


Statement of Research Significance
Research Question(s) or Topic(s): The International Neuropsychological Society Justice and Equity Subcommittee initiated a survey to obtain information about neuropsychological academic training and education programs, clinical practices, and research in as many of the 54 countries of the African continent as possible. Main Findings: Most respondents were clinical psychologists or neuropsychologists. Educational and training opportunities remain limited. Key barriers to program development included insufficient numbers of trained neuropsychologists, clinical training sites, and employment prospects. Despite this, there is strong interest in collaboration to accelerate the development of neuropsychology and neurosciences, given the heavy burden of neurological disease. Study Contributions: This survey represents the first systematic attempt to delineate the neuropsychology clinical practice, research, and education on the African continent. The survey results also report directly on participants’ interest in support from the International Neuropsychological Society in terms of the development of neuropsychology in their countries and the type of support required.
Introduction
Globally, 3.4 billion individuals live with neurological disease. Collectively, neurologic and psychiatric disorders have previously been reported to account for over 28% of the global burden of disease (Silberberg et al., Reference Silberberg, Anand, Michels and Kalaria2015). In fact, stroke, neonatal encephalopathy, dementia, epilepsy, meningitis, and autism spectrum disorder are among the conditions with the highest age-standardized disability-adjusted life years (DALYs; GBD 2021 Nervous System Disorders Collaborators*, 2024). The absolute burden of these diseases is higher in low- and middle-income countries (LMICs; Coates et al., Reference Coates, Ezzati, Robles Aguilar, Kwan, Vigo, Mocumbi, Becker, Makani, Hyder, Jain, Stefan, Gupta, Marx and Bukhman2021; Hamadeh et al., Reference Hamadeh, Van Rompaey and Metreau2023).
Research shows that those in sub-Saharan Africa (SSA) are disproportionately affected. In fact, in Africa, rates of neurological disease are reportedly up to twice those reported for high-income countries (HICs; GBD 2021 Nervous System Disorders Collaborators*, 2024). Higher rates of trauma and violence, non-communicable (e.g., stroke) and communicable diseases (e.g., cerebral malaria and HIV), socioeconomic disparities and related socio-environmental factors impacting neurodevelopment (e.g., malnutrition), are contributory (Akinyemi et al., Reference Akinyemi, Ovbiagele, Adeniji, Sarfo, Abd-Allah, Adoukonou, Ogah, Naidoo, Damasceno, Walker, Ogunniyi, Kalaria and Owolabi2021; GBD 2021 Nervous System Disorders Collaborators*, 2024; Schwaller, Reference Schwaller2024). For example, the incidence of traumatic brain injury (TBI) in SSA was previously reported to exceed five of ten global regions studied, and was notably lower than only two regions, one of which included North African countries (GBD 2016 Traumatic Brain Injury and Spinal Cord Injury Collaborators, 2019). Stroke-related GBD rates are also higher in LMICs (Behera et al., Reference Behera, Rahut and Mishra2024), with post-stroke rehabilitation services in Africa lacking (Tawa et al., Reference Tawa, Rhoda, Brink, Urimubenshi, Giljam-Enright, Charumbira, Niekerk, Louw and Louw2020). In addition, growing access to healthcare and population-level disease prevention strategies is increasing the average life expectancy across the African continent (Brazzaville: WHO Regional Office for Africa, 2022), which is attended by an increasing incidence and prevalence of disorders related to aging. From 1990 to 2010, the incidence of cerebrovascular disease grew by 28–62% in some African countries (Owolabi et al., Reference Owolabi, Akarolo-Anthony, Akinyemi, Arnett, Gebregziabher, Jenkins, Tiwari, Arulogun, Akpalu, Sarfo, Obiako, Owolabi, Sagoe, Melikam, Adeoye, Lackland and Ovbiagele2015). Population growth is expected to soon more than triple the incidence of dementia in SSA (GBD 2019 Dementia Forecasting Collaborators, 2022). Despite the tremendous need for medical resources and neuropsychological services related to brain health in Africa, and while much is known about neuropsychological resources and practice patterns in HICs (e.g., Kasten et al., Reference Kasten, Barbosa, Kosmidis, Persson, Constantinou, Baker, Lettner, Hokkanen, Ponchel, Mondini, Jonsdottir, Varako, Nikolai, Pranckeviciene, Harper and Hessen2021; Sweet et al., Reference Sweet, Klipfel, Nelson and Moberg2021), little is known about the role and scope of practice, training, clinical practice patterns, and scholarly activities of the discipline on the African continent outside of South Africa (SA; Hill-Jarrett et al., Reference Hill-Jarrett, Ikanga, Stringer, Kreutzer, DeLuca and Caplan2018; Truter et al., Reference Truter, Mazabow, Morlett Paredes, Rivera and Arango-Lasprilla2018). Such information is essential to the continued development of neuropsychology in Africa, where the tremendous value of the discipline could be realized at the intersection of high disease burden and scarce neurodiagnostic methodologies.
Kissani and Naji (Reference Kissani and Naji2020) shed light on this dearth of published African-based neuropsychology-related work. The review, spanning 1999–2019, revealed only 42 studies emanating from research studies carried out in 19/157 (12%) LMICs. Seven of these 42 studies (16.7%) were from Africa. Despite this, neuropsychology was reported as an independent discipline in psychology within these studies, with related educational practices and opportunities for ongoing professional development. The low publication rate of such studies from Africa is surprising given that the greatest proportion of LMICs are found in SSA (Hamadeh et al., Reference Hamadeh, Van Rompaey and Metreau2023).
Kissani and Naji (Reference Kissani and Naji2020) further note that the increase in neuropsychological disorders, coupled with the greater focus on neuropsychological research, highlights the importance of the discipline and, consequently, the need for greater education and training in LMICs, and in Africa in particular. They and others (Hill-Jarrett et al., Reference Hill-Jarrett, Ikanga, Stringer, Kreutzer, DeLuca and Caplan2018) point out that most neuropsychology training programs are found in English-speaking HICs and that, barring SA, specific criteria or qualifications for the practice of neuropsychology in Africa are lacking. A consequence of this lack of clarity and the scarcity of neuropsychologists is that other allied health professionals (e.g., neurologists or psychiatrists) may fulfill these roles without adequate neuropsychological training.
Only one previous survey related to neuropsychology in Africa was identified. Truter et al. (Reference Truter, Mazabow, Morlett Paredes, Rivera and Arango-Lasprilla2018) included SA in an online international survey of neuropsychological training, assessment, rehabilitation, and research in 30 countries from North America, Latin America, Europe, and Scandinavia. No other country in Africa was surveyed, underscoring the dearth of available information.
To gain information that may bolster the development of neuropsychology in Africa, the International Neuropsychological Society (INS) Justice and Equity Subcommittee initiated a survey of neuropsychological academic programs, clinical practices, and research throughout the continent. The current paper reports the results of this survey and their implications for the continued development of neuropsychology in Africa.
Study aim
This study aimed to survey neuropsychological academic programs, clinical practices, and research from individuals at academic institutions of higher education across Africa.
Method
Research design and setting
This study is quantitative and cross-sectional. We utilized chain referral, or snowball sampling of potential participants at institutions of higher education across Africa for this survey-based study.
Participants
Participants for this study were sampled from academic institutions of higher education across Africa.
The strategy to identify potential survey participants in each of the countries in Africa (N = 54) was implemented to locate individuals with a high likelihood of familiarity with their countries’ neuropsychological resources through their institutional affiliations. First, uniRank, a search engine and international directory of higher education institutions, was used to identify such institutions in each country. It has compiled rankings, program and course offerings, and admissions information for >13,000 institutions globally. After identifying 1244 academic institutions in Africa, Google search engine research was conducted to find each university’s official website. Next, institution websites were reviewed to identify psychology or psychiatry departments or course offerings related to psychology. Of the 1244 institutions, 759 made no mention of such programming and were excluded. Of the remaining 485 programs, it was unclear whether 244 of them had psychology or psychiatric-related programming; however, we were able to obtain a general institutional contact email from their website for 36 of these programs, with the remaining 208 programs excluded from further contact. In contrast, 241 programs specified some level of psychology or psychiatry programming, such as departments, degree programs, or individual courses. An attempt was made to identify email contacts for faculty or department leadership associated with these psychology or psychiatry program offerings, or a general department contact if a more specific contact was not found. In cases where we could not locate specific contacts or a departmental email address, we used the general university one.
Most programs had more than one contact listed. The introductory email was sent to 608 potential participants who either completed the survey or forwarded it to the appropriate colleague, or did not respond. Reminder emails were sent to 429 of the initial contacts, but not to those contacts with known bounce backs, those who had already responded, or those who were recently contacted. In addition to the 608 initial emails sent, chain referrals from colleagues of the initial contacts yielded another 68 contacts who received individual invitations to participate and a link to access the survey. In sum, the survey was distributed to 676 potential participants representing 46 countries in Africa.
Measures
The study survey was designed to obtain information about the neuropsychological academic training and education programs, clinical practices, and research in as many of the 54 countries of the African continent as possible, as well as the respondents’ interest in developing collaborations and perspective on what resources were needed to continue advancing the field of neuropsychology.
The survey was designed to take approximately 20 min to complete and consisted of five parts. Part 1 collected information about the respondent’s professional background, and part 2 asked questions about academic programs in the respondent’s country. Part 3 collected information about neuropsychological clinical practice and related services available in the country. Part 4 asked about areas of ongoing and needed neuropsychological research and the resources and infrastructure available to support research. Finally, part 5 requested information on how the further development of neuropsychology could be supported in the country. The majority of questions used a multiple-choice or rank order structure, but each part of the survey included free-text fields in which respondents could elaborate or explain their answers or enter additional information.
Procedure
A cover letter outlining the purpose of the survey, background of study leaders, and a request to provide the names and contact emails of any faculty/staff at the participating institution teaching or practicing in psychology-related fields was sent to prospective participants. The letter and survey were written in English and translated into Swahili, Arabic, French, Portuguese, and Spanish. Translations were conducted by neuropsychologists fluent in the target language. The cover letter contained a link to the online study survey, administered on the Qualtrics Survey Platform (www.qualtrics.com), which was also available through a drop-down menu in the noted languages.
Analyses
After data cleaning, descriptive statistics were applied to summarize the data, which were either tabulated or presented graphically. Some open-ended responses were analyzed using basic content analysis (Weber, Reference Weber1990).
Results
Part 1: Survey participants
There were N = 42 respondents to the survey. Surveys were returned from 17 of the 54 countries in Africa (±31.5% country response rate; see Figure 1). The number of respondents differed across the continent, with the largest number being in Kenya (8), and Egypt, Ghana, Uganda, Zambia, Zimbabwe, and South Africa having 3–5 respondents each. Seven surveys, however, were incomplete (five respondents completed 44% of the survey, one each from Sudan, Nigeria, Egypt, Kenya, and Zambia). Additionally, one respondent from Egypt completed 40% of the survey, and one respondent from South Africa completed 29% of the survey. Hence, across the categories, there were, on average, approximately 7–9 responses that were incomplete (range: 7–13), and the data shown is therefore for respondents who completed particular questions only. Where necessary, the breakdown of missing data is provided. Most surveys were completed in English (n = 37), with three completed in French and two in Arabic. No surveys were completed in Swahili, Spanish, or Portuguese.
Distribution by country of respondents (N = 42).

Table 1 summarizes the professional identification and highest degrees obtained by survey respondents. The majority identified as psychologists (clinical and neuropsychologists), with one psychiatrist and three neurologists also completing the survey. Most respondents had earned doctoral degrees, with just over a quarter of the sample (26.2%) reporting their highest degree was at the master’s level. Respondents averaged 8.4 years (SD = 5.7, range = 3–16) of experience in their respective professions.
Descriptives: respondent profession and highest academic degree obtained (N = 42)

Note: This table shows the distribution of professions and academic degrees among the survey respondents. “Other Psychology” included educational psychology (6), counseling psychology (5), research psychology, and cognitive psychology. “Other” included professor and psychological health. “Other” included an associate professor regarding the highest degree earned.
Part 2: Information related to clinical practice
Number of neuropsychologists per country
Figure 2 shows respondents’ estimates of how many people specifically identify themselves as neuropsychologists in their country, across the categories 0, 1–5, 6–10, 11–20, and >20. Most respondents estimated that there are about 1–5 (20/35, 57.14%), and respondents from Kenya, South Africa, Tunisia, and Zambia provided estimates of 20 or more. The figure reflects the average responses across respondents from each country. Respondents from the following countries reported disparate responses for the same country: Ethiopia, Kenya, and Zimbabwe (see Figure 2).
Estimated number of neuropsychologists in each country (N = 35*).
Note. This figure shows the distribution of responses for the number of neuropsychologists in each respondent’s country. Each value displayed is the frequency of responses taken for the categories listed. Green indicates that neuropsychologists were reported to be present in the country, while red indicates that none were reported. Darker colors indicate a higher frequency of response. *Seven participants did not respond (1 from Sudan, South Africa, Nigeria, Kenya, Zambia; 2 from Egypt). Sudan was therefore not represented.

Estimated number of neurologists, psychiatrists/neuropsychiatrists, and clinical psychologists
Figure 3 shows the estimated numbers of neurologists, psychiatrists/neuropsychiatrists, and clinical psychologists in each country. In terms of neurologists, respondents from Cameroon, Egypt, Morocco, South Africa, Tunisia, and two respondents from Zambia estimate 20 or more in their countries, while the respondent from Nigeria and one respondent from Zambia reported zero such professionals in their country. Regarding the estimated number of psychiatrists/neuropsychiatrists in each of the respondent’s countries, respondents from more than half of the countries represented (Egypt, Ethiopia, Kenya, Morocco, Nigeria, South Africa, Tunisia, Uganda, and one respondent from Zambia), estimated 20 or more, while no respondents reported an absence of such professionals in their countries. Last, regarding clinical psychologists, respondents from nine countries (Cameroon, Ghana, Kenya, Nigeria, Rwanda, South Africa, Tunisia, Uganda, Zambia) reported 20 or more in their countries, while only one respondent (Egypt) reported zero such professionals in their country.
Estimated (median) number of clinical psychologists (N = 35), psychiatrists/Neuropsychiatrists (N = 34), neurologists (N = 35).
Note. This table shows the median response for the number of clinical psychologists, psychiatrists/neuropsychiatrists, and neurologists in each country. *Seven participants did not respond for each measure (Sudan, Egypt (2), South Africa, Nigeria, Kenya, Zambia), and the number of psychiatrists/neuropsychiatrists was additionally not reported for Zimbabwe. Sudan was not represented.

Important activities performed by neuropsychologists
Regarding activities performed by neuropsychologists, Figure 4 shows that conducting assessments of cognitive function, carrying out research, and teaching in neuropsychology, as well as assisting with neurological diagnoses, are among the most cited activities.
Activities performed by neuropsychologists across countries (N = 35*).
Note. This figure shows the activities most often performed by neuropsychologists according to the respondents. “Other” included assisting in awake neurosurgery, and the other two related to a lack of services and the fact that the respondent was estimating. *Ten participants did not respond (Sudan, Egypt (3), Ethiopia, South Africa, Zimbabwe, Nigeria, Kenya, Zambia). Sudan and Egypt were not represented.

Tools used to assess neuropsychological disorders
The most commonly cited instruments to assess neuropsychological status (Figure 5) were the patient clinical interview and standardized tests developed outside of Africa. Interestingly, the fewest number of respondents reported using locally developed tests or norms.
Tools used to assess neuropsychological disorders (N = 34*).
Note. *Eight participants did not respond (Sudan, Egypt (2), Ethiopia, South Africa, Nigeria, Kenya, Zambia). Sudan was not represented.

Other professionals who administer neuropsychological tests
When asked what professionals would likely administer neuropsychological tests if they were available, most respondents (N = 35) indicated psychologists (24/35; ±69%), psychiatrists (23/35; ±66%), and neurologists (18/35; ±51%). Other professionals mentioned less frequently were nurses or nurse aids (7/35; 20%), physicians (4/35; ±11%), teachers (5/35; ±14%), and social workers (4/35; ±11%). One participant also indicated occupational therapists.
Diagnostic tests/Neuroimaging use in the respondents’ countries
Figure 6 (a–d) reports on diagnostic test/neuroimaging use in the respondents’ countries. The graphs a-d (from left to right in each row) depict the use of electroencephalogram (EEG), computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET) technology as reported by respondents from each of the 17 countries represented in the survey. Respondents from 14/17 reported EEG use, 13/17 countries reported CT use, 15/17 reported MRI use, and 5/17 reported PET use. Note, however, that responses from Egypt and Sudan in particular were impacted by the non-completion of the survey.
Neuroimaging and electrophysiology use reported by respondents across countries.
Note. The figures show in which countries participants indicated having each type of testing available. *Sudan was not represented.

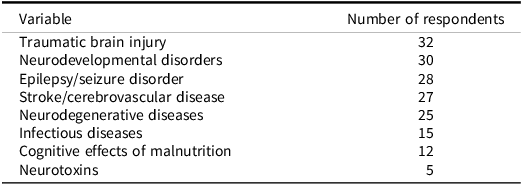
Neurological populations that would benefit most from neuropsychological care
Across the sample, respondents ranked individuals who have sustained TBIs, those who are diagnosed with neurodevelopmental disorders, and those with epilepsy/seizure disorders as being the neurological populations that would benefit the most from neuropsychological care (Table 2). An additional response of “accident victims” likely also refers to TBI.
Neurological populations that would benefit most from neuropsychological care (N = 35*)

Note: This table shows the populations that were indicated as benefiting from neuropsychological care.
* Seven respondents did not answer (Sudan, Egypt (2), South Africa, Nigeria, Kenya, Zambia).
Age groups most in need of neuropsychological services
Regarding age groups most in need of neuropsychological services, respondents (N = 29) ranked groups according to those they reported to need services the most, to those that need such services the least. Children aged 5–12 and adults older than 60 years were ranked as most in need overall, followed by other pediatric groups (preschool and adolescent groups), with adults under 60 ranked as least in need relative to the other groups (including preschool children and adolescents). For this survey question, Rwanda, DR Congo, and Sudan were not represented.
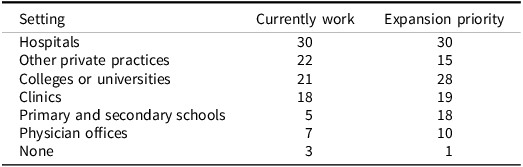
Settings where neuropsychologists work and expansion priorities
Neuropsychologists were reported to work most frequently in hospitals, private practices, colleges/universities, and clinics. Notably, while priorities for expanding or developing neuropsychological work largely paralleled these locations, many also expressed the need to develop services in primary and secondary schools (Table 3).
Where neuropsychologists work and expansion priorities (N = 34*)

Note: This table shows the setting in which neuropsychologists currently work and where respondents indicated there should be a priority for expansion of neuropsychology.
* Eight participants did not respond (Sudan, Egypt (2), South Africa, Zimbabwe, Nigeria, Kenya, Zambia). One of these eight (Zimbabwe) provided responses for expansion priorities. Sudan was not represented.
Part 3: Research
Neuropsychological research in the respondents’ countries
The majority of respondents (74%) affirmed having neuropsychological research in their country. The countries where at least one respondent in the country indicated research activity included: Botswana, Cameroon, DR Congo, Egypt, Ghana, Kenya, Morocco, Sierra Leone, South Africa, Tunisia, Uganda, Zambia, and Zimbabwe. Regarding international neuropsychological research collaborations, a little less than half of respondents (49%) reported engaging in international collaborations. Countries with the most international collaborations were Kenya (n = 3) and Uganda (n = 4) (Figure 7).
Areas where neuropsychological research is currently underway (N = 29) and needed (N = 32).
Note. Ten participants did not respond for needed areas of research (Egypt (2), Ethiopia, Kenya, Nigeria (2), South Africa (2), Sudan, Zambia). Sudan and Nigeria were not represented. Thirteen participants did not report areas of research currently underway (Egypt (2), Ethiopia (2), Ghana, Kenya (2), Nigeria (2), South Africa, Sudan, Zambia, Zimbabwe). Sudan, Ethiopia, and Nigeria were not represented. Respondents were asked to select multiple responses, up to 5.

Areas of neuropsychological research currently underway and needed
Respondents were asked to select up to 5 areas of neuropsychological research that are currently underway in their respective countries. As summarized in Figure 8, the top three areas of current research activity were on the neuropsychological effects of psychiatric disorders such as depression and post-traumatic stress disorder, closely followed by neuropsychological impacts of infectious diseases (e.g., HIV, COVID-19, and cerebral malaria), and neurodevelopmental disorders. Minimal research is being conducted on the neuropsychological consequences of metabolic disorders and neurotoxins. According to respondents, there is also little research activity on the applications of neuropsychology in courts of law and public health.
Common research funding sources (N = 32).
Note. “Other” included self-financing and minimal (‘not much’) financing. *Ten participants did not respond (Ethiopia (2), Sudan, Egypt (2), South Africa, Nigeria (2), Kenya, Zambia). Sudan, Ethiopia, and Nigeria were not represented.

Respondents were also asked to select up to 5 areas in which neuropsychological research is needed. Of note, even though most research activity is directed to psychiatric disorders, infectious diseases, and neurodevelopmental disorders (see Figure 7), these same areas of research are highlighted as needing the most research. Research on neurodegenerative disorders, TBI, rehabilitation, and public health are further recognized by respondents as a priority.
Sources of research funding
Regarding the common sources of research funding, Figure 8 shows that respondents cited private or government grants from other countries and international partnerships as the most common funding sources. Funding from non-governmental organizations, national grants, and local institutions were less common, and self-financing and minimal (or a lack of) financing were very rare.
Utility of support from the International Neuropsychological Society for the development of neuropsychology
Regarding whether there would be interest in support from the INS for the development of neuropsychology in the respondents’ country, 34/42 (±81%) of respondents indicated strong interest in all categories of support priorities from INS, with all areas endorsed at 2.8/3 or higher: Financial support for INS membership and INS conference attendance, in person symposia, short courses, full courses in neuropsychology, support for academic and clinical infrastructure development, opportunities to collaborate with other neuropsychologists, neuropsychological tests, online courses, access to recorded interviews or discussions, clinical supervision, research mentoring, and books.
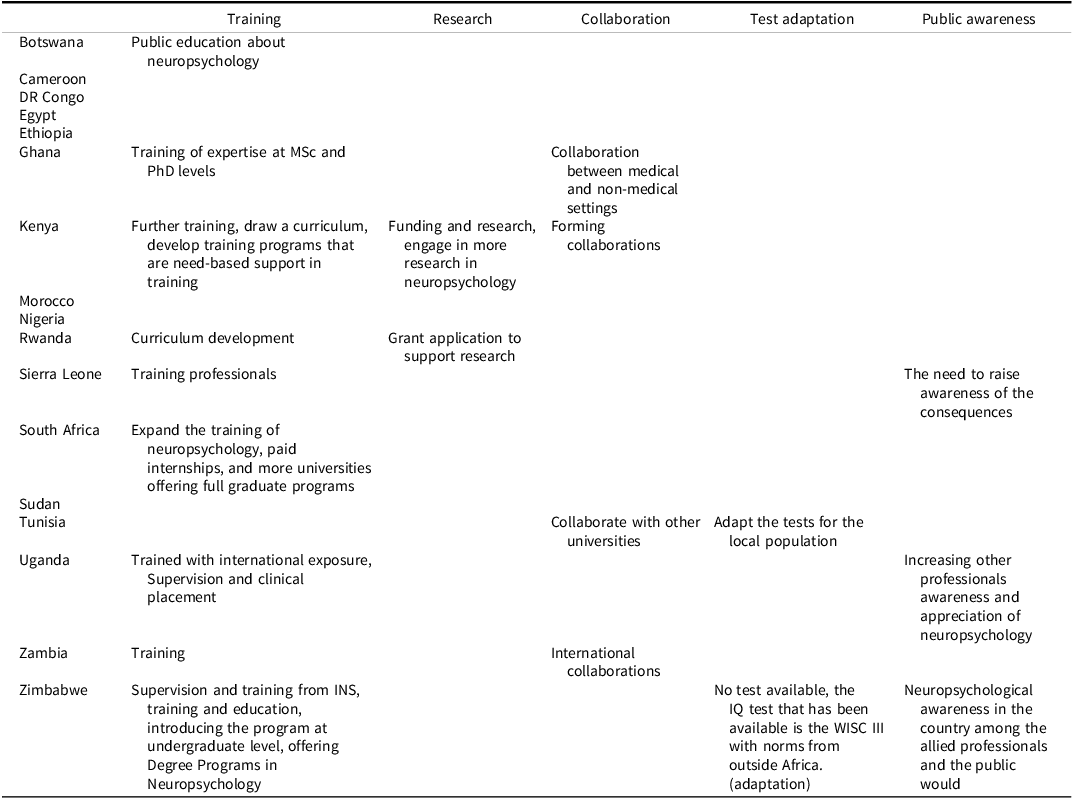
Next steps in neuropsychology development
Table 4 shows respondents’ perspectives (based on common responses provided by participants) of what the next steps to develop neuropsychology are, with training in neuropsychology and related responses reported by most participants who responded to this survey question, followed by collaboration and greater public awareness.
Next step in neuropsychology development from respondents’ perspective (N = 28)

Part 4: Education
Education programs available in respondents’ countries
Education programs available in respondents’ countries (see Figure 9) range from individual courses in neuropsychology to formal undergraduate (bachelor’s degrees) to postgraduate qualifications (master’s and PhD), either in neuropsychology specifically or in clinical psychology with relevant coursework in neuropsychology. In countries where there were multiple respondents, there were often disparate responses in terms of the types of educational programs available, except in SA, where all respondents agreed that the training for neuropsychology occurred in Master’s degree programs. All respondents from Botswana, DR Congo, Ethiopia, and Rwanda, who completed this question reported no educational programs in neuropsychology in their respective countries.
Educational programs in neuropsychology available in respondents’ country (N = 41).
Note. Green shading indicates that at least one respondent from the country indicated that the program was available in their country. Missing data: Sudan not represented in table; NP: neuropsychology. “Other” responses included: teaching neuropsychology at the undergraduate level to students of the psychology program (Egypt); bachelors, master’s degree, and PhD in counseling psychology (Kenya), BSc in Clinical Counseling/Psychology (Sierra Leone), un master professionnel en neuropsychologie clinique avec cours et stage en neuropsychologie clinique; un programme de master en neuropsychologie clinique avec cours et stage en neuropsychologie (Tunisia); Bachelor’s and Master’s degree in Psychology with Neuropsychology Course Units, and a PhD by research that can be in Neuropsychology (Uganda).

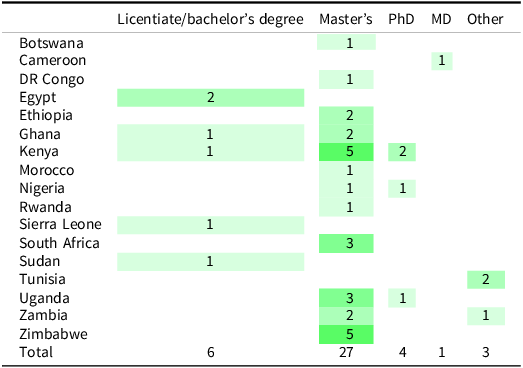
Minimum university/college degree required to practice neuropsychology
Table 5 shows that a Master’s degree is reported to be the minimum requirement by±66% of respondents (71% if one includes the two Other responses from Tunisia). Respondents from Egypt, Sierra Leone, and Sudan reported the minimum requirement to be a licentiate/bachelor’s degree.
Minimum university/college degree required to practice neuropsychology in respondents’ country of work (N = 41)

Note: One missing response (Egypt); MD: medical doctor. Responses coded as “Other” included master professional (n = 2; Tunisia) and “I don’t know” (n = 1; Zimbabwe).
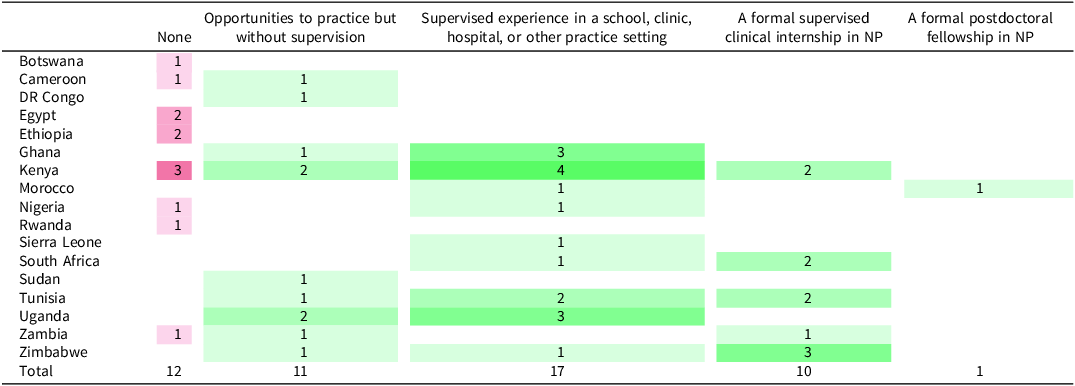
Clinical training in neuropsychology in respondents’ countries
Table 6 shows that 42.5% of respondents reported supervised experience in a school, clinic, hospital, or other practice setting, 27.5% of respondents reported opportunities to practice but without supervision, while 25% of respondents reported that a formal supervised clinical internship in neuropsychology exists in their country. Respondents from Botswana, Egypt, Ethiopia, and Rwanda, however, reported that there are no such clinical training opportunities in their countries, while a respondent from only one country, Morocco, reported a formal postdoctoral fellowship in neuropsychology.
Clinical training available in neuropsychology in respondents’ country (N = 40)

Green indicates that opportunities were reported to be available in the country, while red indicates that none were reported. Darker colors indicate a higher frequency of response.
Note: Two missing responses (Egypt and South Africa); multiple responses allowed per respondent.
Opportunities for regular case discussions/Continuous education
Regarding whether there is opportunity to regularly discuss neuropsychological cases with colleagues for the purpose of continuing education, 17/39 respondents (±44%) said yes, 22 (±56%) said no, and responses were missing for 3 participants. Respondents who said yes worked in 13 different countries (all countries presented except Cameroon, Ghana, Rwanda, and Sierra Leone).
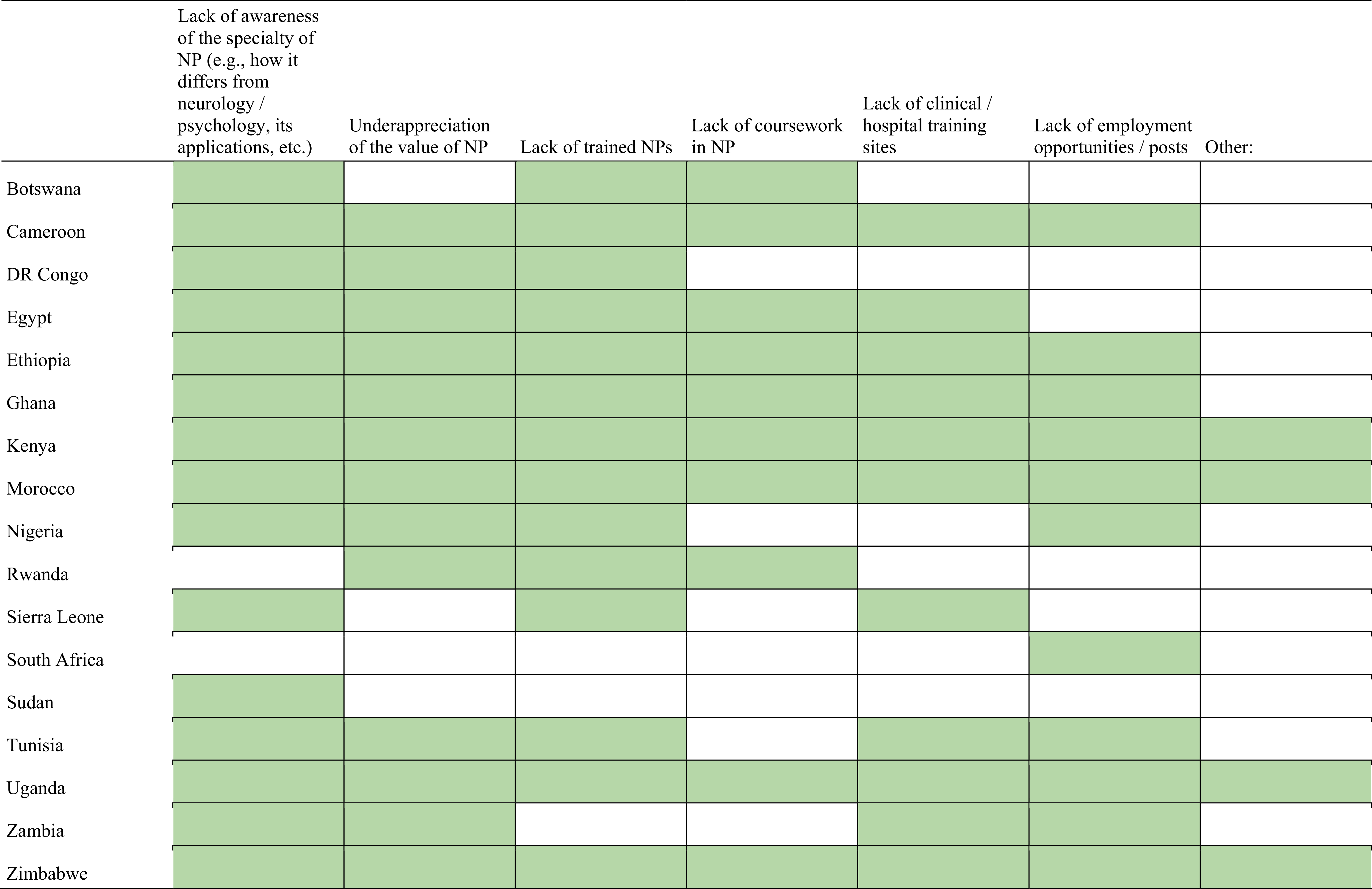
Greatest challenges to further developing the academic study of neuropsychology
Finally, respondents reported several challenges to developing academic programs in neuropsychology (Figure 10), including lack of trained neuropsychologists (±85%), a lack of awareness of the specialty (e.g., how it differs from neurology/psychology, its applications, etc.; ±69%), an underappreciation of the value of the specialty (56.4%), a lack of employment opportunities (54%) and clinical/hospital training sites (44%), and a lack of coursework in neuropsychology (38.4%).
Greatest challenges to further developing the academic study of neuropsychology in respondents’ countries (N = 39).
Note. Green indicates that at least one respondent indicated the challenge as a challenge in their country. Three missing responses (Egypt, South Africa, and Zambia); one “Other” response from Egypt (كل ما سبق) translated to “and all of the above” – other columns checked; remaining responses for other column included: finances/funding, lack of neuropsychological tests in Arabic, lack of relevant equipment and neuropsychological assessment tools; lack of tests – individually purchasing them is expensive, lack of textbooks, lack of neuropsychological tests; lack of material resources.

Discussion
This survey represents the first systematic attempt to delineate the neuropsychology clinical practice, research, and education on the African continent. Survey respondents represented a third of the countries on the continent, and were primarily clinical psychologists and neuropsychologists. Most had earned a doctorate (69%) or master’s (26%) degree, and respondents had an average of 8 years of experience. Educational opportunities varied across countries. In some places, there were no educational programs or only individual (presumably non-degree) undergraduate and postgraduate courses. The most common programs were a master’s level clinical psychology degree, with coursework or clinical internship in neuropsychology (32% of respondents), and in line with this, most respondents (66%) reported a master’s degree was the minimum requirement to practice neuropsychology. However, respondents from Egypt, Sierra Leone, and Sudan reported the minimum degree to be a Licentiate/Bachelor’s Degree.
Barriers to the development of neuropsychology in Africa
Careful, strategic investments are needed to overcome the many challenges to the development of neuropsychology on the continent that were raised. These center on five primary areas. First, at the most basic level, some countries reported an absence of educational programs providing instruction in neuropsychology. Beyond academic instruction, limited access to clinical training sites and qualified neuropsychological mentors for clinical training and/or research is a formidable challenge for many African countries at this time. For example, with only about a third of respondents reporting the availability of supervised clinical experience in school, clinic, hospital, or other practice settings, and only a single instance of postdoctoral training, many have no practical and supervised training in diagnosis, research, or rehabilitation. Respondents also noted a lack of awareness of the value of the speciality. A third related challenge is the paucity of neuropsychologists in current practice. While results suggest that there may be more than 20 practicing in Kenya, South Africa, Tunisia, and Zambia, most countries reported having fewer than 5. This is astounding in light of the populations and geographies of these countries, underscoring the incredible demand that would be placed on any few experts there to lead in clinical care, training, and research. African neuropsychologists mainly work in hospitals, private practices, and colleges or universities, and all these settings could reportedly benefit from the expansion of opportunities for neuropsychologists. A fourth daunting challenge to the development of neuropsychology is the lack of validated, standardized, culturally relevant neuropsychological measures. Instead, most respondents indicate the use of patient clinical interviews and standardized tests developed outside of Africa. The importance of locally developed/adapted and normed tests to avoid misinterpretation of outcomes has long and consistently been reported in the literature (Ferrett et al., Reference Ferrett, Thomas, Tapert, Carey, Conradie, Cuzen, Stein and Fein2014; Shuttleworth-Edwards & Truter, Reference Shuttleworth-Edwards and Truter2023). And finally, the limited availability of diagnostic neuroimaging techniques also often reflects the nascent development of the neurosciences in many African countries. This, too, introduces challenges to teaching, research, and clinical care.
These five challenges, specifically access to educational instruction, mentors, training sites, instrumentation, and neuroscience infrastructure, are formidable, but not insurmountable. Ponsford’s (Reference Ponsford2017) review of the development of neuropsychology illustrated the advanced development of the field in North America, Europe, and Australia, the emerging structure of the field in South America, Asia, and the Middle East, and the newer indications of science and practice in Africa. Since that time, opportunities across science, practice, and education have systematically grown, but clearly require continued investment and commitment.
Opportunities for the development of neuropsychology in Africa
We are aware of sparks of scholarly development in several countries. The investments that are needed to truly develop the field of neuropsychology on the African continent range from small to large, with each strengthening the emerging web of collaborations that can yield a strong network of clinical training and research centers. Examples of small, but meaningful contributions would include offering educational courses or presentations, in person or via virtual modalities, at little or no cost to students in neuroscience adjacent fields, sponsoring conference attendance, or donating test kits and supplies of instruments that have been locally validated. Examples of medium and notable investments would be to sponsor and facilitate graduate PhD training (and associated visa sponsorship) in countries with the necessary local infrastructure, being mindful of any limitations to the recognition of coursework or supervised experience in the home country; to fund and partner with African colleagues to develop neuropsychological research protocols to advance local neuropsychological research, which not only lead to scientific discovery, but also foster local instrument validation and opportunities for developing scholars (e.g., research in cerebral malaria; Bangirana et al., Reference Bangirana, Opoka, Boivin, Idro, Hodges and John2016; interventions in brain health at the Brain Mind Institute at The Aga Khan University (2025), with a campus in East Africa). Large investments would be to secure resources, through any combination of philanthropy, government funding, and research grants, to establish graduate programs within African university settings. Such programs should be built from the onset with the goal of becoming independently self-sustaining after an initial period where both African and external experts and mentors collaborate with local leadership to build the program. An example of such a comprehensive effort to develop neuropsychology involves a program that was recently seeded at the University of Rwanda, the Neuroscience Expertise through US-Africa partnership: NEXUS program, which is an NIH D43-funded training program designed to establish a program in brain health (PI: DK). Central to NEXUS is the training of eight PhD clinical psychologists with a concentration in neuropsychology. Pillars of the program involve (1) instrument development, validation, and standardization; (2) foundational instruction including functional neuroanatomy, lifespan assessment methods, research methods, disorders of the nervous system, and neurorehabilitation; (3) practical clinical training; and (4) neuropsychological research. Further, local initiatives, such as the African Neuropsychology Network, which includes INS Global Engagement Committee regional representatives from Africa and other neuropsychology scholars from across the continent, can serve to foster collaborations and educational efforts across academic institutions locally.
Not surprisingly, our findings related to current research activities largely parallel recent publications on the continent (e.g., Aderinto et al., Reference Aderinto, Alare, AbdulBasit, Edun and Ogunleke2023; Schoeman et al., Reference Schoeman, Carey and Seedat2009; Segre et al., Reference Segre, Cargnelutti, Bersani, Njogu, Roberti, Campi, De Vita, Morino, Canevini and Bonati2023), with the top three focus areas of infectious disease (e.g., HIV, COVID-19), neurodevelopmental disorders, and the neuropsychological effects of psychiatric disorders (e.g., depression, post-traumatic stress disorder). Research on TBI and neurodegenerative disorders was also reported by a third or more of respondents, also in line with local research (e.g., Adegboyega et al., Reference Adegboyega, Zolo, Sebopelo, Dalle, Dada, Mbangtang, Tetinou, Kanmounye and Alalade2021; Onohuean et al., Reference Onohuean, Akiyode, Akiyode, Igbinoba and Alagbonsi2022). There is a clear interest in opportunities to collaborate nationally and internationally to build capacity. The reported interest in building future services for individuals who have sustained TBIs, those with neurodevelopmental disorders, and those with epilepsy maps onto the populations reported to be most in need of services, i.e., school-aged children and adults over 60 years.
Future directions for African neuropsychology development
Stemming from the barriers and opportunities identified above, work is needed to educate the public in African countries on the applications and benefits of neuropsychology and to develop academic and clinical training opportunities for clinicians and researchers. In doing so, the importance and quality of supervision in the training of neuropsychologists cannot be underscored enough and present an important area for future development (Ferreira-Correia, Reference Ferreira-Correia2017; Stucky et al., Reference Stucky, Bush and Donders2010). Third, research is needed to develop, adapt, standardize, and establish normative standards for tools designed specifically for Africa. The support needed for the development of neuropsychology includes specialty-level coursework (including online courses), culturally appropriate neuropsychological instruments normed for use in Africa, and opportunities for international collaboration.
In line with this, there was high respondent endorsement (81%) in the survey of the need for INS support, indicating several potential areas of individual and organizational advocacy. The findings from this study clearly indicate opportunities for INS to prioritize the development of the field in Africa. This clearly aligns with the mission of the INS Global Engagement Committee to develop neuropsychology in areas where it is least available and most needed. Support in the form of scholarships and travel awards, such as those offered by the INS Science Committee, was requested. This research aligns with other reports reflecting the neurosciences as nascent, but emerging, and much-needed disciplines (Abd-Allah et al., Reference Abd-Allah, Kissani, William, Oraby, Moustafa, Shaker, El-Tamawy and Shakir2016; GBD 2021 Nervous System Disorders Collaborators*, 2024).
While many organizations, including INS, offer tiered membership dues, the cost of societal membership and travel to meetings held outside of the continent is often daunting relative to annual incomes in LMICs. Here, too, there may be an opportunity to re-evaluate if and how waivers could be implemented relative to earnings, augmenting the feasibility of conference attendance, learning, and collaboration. Such discussions could be taken up with the INS Membership Engagement Committee, who engage in outreach and strengthening INS member experiences.
A further recommendation for future research is to consider the interpretations of such findings within frameworks such as the Theoretical Domains Framework (Atkins et al., Reference Atkins, Francis, Islam, O’Connor, Patey, Ivers, Foy, Duncan, Colquhoun, Grimshaw, Lawton and Michie2017) and the Consolidated Framework for Implementation Research (Damschroder et al., Reference Damschroder, Reardon, Widerquist and Lowery2022). Use of such frameworks for implementation science was beyond the scope of our paper as this was not our objective when we designed the survey. However, these frameworks might be used in the future to identify the antecedents for the required systemic changes to both current and targeted behaviors, to guide the development of the field in Africa. Practically, such inquiry and implementation would need to be country- and even institution-specific to be effective, as a continent-wide strategy would not be appropriate given the known variation in the development of neuropsychology and readiness for education and training programs by country. Last, understanding the registration requirements for psychology practice in African countries, and governance or regulation of health professionals, while noting the variation of regulatory bodies and standards across the continent, is also an important aspect that would be helpful to guide recommendations for next steps. The rich diversity in culture, language, and healthcare and educational infrastructure underscores the need for thoughtful, tailored approaches.
Study limitations
A major limitation of this study was that there were responses from only a third of African countries, limiting generalizability of results beyond the countries from which surveys were returned. However, the response rate can be considered a strong beginning when considering that neuropsychology is a highly specialized field of practice and research. In addition to the current state of slow development of the field in Africa (Kissani & Naji, Reference Kissani and Naji2020), the response rate may also have been impacted by developing infrastructure, making identification of the people with the most relevant knowledge challenging (e.g., academic settings with little or no internet presence). Additionally, survey fatigue may have impacted engagement, as a function of multiple surveys on other topics in Africa, which has been observed in other disciplines (de Koning et al., Reference de Koning, Egiz, Kotecha, Ciuculete, Ooi, Bankole, Erhabor, Higginbotham, Khan, Dalle, Sichimba, Bandyopadhyay and Kanmounye2021). Third, our survey response rate, which we report transparently, seems to be in keeping with the results of a systematic review of survey research in neuropsychology (Marcopulos et al., Reference Marcopulos, Guterbock and Matusz2020). Their findings show that almost 24% of the studies reviewed did not report a response rate, and among those that did, these ranged from 9.7 to 98%. These authors report a general trend in lower response rates to neuropsychology-based surveys over time, which could be attributable to a move toward more online surveys. Research has shown that online surveys result in poorer response rates than paper-based or traditional surveys (Wu et al., Reference Wu, Zhao and Fils-Aime2022) and that the growth of the profession may create greater diffusion of responsibility and diminish the sense of connection that could encourage participation, at least for some (Marcopulos et al., Reference Marcopulos, Guterbock and Matusz2020). Fourth, we acknowledge that professionals from one discipline may have limited knowledge of the number of professionals in another, and we interpret the relevant outcomes cautiously. Last, we acknowledge that the results reported in Tables 5 and 6 show widely differing views on the minimum level of education required to practice neuropsychology and on current training available in many countries. These disparities highlight a lack of consensus, indicating the need for regional discussions that consider varied and emerging regulations across countries.
Conclusion
The current study demonstrates the need for a greater focus on developing neuropsychology in LMICs like those in Africa (Hamadeh et al., Reference Hamadeh, Van Rompaey and Metreau2023), where development has been slower than in other LMIC settings (Kissani & Naji, Reference Kissani and Naji2020), especially given the heavy burden of neurological disease on the continent. The results of the survey demonstrate the need for accelerated development of neuropsychology, and more broadly, the neurosciences, in Africa (Besharati & Akinyemi, Reference Besharati and Akinyemi2023).
Long term aims (significance)
-
1. Identify inequities in neuropsychological diagnosis, treatment, prevention, research, education, and training that impact brain health internationally.
-
2. Develop culturally appropriate, international collaborative initiatives to assess and address these inequities.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1355617725101756.
Funding statement
We appreciate the support of the former INS Justice and Equity subcommittee members during the inception of the survey, as well as the seed funding provided by INS in support of the initiation of data collection.
Competing interests
None.
Ethical standards
The research was completed in accordance with the Helsinki Declaration. This study was approved by the Institutional Review Board of Duke University Health System (Protocol 00109602). An introductory page to the survey explained the purpose and voluntary nature of the study, and consent was indicated by proceeding to the survey.













 Open access
Open access