit 21), is provided in the supplementary material (Supplementary Tables 1 and 2).
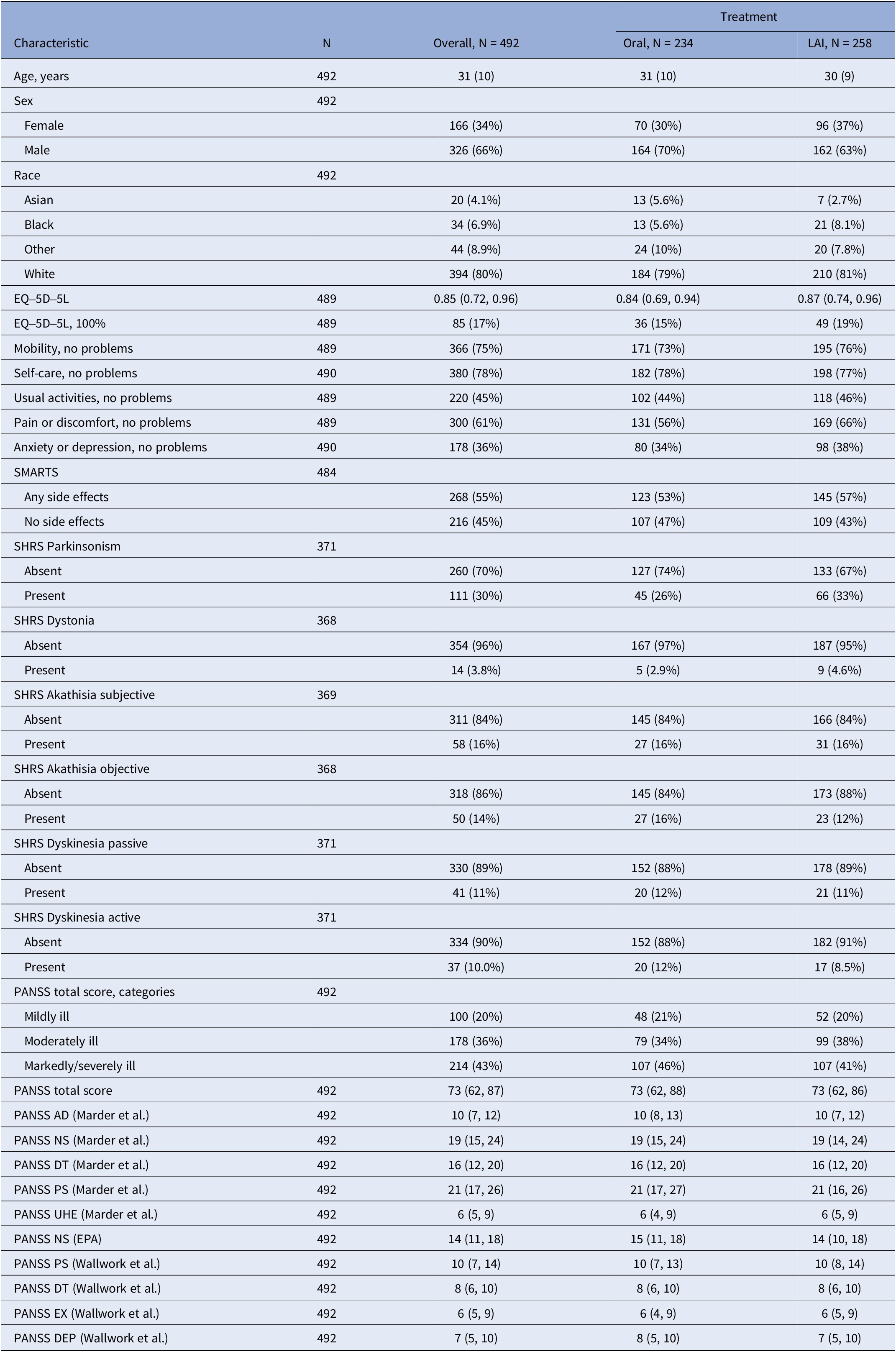
Descriptive statistics of the overall ITT sample, and the oral and LAI treatment groups at visit 2

Note: Descriptive statistics for age, sex, race, EQ-5D-5L, SMARTS, SHRS and PANSS total score (≤58 mildly ill, 59–75 moderately ill, ≥76 markedly/severely ill), and PANSS dimensions (Marder et al., Wallwork et al., and EPA guidance) of the ITT sample at baseline (visit 2) for the overall study population, oral and LAI treatment groups. Data are presented as mean (standard deviation) and median (25th, 75th percentiles) for continuous variables and as number (percentage) for categorical variable.
Abbreviations: AD, anxiety/depression; DEP, depressed; EX, excited; LAI, long-acting injectable; NS, negative symptoms; PANSS, positive and negative syndrome scale; PS, positive symptoms; SHRS, St. Hans rating scale for extrapyramidal syndromes; SMARTS, systematic monitoring of adverse events related to treatmentS; UHE, uncontrolled hostility/excitement.
At baseline, the mean overall age was 31 (SD 10), 80% were of white ethnicity, and 34% were female (30% in the oral treatment group, 37% in the LAI treatment group). Median PANSS total scores were comparable in the oral and LAI treatment groups as well as in patients assigned to treatment with aripiprazole or paliperidone.
EQ-5D-5L evaluation
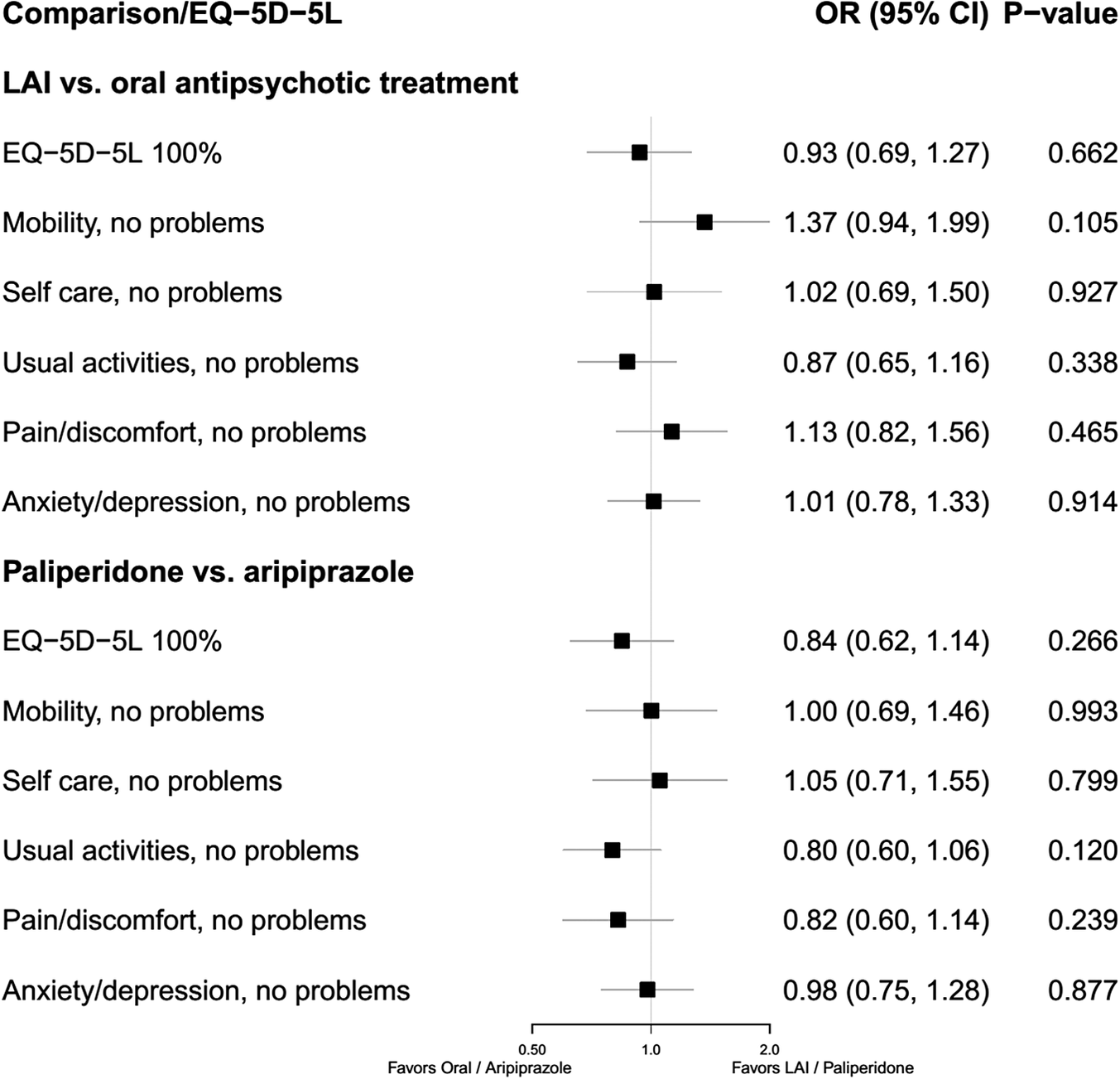
The results of the primary and secondary analyses are depicted in Figure 1. Overall, an improvement in QoL was observed during the study period, both in terms of the EQ-5D-5L total score and in terms of ideal QoL (EQ-5D-5L 100%) and all EQ-5D-5L dimensions. In total, 45% of patients across treatment groups reported an ideal QoL at visit 21 as compared to 17% at visit 4. The primary analysis did not identify a statistically significant effect of LAI versus oral antipsychotic treatment on ideal QoL as assessed by the EQ-5D-5L on average over time (OR 0.93 [95% CI 0.69, 1.27]; p = 0.662). We also did not find a statistically significant treatment effect on the individual EQ-5D-5L dimensions in our secondary analysis, defined as having no any problems in terms of mobility (p = 0.105), self-care (p = 0.927), usual activities (p = 0.338), pain/discomfort (p = 0.465), and anxiety/depression (p = 0.914).
Forest plot of treatment (LAI/ oral) and medication (paliperidone/aripiprazole) effect on average over time on EQ-5D-5L. Effect on average over time on EQ-5D-5L from baseline (visit 2) for treatment (LAI/ oral) and assigned medication (aripiprazole/paliperidone) for EQ-5D-5L 100% (ideal QoL) and EQ-5D-5L dimensions (no problems in: mobility, self-care, usual activities, pain/discomfort, anxiety/depression). Abbreviations: CI, confidence interval; LAI, long-acting injectable; OR, odds ratio.

Assessment of the potential impact of the assigned antipsychotic compound (aripiprazole/paliperidone) showed no significant effect either in terms of ideal QoL (OR 0.84 [95% CI 0.62, 1.14]; p = 0.266) nor in terms of the individual EQ-5D-5L dimensions (no problems with mobility [p = 0.993], self-care [p = 0.799], usual activities [p = 0.120], pain/discomfort [p = 0.239], and anxiety/depression [p = 0.877]).
The respective sensitivity analyses for differences in treatment effect (oral/LAI) on ideal QoL and EQ-5D-5L dimensions at individual study visits revealed statistically significant differences at visit 6 for ideal QoL (OR 0.52 [95% CI 0.28, 0.98]; p = 0.044), for no problems with mobility at visit 2 (OR 2.42 [95% CI 1.05, 5.55]; p = 0.037), and for no problems with pain/discomfort at visit 5 (OR 0.45 [95% CI 0.22, 0.94]; p = 0.034) (Supplementary Figure 1). Moreover, there were no significant differences when analyzing EQ-5D-5L as a continuous variable, neither between treatments (LAI/oral) nor between medications (aripiprazole/paliperidone) (Supplementary Figures 2 and 3). An additional analysis of possible differences between individuals with EQ-5D-5L 100% and EQ-5D-5L <100% proved to be non-significant for the continuous (p = 0.168) and categorical variables (0.107).
Subgroup evaluation
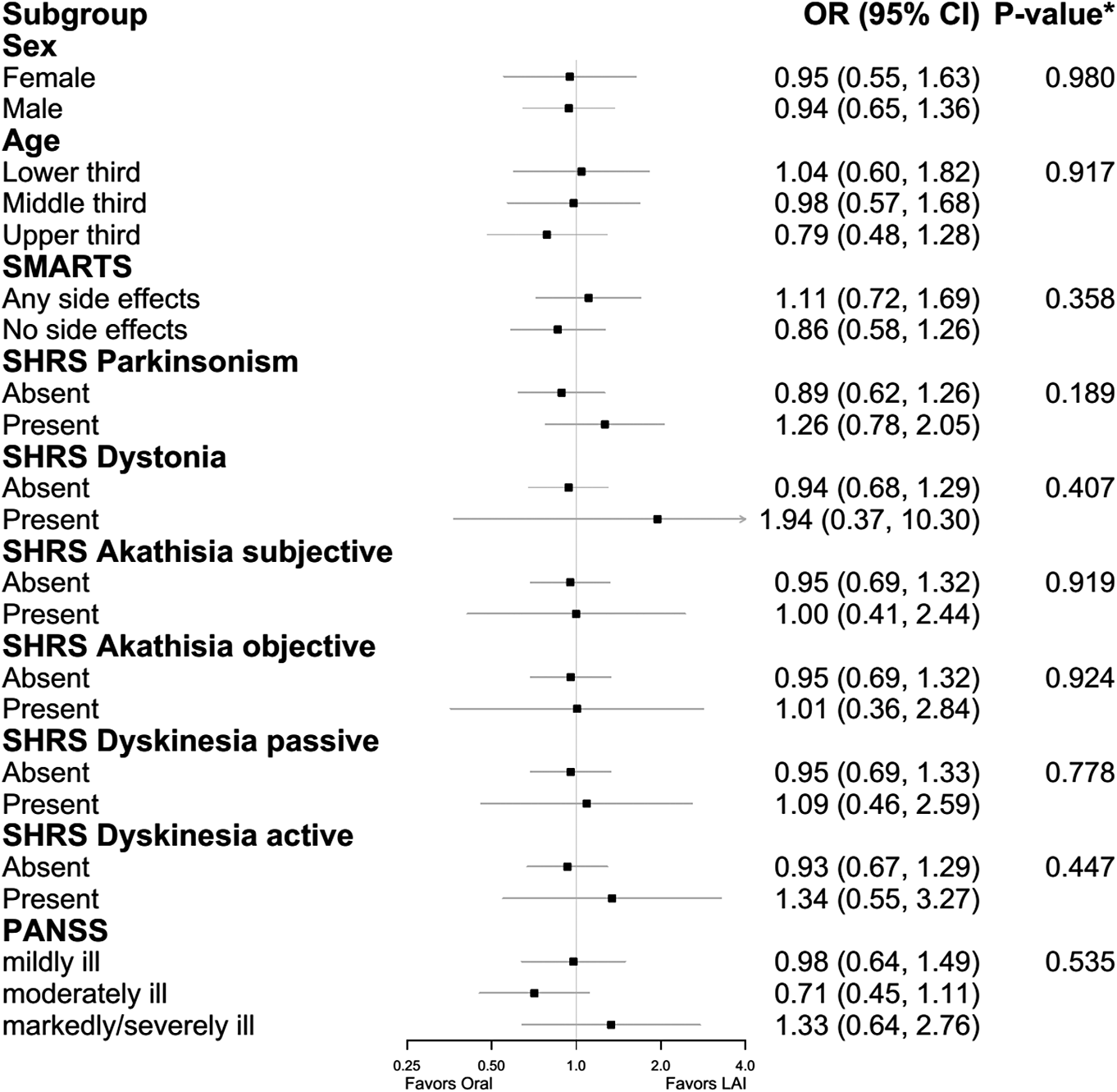
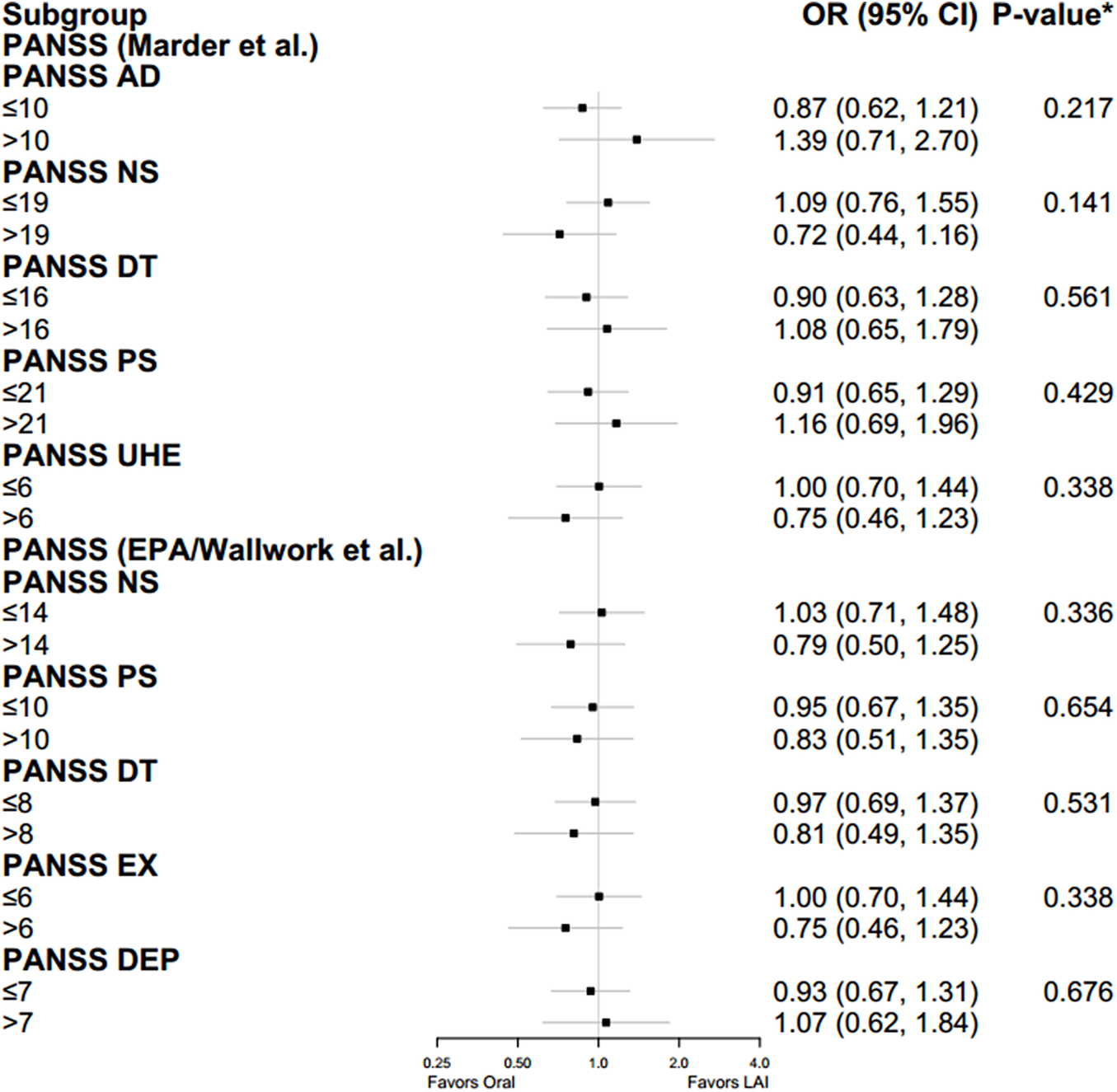
The results of the subgroup analyses are depicted in Figure 2. There was no significant difference in the average effect of LAI versus oral treatment on ideal QoL over time with respect to sex (p = 0.980), age (p = 0.917), and side effects of antipsychotic medication as assessed by the SMARTS (p = 0.358). Similar results were obtained for all SHRS dimensions and for the severity of symptoms as captured by the PANSS, with regard to the PANSS total score as well as according to factor analyses by Marder et al., Wallwork et al., and EPA guidance (all p > 0.05), which is outlined in Figure 3.
Forest plot on analyzing differences of the effect on average over time on EQ-5D-5L 100 % between assigned treatment (LAI/oral) for subgroups. Effect on average over time on EQ-5D-5L by subgroups from baseline (visit 2) analyzing possible differences between treatment groups (LAI/ oral). Subgroups include: sex, age (lower, middle, and upper third), SMARTS (absent or present), SHRS dimensions (absent or present), and PANSS (0–58 mildly ill, 59–75 moderately ill, 76–95 markedly ill, and 96–116 severely ill). *p-values from a model including the continuous variable for age and PANSS. All subgroup analyses were corrected for multiple testing using the Bonferroni method. Abbreviations: CI, confidence interval; LAI, long-acting injectable; OR, odds ratio; PANSS, positive and negative syndrome scale; SHRS, St. Hans rating scale for extrapyramidal syndromes; SMARTS, systematic monitoring of adverse events related to treatments.

Forest plot on analyzing differences of the effect on average over time on EQ-5D-5L 100 % between assigned treatment (LAI/oral) for PANSS dimensions. Effect on average over time on EQ-5D-5L by PANSS dimensions (Marder et al., Wallwork et al., and EPA guidance) from baseline (visit 2) analyzing possible differences between treatment groups (LAI/oral). *p-values from a model including the continuous variable for PANSS. All subgroup analyses were corrected for multiple testing using the Bonferroni method. Abbreviations: AD, anxiety/depression; CI, confidence interval; DEP, depressed; EX, excited; LAI, long-acting injectable; OR, odds ratio; NS, negative symptoms; PANSS, positive and negative syndrome scale; PS, positive symptoms; UHE, uncontrolled hostility/excitement.

Sex-specific evaluation
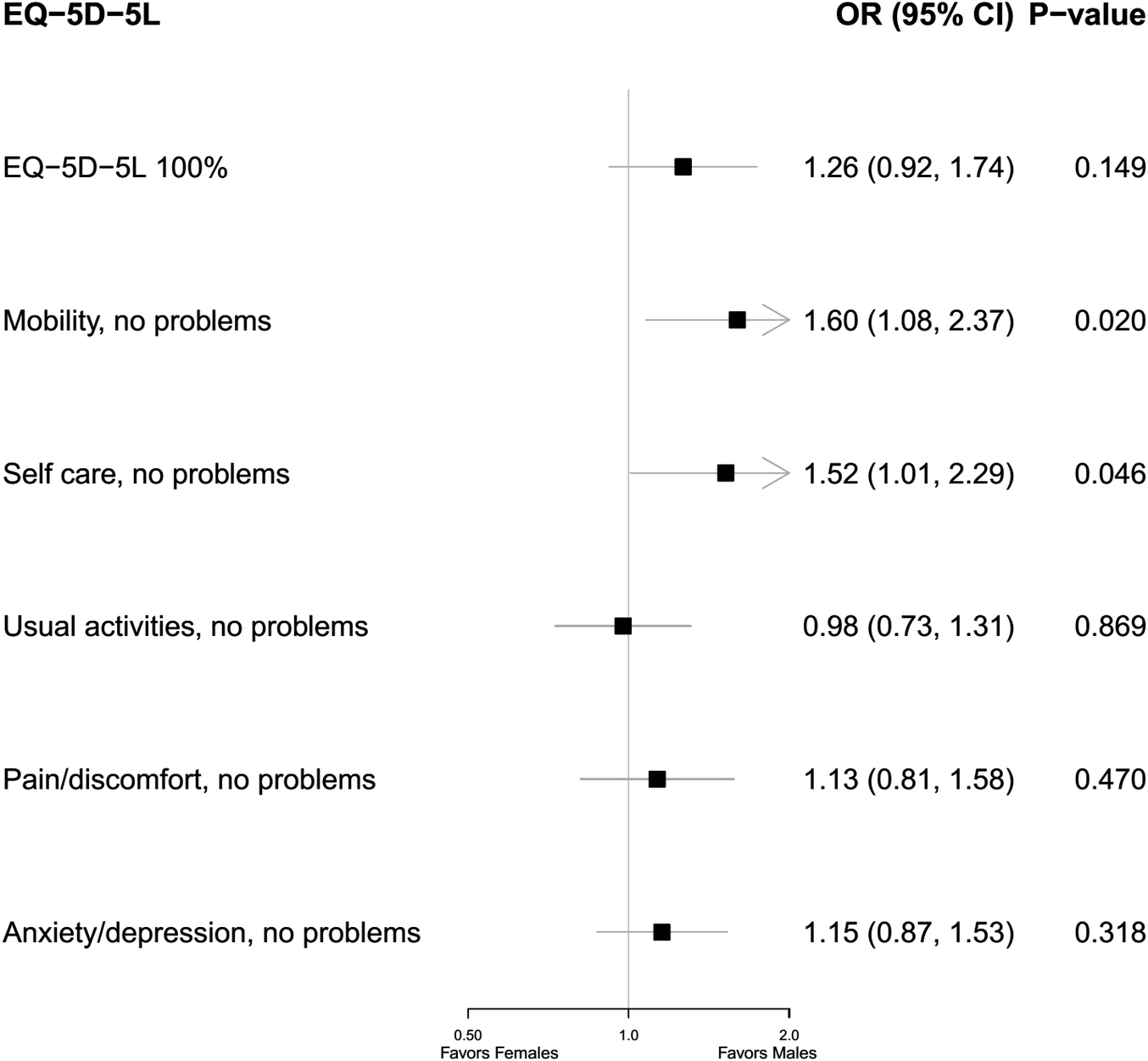
As depicted in Figure 4, we found no significant sex-specific differences in ideal QoL (p = 0.149) as well as the following EQ-5D-5L dimensions: no problems with usual activities (p = 0.869), pain/discomfort (p = 0.470), and anxiety/depression (p = 0.318). However, the odds for having no problems with mobility (OR 1.60 [95% CI 1.08, 2.37]; p = 0.020) and self-care (1.52 [1.01, 2.29]; p = 0.046) were significantly higher among males as compared to females.
Forest plot of the effect of sex (male/female) on average over time on EQ-5D-5L. Effect on average over time on EQ-5D-5L from baseline (visit 2) through visit 21 of sex (female/ male) for EQ-5D-5L 100% and EQ-5D-5L dimensions (no problems in: mobility, self-care, usual activities, pain/ discomfort, anxiety/ depression). Abbreviations: CI, confidence interval; OR, odds ratio.

Discussion
During the EULAST study, HRQoL generally improved, with no significant differences between LAI and oral antipsychotics in EQ-5D-5L scores. Secondary analyses likewise showed no treatment effects on individual EQ-5D-5L dimensions, suggesting that the administration route did not differentially impact QoL or PROs over time. Conversely, a 2016 narrative review found LAI risperidone improved functioning and QoL in stable SZ patients compared to oral or first-generation LAIs, but not in unstable SZ. Comparable efficacy was reported for LAI risperidone and LAI paliperidone, implying similar effects among second-generation LAIs with similar receptor profiles. Regarding the use of second-generation LAI antipsychotics in first-episode or recent-onset SZ, the authors stated the evidence to be far from conclusive, specifically concerning the duration of treatment [Reference Montemagni, Frieri and Rocca68].
Previous studies suggest that a potential efficacy advantage of LAI over oral antipsychotics becomes more apparent the better the study design reflects real-world conditions [Reference Kirson, Weiden, Yermakov, Huang, Samuelson and Offord69]. In EULAST, baseline EQ-5D-5L scores were already high [Reference Encheva, Djambazov, Vekov and Golicki70–Reference Van Wilder, Charafeddine, Beutels, Bruyndonckx, Cleemput and Demarest78] and PANSS scores low, which may have limited observable differences. However, LAIs may still offer unmeasured daily-life benefits, such as reduced treatment burden, especially for patients with cognitive deficits [Reference Fleischhacker, Oehl and Hummer79]. In addition, it should also be noted that, according to Osborne et al. [Reference Osborne, Dalton, Hertel, Schrover and Smith80], longer intervals between LAI injections (3-month interval compared to 2- and 4-week intervals) are associated with the highest utility scores. Therefore, current guiding principles on selecting PRO measures for clinical trials recommend a primary PRO, which is proximal to the disease or treatment (i.e. symptoms or treatment side effects) as opposed to more multidimensional and distal outcomes like HRQoL, which is likely to be affected by factors beyond the trial interventions, including social context and other life events [Reference Mercieca-Bebber, King, Calvert, Stockler and Friedlander81, Reference Luckett and King82].
No significant impact on overall EQ-5D-5L scores or individual QoL dimensions was observed based on the specific antipsychotic compound used (aripiprazole vs. paliperidone). Conversely, the QUALIFY study, a 28-week, randomized, head-to-head study comparing HRQoL in SZ patients treated with LAI aripiprazole or LAI paliperidone palmitate, demonstrated the superiority of LAI aripiprazole in terms of QoL improvements [Reference Naber, Hansen, Forray, Baker, Sapin and Beillat83]. The authors suggested this might be explained by the partial agonism of aripiprazole on dopamine D2 receptors, leading to a reduction in positive symptoms and potential improvements in negative and cognitive symptoms [Reference Lieberman84]. However, these inconsistent findings may be partly explained by differences in study populations and assessment methods. QUALIFY included an older sample with a longer illness duration and evaluated psychopathology using the CGI rather than the PANSS. In addition, QUALIFY assessed QoL with the schizophrenia-specific Heinrichs–Carpenter Quality of Life Scale (QLS, [Reference Heinrichs, Hanlon and Carpenter85]) instead of the generic EQ-5D-5L, and the study duration was rather short-framed with 4 weeks compared to up to 19 months of follow-up within EULAST. As a result, the study populations and outcome measures are not fully comparable, making cross-study interpretation challenging.
Subgroup analyses based on sex, age, medication side effects, and psychopathology did not reveal any significant differences in EQ-5D-5L outcomes between oral and LAI antipsychotic treatment. While no significant sex-specific differences in regard to ideal QoL were observed, males were significantly more likely to report no problems with mobility and self-care compared to females. This might suggest sex-related differences in functional outcomes; however, EQ-5D-5L general population norms consistently report diminished HRQoL among females across all countries with valid EQ-5D-5L index sets participating in the EULAST study [Reference Encheva, Djambazov, Vekov and Golicki70-Reference Van Wilder, Charafeddine, Beutels, Bruyndonckx, Cleemput and Demarest78]. Our results therefore suggest a less sex-specific reduced HRQoL in female compared to male SZ patients compared to the general population. Future studies are needed to clarify whether this is indeed a disease-specific finding.
Our study has several strengths and limitations. The mixed nature of previous findings highlights the need for careful selection of outcome measures and while generic tools such as the EQ-5D-5L enable comparisons across different diseases, they may be less sensitive to treatment-specific changes [Reference Bullinger, Kuhn, Leopold, Janetzky and Wietfeld86], especially in a study population with low baseline symptomatic burden, as in EULAST. In contrast, disease-specific questionnaires (e.g., the QLS for SZ) are designed and validated for a defined clinical population and assess aspects of QoL that are particularly relevant to that disorder and its treatment. These instruments are typically more sensitive to detecting clinically meaningful changes, including those resulting from pharmacological interventions, and therefore might have captured changes in HRQoL during EULAST more accurately. Furthermore, even though the EQ-5D 5L version shows fewer ceiling effects than the 3L version, suggesting increased sensitivity, significant ceiling effects exist in the EQ-5D [Reference Cheng, Pan, Chen, Cheng, Mulhern and Devlin87]. Thus, it cannot be fully excluded that the lack of significant differences in HRQoL outcomes between LAI and oral antipsychotics within EULAST could partially reflect a ceiling effect of the EQ-5D-5L rather than an actual absence of treatment effect. To take this ceiling effect into account, we compared individuals with an EQ-5D 5L of 100% with those <100%. However, categorizing the HRQoL variable may result in losing important information making the detection of clinically relevant differences less likely. Consequently, we conducted a sensitivity analysis including EQ-5D 5L as a continuous variable, which also resulted in no significant differences between the treatment groups.
Our objective was to implement an intention-to-treat approach, which holds the initial randomization between treatment groups [Reference Agency88]. This approach ensures that the treatment groups are comparable and any variation between groups is random [Reference Hollis and Campbell89]. A strength of our analysis is that we fitted a GEE model, which enables including participants into the analysis even if they do not provide data on all visits during the follow-up period. However, results may be biased if individuals who dropped out of the study differ from those who remained in the study, i.e. the drop-out is missing not at random [Reference Garrett, Fitzmaurice and Ware90]. Notably, the primary analysis of the EULAST trial showed that there were no statistically significant differences in all-cause discontinuation between the oral and LAI treatment groups [Reference Winter-van Rossum, Weiser, Galderisi, Leucht, Bitter and Glenthøj47]. In addition, baseline characteristics of the study participants were broadly similar when comparing individuals who completed the study with those who did not complete the study. Nevertheless, it cannot be ruled out that individuals who dropped out of the study worsened in HRQoL over time. Another strength is that we conducted a number of analyses across clinically relevant subgroups. We found no statistically significant differences in the effect of oral and LAI treatment on HRQoL on average over time. However, it is also important to note that we may have had limited statistical power to conduct these analyses. Consequently, further investigations are needed.
In conclusion, QoL plays an increasingly important role in adherence as therapy duration extends, ultimately influencing long-term outcomes in SZ [Reference Karow, Wittmann, Schöttle, Schäfer and Lambert15, Reference Ruggeri, Nosè, Bonetto, Cristofalo, Lasalvia and Salvi16, Reference Priebe, Gruyters, Heinze, Hoffmann and Jäkel91]. In the aforementioned meta-analysis of 19 studies, Petkari and Pietschnig [Reference Petkari and Pietschnig17] identified a strong association between QoL and treatment satisfaction. Furthermore, research has shown that in patients with stable SZ, adherence is primarily influenced by their recognition of the positive impact of pharmacological therapy on daily life [Reference Keith, Pani, Nick, Emsley, San and Turner92, Reference Lindenmayer, Eerdekens, Berry and Eerdekens93]. Key factors contributing to poor adherence include medication side effects, complex treatment regimens, and misunderstandings regarding dosage schedules [Reference Bai, Chen, Wu, Hung, Lin and Hu94]. In this context, it is likely for LAI antipsychotics to offer advantages in terms of adherence, patient functioning, and QoL during maintenance treatment. Further studies with longer follow-up periods are therefore needed and may provide deeper insights into potential subgroup benefits and the long-term impact of antipsychotic administration routes on HRQoL.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1192/j.eurpsy.2026.12209.
Acknowledgments
None.
Author contribution
A-T.S.: Conceptualization, Writing – Original draft preparation. L.T.: Methodology, Formal analysis, Visualization, Writing – Original draft preparation. F.P.: Conceptualization, Investigation, Writing – Reviewing and Editing. B.F-A.: Conceptualization, Investigation, Writing – Reviewing and Editing. W.W.F.: Supervision, Writing – Reviewing and Editing. M.D.: Supervision, Writing – Reviewing and Editing. A.H.: Conceptualization, Methodology, Visualization, Supervision, Project administration, Writing – Reviewing and Editing.
Financial support
We are grateful to Lundbeck and Otsuka, who provided financial support and study medication.
Competing interests
M.D. is an employee of Minerva Neurosciences with stock options. W.W.F. reports consultant fees from Angelini, Richter, Recordati, Lundbeck, Otsuka, Teva, Boehringer-Ingelheim, Pierre Fabre, Janssen, Sunovion, Dainippon-Sumitomo, Takeda, and Pfizer; speaker fees from Janssen, Lundbeck, Otsuka, Richter, and Recordati; and grants from Janssen, Lundbeck, and Otsuka. AH has received grant support from the federal state of Tyrol (F.21427, F.42856) and Gedeon Richter. In addition, he has received honoraria and/or travel support from Boehringer Ingelheim, Johnson & Johnson, Lundbeck, Recordati, and Rovi. All other authors declare no competing interests.
Declaration of generative AI and AI-assisted technologies in the writing process
Statement: During the preparation of this work, the authors used ChatGPT and DeepL in order to prune the manuscript according to submission criteria and to improve phrasing. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.



 Open access
Open access
Comments
No Comments have been published for this article.