


Metabolic dysfunction-associated steatotic liver disease (MASLD), recently redefined from non-alcoholic fatty liver disease(Reference Rinella, Lazarus and Ratziu1), is the leading chronic liver disease worldwide. The number of patients with MASLD doubled from 24 million in 1990 to 48 million in 2021(Reference Gu, Guo and Liu2). Beyond predisposing to liver fibrosis, cirrhosis and hepatocellular carcinoma, MASLD independently increases the risks of cardiovascular events, type 2 diabetes and all-cause mortality(Reference Targher, Byrne and Tilg3–Reference Liu, Zhong and Tan5), adding substantially to global disease burden(Reference Younossi, Golabi and Paik6).
Among modifiable exposures, dietary fat composition(Reference Hassani Zadeh, Mansoori and Hosseinzadeh7) is an important determinant of MASLD(Reference Hernández, Kahl and Seelig8,Reference Valibeygi, Davoodi and Dehghan9) . SFA have been strongly associated with MASLD(Reference Luukkonen, Sädevirta and Zhou10). Mechanistically, high SFA intake augments lipogenesis, oxidative stress and mitochondrial dysfunction(Reference Meex and Blaak11–Reference Rosqvist, Kullberg and Ståhlman13) – processes that may contribute to MASLD development. SFA are conventionally categorised by chain length as long-chain fatty acids (LCFA; e.g. C14:0, C16:0, C18:0), medium-chain fatty acids (MCFA; e.g. C8:0, C10:0, C12:0) and short-chain fatty acids (SCFA; e.g. C4:0, C6:0), with varying metabolic effects. LCFA, particularly the predominant dietary forms palmitic acid (C16:0) and stearic acid (C18:0), are consistently linked to hepatic steatosis and metabolic stress(Reference Senanayake, Hapugaswatta and Samarawickrama14–Reference Shen, Miao and Zhang17). In contrast, MCFA and SCFA may exhibit lower lipotoxicity or even anti-inflammatory properties in selected contexts(Reference Gao, Yao and Meng18,Reference Huang, Gao and Chen19) , although effects may depend on individual metabolic milieu, intake levels and target tissues. Moreover, most epidemiological studies have examined only total SFA intake, overlooking the potential adverse effects of individual SFA and their combined impacts on MASLD risk. Therefore, modern mixture analyses are required to clarify the joint effects of SFA profiles on MASLD.
Beyond dietary patterns, MASLD development involves metabolic and inflammatory processes. Insulin resistance (IR) impairs hepatic glucose utilisation and stimulates lipolysis and hepatic lipogenesis, thereby promoting lipid accumulation and liver injury(Reference Fujii and Kawada20,Reference Palma, Pronio and Romeo21) . Notably, SFA can induce IR by disrupting insulin signalling and glucose/lipid metabolism(Reference Min, Yang and Lee22). Serum albumin, an abundant plasma protein with antioxidant and anti-inflammatory properties(Reference Arroyo, García-Martinez and Salvatella23,Reference Sitar, Aydin and Cakatay24) , declines in proportion to systemic inflammation, oxidative stress(Reference Sheinenzon, Shehadeh and Michelis25,Reference Kinoshita, Watanabe and Azma26) and impaired hepatocellular synthetic capacity(Reference Czaja27). Lower serum albumin is increasingly recognised as a biomarker of MASLD(Reference Sun, Wang and Liu28,Reference Kawaguchi, Sakai and Terashima29) . Although previous literature has confirmed the associations of IR and albumin levels with MASLD, their roles as potential mediators of the relationship between dietary fatty acids and MASLD remain untested.
Using nationally representative data from multiple cycles of National Health and Nutrition Examination Survey (NHANES), we examined the independent associations of individual SFA with MASLD, assessed the joint effect of the SFA mixture and explored the potential mediating pathways involving IR and serum albumin.
Research methods
Study population
NHANES is an ongoing survey focused on the nutrition and health of the US population. This study used seven NHANES cycles between 2005 and 2018 and was conducted as a cross-sectional analysis. The survey protocols were approved by the CDC Institutional Review Board and followed guidelines protecting the safety and privacy of human subjects, complying with the STROBE statement. All participants provided informed consent. From an initial pool of 70 190 participants, we excluded (1) participants aged < 20 years, (2) viral hepatitis carriers (positive HBsAg or anti-HCV), (3) excessive alcohol consumers (men > 4 drinks/d or women > 3 drinks/d), (4) pregnant women, (5) participants with missing fatty liver index (FLI) components or fatty acid intake data and (6) participants with missing key covariates. After excluding 57 071 individuals, 13 119 eligible adults remained (online Supplementary Figure S1). Missing data for physical activity, poverty:income ratio (PIR) and hypercholesterolaemia (about 10 % each) were coded as a separate category of those variables.
Definition of metabolic dysfunction-associated steatotic liver disease
The definition of MASLD was based on the United States Fatty Liver Index (US-FLI)(Reference Ruhl and Everhart30), a validated non-invasive surrogate marker widely applied in NHANES-based epidemiological studies, calculated as: US-FLI = (e^y) / (1 + e^y) × 100, where y = 0·8073 × non-Hispanic Black + 0·3458 × Mexican American + 0·0093 × age + 0·6151 × ln GGT + 0·0249 × waist circumference + 1·1792 × ln insulin + 0·8242 × ln glucose − 14·7812. Participants without other causes of liver diseases (positive HBsAg or anti-HCV, excessive alcohol consumption or pregnancy) were classified as having MASLD if US-FLI ≥ 30. The control group comprised participants without MASLD (US-FLI < 30) from the same eligible population.
Cardiometabolic risk factors
Following the 2023 MASLD Delphi consensus criteria(Reference Rinella, Lazarus and Ratziu1), we defined the presence of cardiometabolic risk factors based on five components:
-
(1) Overweight/obesity: BMI ≥ 25 kg/m2
-
(2) Diabetes: Self-reported diagnosis or use of medication
-
(3) Hypertension: Self-reported diagnosis or use of medication
-
(4) Hypertriacylglycerolaemia: Fasting TAG ≥ 150 mg/dl
-
(5) Low HDL-cholesterol: < 40 mg/dl for men and < 50 mg/dl for women
Participants with none of these risk factors were classified as having no cardiometabolic risk factors, while those with at least one were classified as having cardiometabolic risk factors. This binary variable was used for stratified analyses and to assess potential effect modification by metabolic status.
Assessment of dietary SFA
We utilised the average values from two 24-h dietary recall interviews(Reference Wang, Yu and Zhang31). For participants who did not complete the second recall, only the first day’s data were used. Among the included participants, 94·8 % of participants completed the dietary recall for the first day, 84·1 % completed it for the second day and 84·1 % of participants completed both 24-h recalls (online Supplementary Table S14). NHANES collected data on eight SFA, specifically C4:0 (butyric acid), C6:0 (caproic acid), C8:0 (caprylic acid), C10:0 (capric acid), C12:0 (lauric acid), C14:0 (myristic acid), C16:0 (palmitic acid) and C18:0 (stearic acid). Very long-chain SFA (C20:0, C22:0 and C24:0) are not available in the public-use data files and were therefore not examined in this study.
Covariates
Demographic information includes age, sex, marital status, race/ethnicity (non-Hispanic White, non-Hispanic Black, Mexican American, non-Mexican Hispanic and other races), household income and education level (< high school, high school and ≥ college). Household income was categorised based on the PIR into low (PIR ≤ 2·0) and high (PIR > 2·0). Physical activity was defined as engaging in any vigorous-intensity exercise, fitness or recreational activities lasting at least 10 min continuously within a week. BMI was categorised as < 25 kg/m2 (normal/underweight) or ≥ 25 kg/m2 (overweight/obese). Smoking status was determined based on the participant’s response to the question ‘Have you smoked at least 100 cigarettes in your lifetime?’ from the smoking questionnaire. Hypertension, diabetes and high cholesterol were identified based on self-reported diagnoses.
Statistical analysis
Baseline characteristics of MASLD group and control group were compared using parametric (Student’s t test) or non-parametric tests (Mann–Whitney U test and χ 2 test). Fatty acid intakes were adjusted for total energy intake using the residual method(Reference McCullough and Byrd32) and were mean-centred prior to analyses.
We used unadjusted and adjusted multivariable logistic regressions to evaluate associations between individual SFA and MASLD. Restricted cubic spline (RCS) models with three knots were applied to explore the dose–response relations. Subgroup analyses were conducted by sex, age, BMI and presence of cardiometabolic risk factors to explore potential effect modification. For each factor, interaction terms between the SFA and the subgroup indicator were included in the regression models to test whether the associations differed across subgroups.
We applied weighted quantile sum (WQS) and quantile g-computation (QGC) models to assess the joint associations of the SFA mixture. WQS index was constructed based on the quartiles of SFA intake(Reference Carrico, Gennings and Wheeler33). Separate WQS models were fitted for positive/negative directions using a logit link, with 1000 bootstrap iterations conducted in the training (40 %) and validation (60 %) subsets. QGC further estimated the directional associations of individual SFA, in which positive/negative weights sum to 1.
We assessed the mediating roles of IR and serum albumin in the SFA-MASLD association. IR was defined by the HOMA-IR index(Reference Abdesselam, Zidoum and Zadjali34), calculated as fasting insulin (μU/ml) × fasting glucose (mmol/l) ÷ 22·5, with HOMA-IR ≥ 2·0 considered as indicating IR. We used the Stata ‘medeff’ command(Reference Imai, Keele and Tingley35) to estimate the direct effect and indirect effect, with 1000 bootstrapped resamples. Finally, sensitivity analyses were conducted to assess the robustness of the main results, including: (1) applying the NHANES complex sampling design; (2) using an alternative definition of fatty liver – HSI(Reference Lee, Kim and Kim36), calculated as: HSI = 8 × (alanine aminotransferase/aspartate aminotransferase ratio) + BMI (+2 for female; +2 for diabetes), with HSI > 36 indicating MASLD; (3) excluding participants with missing values in physical activity, PIR and high cholesterol; (4) using multiple imputation on missing data on physical activity, PIR and high cholesterol (mi impute chained in Stata); (5) adjusting P-values using the Benjamini–Hochberg false discovery rate; (6) adjusting alcohol consumption, PUFA and MUFA; (7) restricting the analysis to participants who completed both 24-h recalls and (8) using raw SFA values with adjustment for total energy, protein and carbohydrate. The RCS, WQS and QGC models were performed in R (version 4.4.1), while all other analyses were conducted using Stata (version 18.0). A two-sided P-value < 0·05 was considered statistically significant.
Results
Descriptive statistics
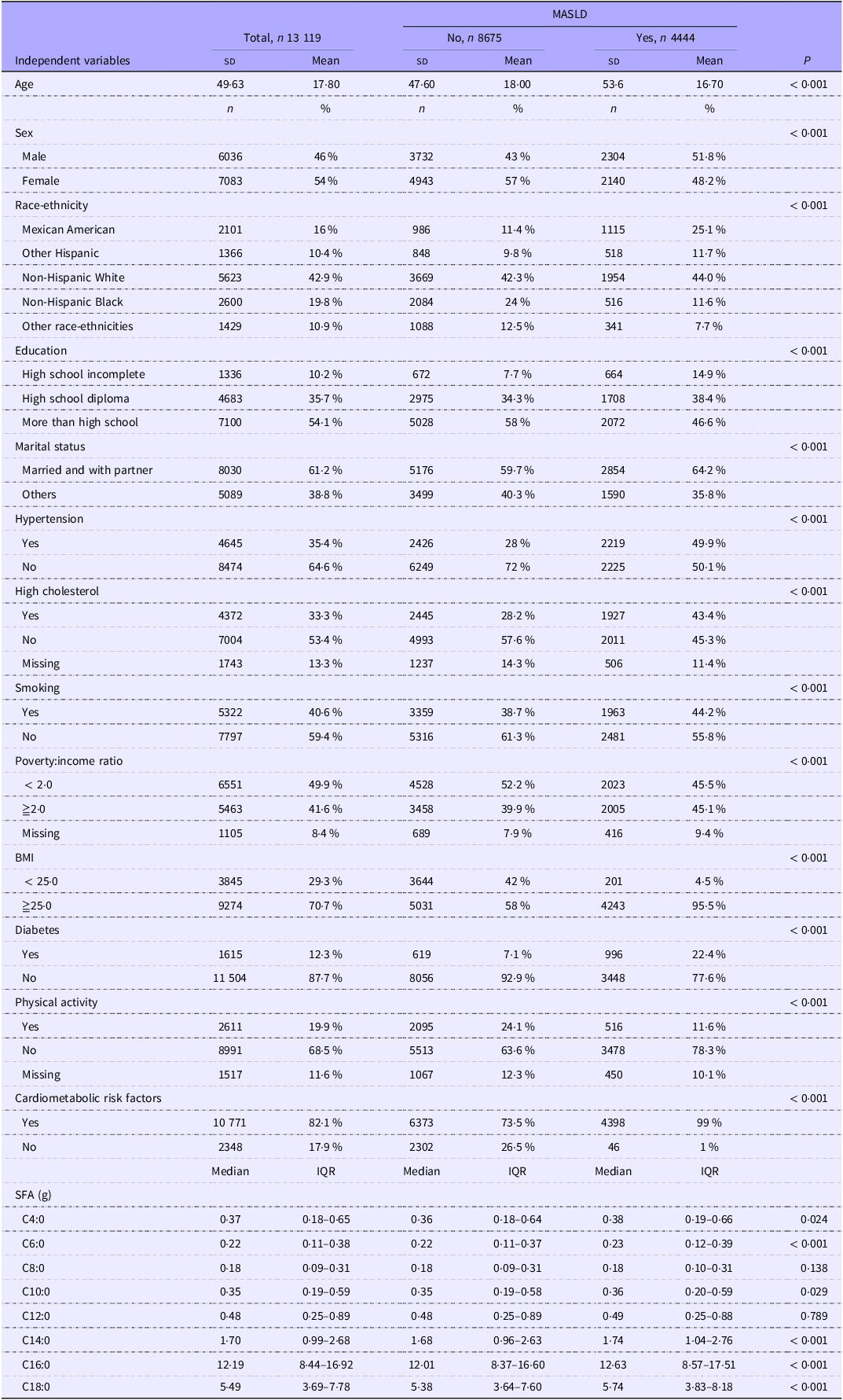
The baseline characteristics of the 13 119 sampled participants are presented in Table 1. Among them, 4444 (33·9 %) had MASLD. Compared with the non-MASLD group, participants in the MASLD group were older, more likely to be male, less likely to receive higher education and showed higher prevalence of hypertension, high cholesterol, smoking, diabetes and obesity. Notably, dietary intake levels of C4:0, C6:0, C10:0, C14:0, C16:0 and C18:0 were significantly higher in the MASLD group v. the control group. Spearman’s rank correlation revealed (online Supplementary Figure S2) that the strongest correlations among the eight SFA were observed between C8:0 and C10:0 and between C16:0 and C18:0 (both r = 0·96).
Baseline characteristics of study participants (≥ 20 years old)

MASLD, metabolic dysfunction-associated steatotic liver disease.
Continuous variables are represented as sd (mean) or median (interquartile range, IQR). The categorical variable is represented as n (%).
C4:0 (butyric acid), C6:0 (caproic acid), C8:0 (caprylic acid), C10:0 (capric acid), C12:0 (lauric acid), C14:0 (myristic acid), C16:0 (palmitic acid) and C18:0 (stearic acid). Cardiometabolic risk factors were defined according to the 2023 MASLD Delphi consensus criteria (presence of at least one of: overweight/obesity (BMI ≥ 25 kg/m2), diabetes, hypertension, hypertriacylglycerolaemia (TAG ≥ 150 mg/dl) or low HDL-cholesterol.
The association between single fatty acids and metabolic dysfunction-associated steatotic liver disease
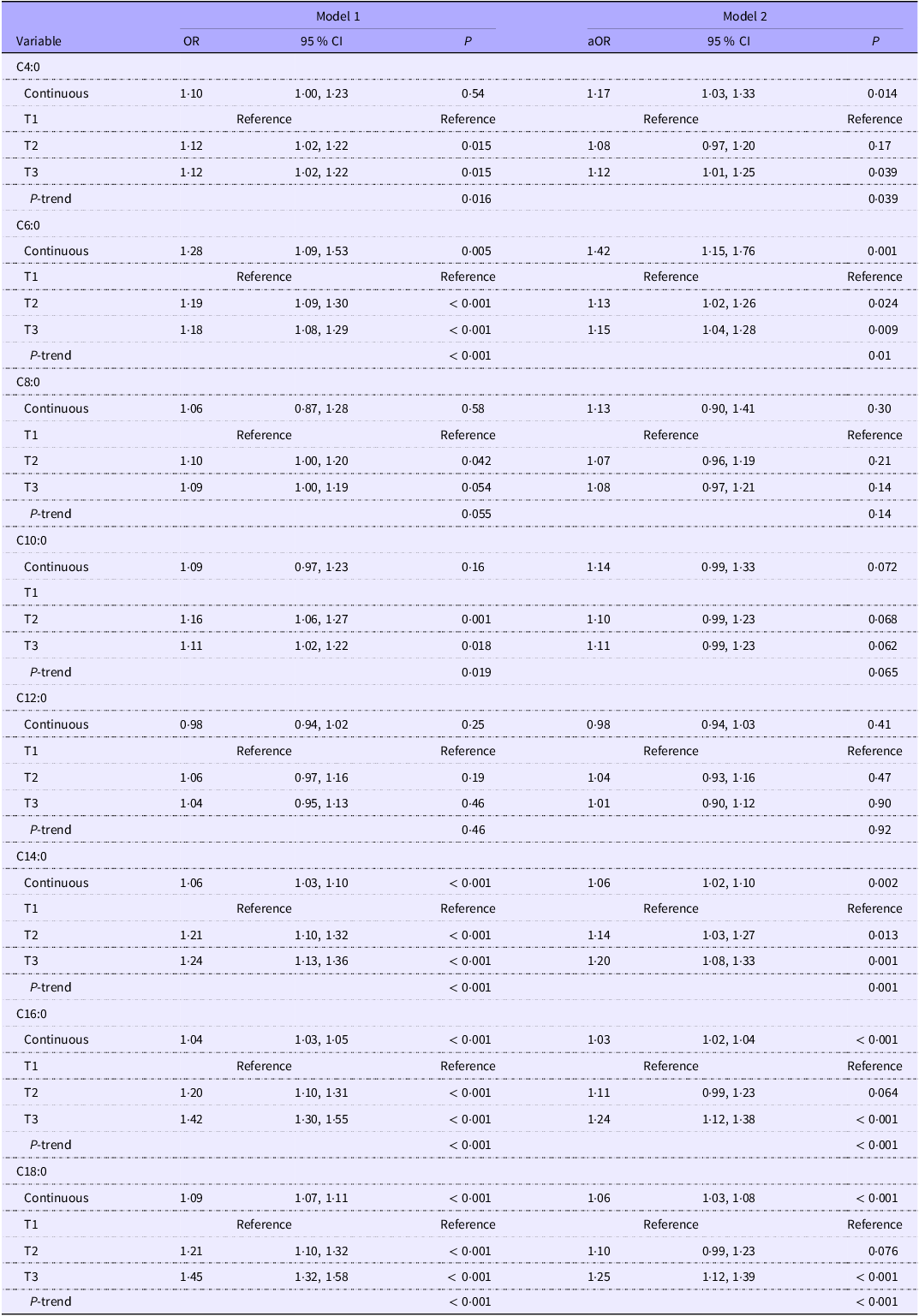
In the unadjusted model, all SFA were positively associated with MASLD except for C8:0, C10:0 and C12:0 (Table 2). After multivariable adjustment, higher intakes of specific SFA were associated with elevated odds of MASLD: C4:0, OR 1·17 (95 % CI 1·03, 1·33); C6:0, OR 1·42 (95 % CI 1·15, 1·76); C14:0, OR 1·06 (95 % CI 1·02, 1·10); C16:0, OR 1·03 (95 % CI 1·02, 1·04); and C18:0, OR 1·06 (95 % CI 1·03, 1·08). These correspond to 17 %, 42 %, 6 %, 3 % and 6 % higher odds of MASLD per 1 g/d increase in C4:0, C6:0, C14:0, C16:0 and C18:0, respectively.
The association between individual fatty acids and MASLD

MASLD, metabolic dysfunction-associated steatotic liver disease; PIR, poverty:income ratio.
C4:0 (butyric acid), C6:0 (caproic acid), C8:0 (caprylic acid), C10:0 (capric acid), C12:0 (lauric acid), C14:0 (myristic acid), C16:0 (palmitic acid) and C18:0 (stearic acid).
Model 1: unadjusted model.
Model 2: based on age, sex, marital status, race, PIR, education, physical activity, BMI, smoking, diabetes, hypertension and high cholesterol.
When SFA levels were categorised into tertiles, MASLD odds in the highest tertile (T3) of C4:0, C6:0, C14:0, C16:0 and C18:0 were 12 % (OR = 1·12, 95 % CI 1·01, 1·25), 15 % (OR = 1·15, 95 % CI 1·04, 1·28), 20 % (OR = 1·20, 95 % CI 1·08, 1·33), 24 % (OR = 1·24, 95 % CI 1·12, 1·38) and 25 % (OR = 1·25, 95 % CI 1·12, 1·39) higher than the reference group (T1) after adjusting for covariates, respectively. Tests for linear trends indicated that, all SFA, except for C8:0, C10:0 and C12:0, were significantly associated with increased odds of MASLD (P for trend < 0·05).
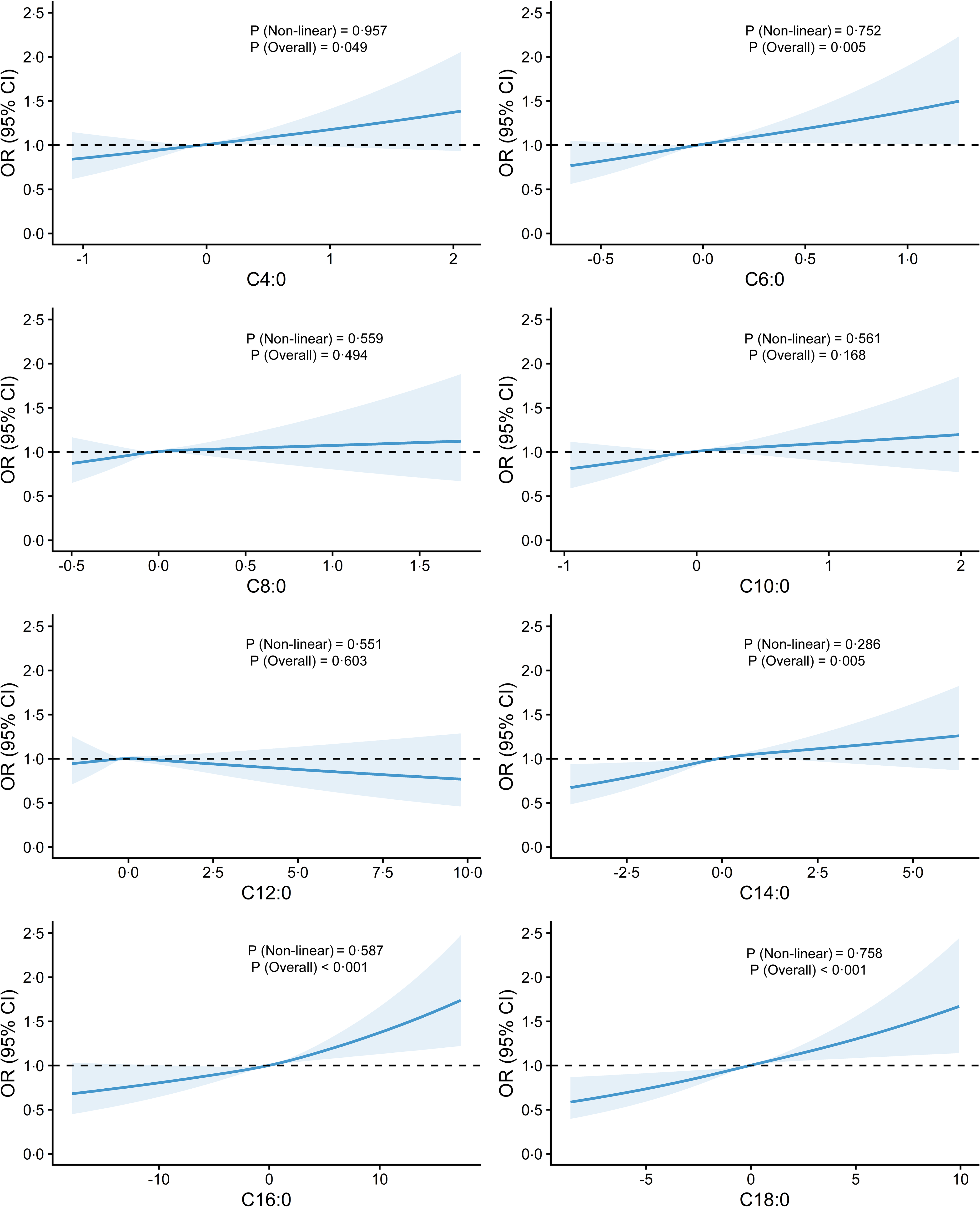
Additionally, RCS models (Figure 1) revealed monotonic, dose–response relationships between specific SFA (C4:0, C6:0, C14:0, C16:0 and C18:0) and MASLD risk (P for overall < 0·05). No evidence of non-linear associations was observed between any SFA and MASLD.
Restricted cubic spline (RCS) curves of dose–response relationships between eight SFA and metabolic dysfunction-associated steatotic liver disease (MASLD). Adjusted for covariates including age, sex, marital status, race, poverty:income ratio (PIR), education, physical activity, BMI, smoking, diabetes, hypertension and high cholesterol.

Subgroup analyses
Among participants aged 60 years and older, the highest tertile (T3) of C6:0, C8:0, C10:0, C12:0 and C14:0 was associated with higher odds of MASLD compared with T1 (online Supplementary Table S1). Significant interactions were observed between age and both C8:0 and C12:0 (P for interaction < 0·05). C16:0 and C18:0 showed positive associations with MASLD across age groups.
When stratifying the sample by sex, T3 levels of C4:0, C6:0 and C14:0 were associated with higher odds of MASLD in males (v. T1), but no significant associations were observed in females (online Supplementary Table S2). C16:0 and C18:0 were positively associated with MASLD in both sexes. However, no significant interactions were found between sex and individual SFA.
Concerning BMI (online Supplementary Table S3), higher levels (T3) of C6:0, C14:0, C16:0 and C18:0 were associated with higher odds of MASLD among participants with higher BMI (≥25 kg/m2), whereas no significant associations were observed in those with BMI < 25 kg/m2. The BMI–SFA interactions were not significant.
In the subgroup with at least one cardiometabolic risk factor (online Supplementary Table S4), higher intakes of C4:0, C6:0, C14:0, C16:0 and C18:0 were significantly associated with MASLD, consistent with the main analysis. In the subgroup without any cardiometabolic risk factor, the continuous OR for SFA ranged from 0·99 to 2·45, with all 95 % CI including 1·0 (online Supplementary Table S4). In tertile analyses, compared with the lowest tertile (T1), the highest tertile (T3) of C8:0, C10:0, C12:0 and C14:0 was positively associated with MASLD. No other SFA showed statistically significant associations in this subgroup.
Joint effects of mixed SFA on metabolic dysfunction-associated steatotic liver disease
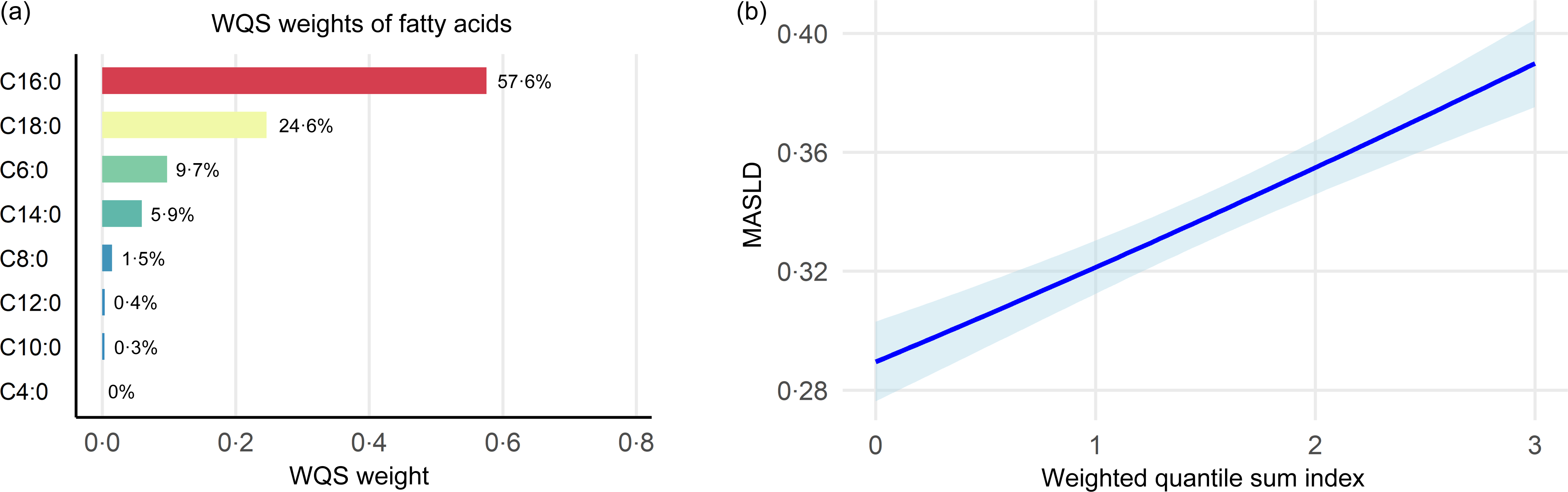
The WQS model was used to evaluate the association of SFA mixtures on MASLD (Figure 2). After covariates adjustment, the WQS model demonstrated an overall positive association between SFA mixtures and MASLD (online Supplementary Table S4), in which C16:0 carried the largest positive weight (58 %), followed by C18:0 (25 %) (Figure 2(a)). Each quartile increase in the WQS index (Figure 2(b)) was associated with 10 % higher odds of MASLD (OR = 1·10, 95 % CI 1·04, 1·17).The negative-direction WQS regression yielded no association between SFA mixtures and MASLD (OR = 1·02, 95 % CI 0·95, 1·06).
Association between SFA mixtures and metabolic dysfunction-associated steatotic liver disease (MASLD) based on the weighted quantile sum (WQS) model. (a) The weights of eight SFA in the positive direction. (b) The association between SFA mixtures and MASLD.

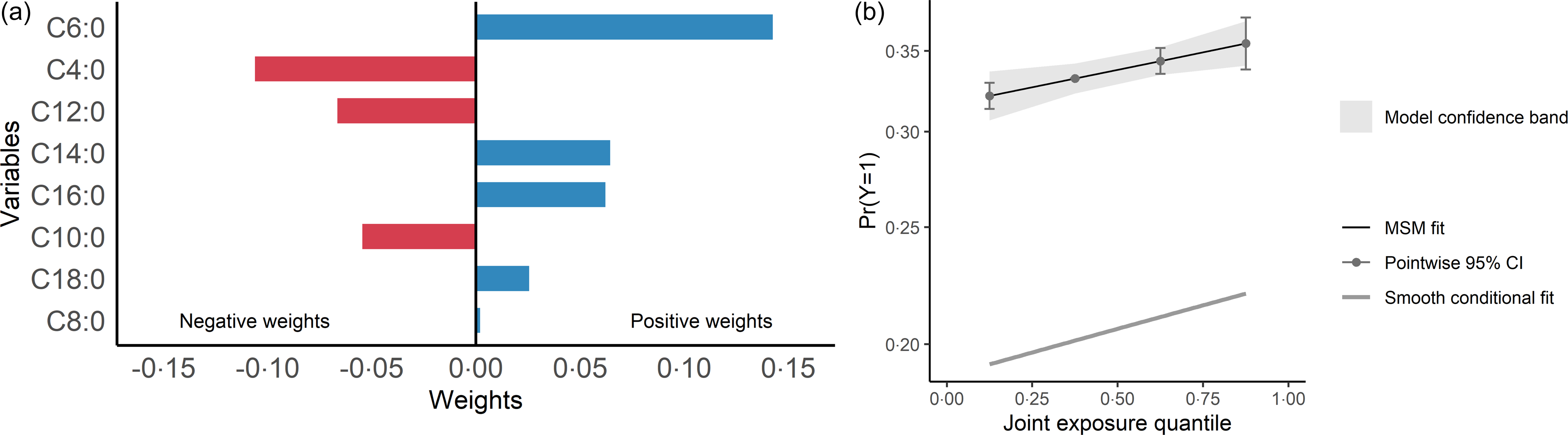
The QGC model corroborated findings of the WQS analysis (online Supplementary Table S4), indicating 3 % higher odds of MASLD with a one-quartile increase in the joint SFA mixture (OR = 1·03, 95 % CI 1·01, 1·06). C6:0, C16:0, C14:0, C18:0 and C8:0 exhibited positive weights, while C4:0, C12:0 and C10:0 showed negative weights (Figure 3).
Association between the SFA mixture and metabolic dysfunction-associated steatotic liver disease (MASLD) based on the quantile g-computation (QGC) model. (a) Estimated weights of individual SFA contributing to the overall association. (b) Combined association of the SFA mixture with MASLD.

Mediation analysis
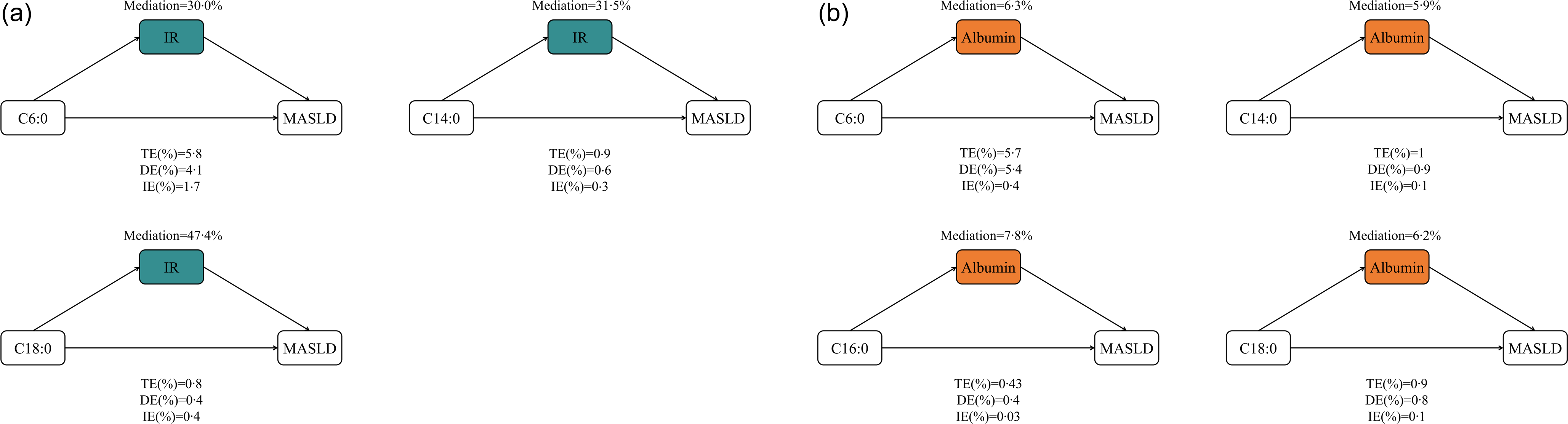
Mediation analysis was restricted to SFA with significant associations with MASLD (online Supplementary Table S5), incorporating IR (binary) and serum albumin (continuous) as potential mediators (Figure 4). IR accounted for 30·0 % (C6:0), 31·5 % (C14:0) and 47·4 % (C18:0) of the total association (Figure 4(a)). No significant indirect associations were observed for other SFA. Serum albumin also played a notable mediating proportions (Figure 4(b)), accounting for 6·3 %, 5·9 %, 7·8 % and 6·2 % of the total effects of C6:0, C14:0, C16:0 and C18:0, respectively.
Mediating role and proportion of insulin resistance (IR, panel (a)) and serum albumin (b) in the association between SFA and metabolic dysfunction-associated steatotic liver disease (MASLD). This model has been adjusted for age, sex, marital status, race, poverty:income ratio (PIR), education, physical activity, BMI, smoking, diabetes, hypertension and high cholesterol. TE, total effect; DE, direct effect; IE, indirect effect. The proportion mediated was calculated as (IE/TE) × 100 %.

Sensitivity analyses
All sensitivity analyses – including survey-weighted models, HSI-defined MASLD, complete-case analysis, multiple imputation, false discovery rate adjustment, adjustment for alcohol, PUFA and MUFA, restriction to participants who completed both 24-h recalls and use of raw SFA values with adjustment for total energy, protein and carbohydrate – yielded results similar to our main analyses (online Supplementary Tables S6–16), thus corroborating our findings.
Discussion
This study is the first large-scale investigation to systematically evaluate individual and combined associations of specific SFA on MASLD. Higher intakes of most SFA were independently associated with increased odds of MASLD. RCS models demonstrated significant linear dose–response relationships between most SFA and MASLD. Significant age–SFA interactions were observed for C8:0 and C12:0. Furthermore, mixed exposure models confirmed a positive association between SFA mixtures and MASLD, with C16:0 contributing most prominently, while mediation analyses indicated that IR and serum albumin may act as partial mediators in these associations, possibly providing novel and potential pathways for complicated relationships.
Among fatty acids, abnormal SFA accumulation is a key dietary driver of MASLD development and progression(Reference Chen, Pang and Huang37). For instance, C16:0-rich diets exacerbate liver injury and metabolic dysfunction, critically driving MASLD progression(Reference Ceja-Galicia, Cespedes-Acuña and El-Hafidi16,Reference Scavo, Negro and Arrè38) . Among other LCFA, elevated levels of C18:0 and C14:0 have also been positively associated with the severity of MASLD(Reference López-Bautista, Barbero-Becerra and Ríos39,Reference Jiang and Sun40) , which is consistent with our findings. As for SCFA and MCFA, some studies suggest that they have lower lipotoxicity and may even exert anti-inflammatory effects(Reference Gao, Yao and Meng18,Reference Huang, Gao and Chen19) , but real-world dietary patterns involve complex mixtures, potentially modulating the net effect of individual fatty acids. The results of the WQS and QGC models further support the association between SFA mixture exposure and MASLD, which is consistent with previous findings(Reference Zhuang, Ao and Liu41).
While some studies suggested lower lipotoxicity of SCFA, our findings showed that C4:0 and C6:0 were positively associated with MASLD. This inconsistency may stem from SCFA inducing inflammation by promoting pro-inflammatory cytokines and immune cell migration(Reference Du, He and An42,Reference Cueno, Kamio and Seki43) . Notably, in the QGC mixture model, C4:0, C10:0 and C12:0 exhibited negative weights, which contrasted with their positive single-exposure associations observed in univariate analyses. This apparent discrepancy is likely attributable to strong multicollinearity among fatty acids in the mixture, rather than a genuine protective effect of these fatty acids. Specifically, Spearman’s correlations between C4:0 and other fatty acids all exceeded 0·6, and those for C10:0 and C12:0 with other fatty acids were all above 0·58 (online Supplementary Figure S2), indicating substantial intercorrelations among these lipids. Moreover, in real-world dietary patterns, various fatty acids often interact and potentially influence one another, which may further contribute to the observed differences between mixture and single-exposure models(Reference Gehrmann, Würdemann and Plötz44,Reference Horrobin, Jenkins and Bennett45) . Therefore, the divergent results between single-exposure and mixture models may reflect statistical redistribution of overall risk contributions when accounting for correlated exposures, rather than opposing biological effects.
Furthermore, we observed a U-shaped pattern in the association between SFA’s chain length and MASLD. LCFA (C14:0, C16:0 and C18:0) and SCFA (C4:0 and C6:0) were positively correlated with MASLD, while MCFA (C8:0, C10:0) showed no significant association with the same. This result may be explained by the fact that LCFA(Reference Senanayake, Hapugaswatta and Samarawickrama14) and SCFA(Reference Du, He and An42) are more likely to accumulate in hepatocytes and induce inflammatory responses and oxidative stress at high exposure levels. In contrast, MCFA may exert relatively weak effects due to their rapid metabolism and lower hepatic accumulation(Reference Pereyra, McLaughlin and Buddo46). Chain length structure of fatty acids may play a critical role in modulating SFA’s effects on MASLD, warranting further investigation.
C16:0 emerged as the dominant contributor in both WQS and QGC models, supporting its important role in the SFA–MASLD association. The differential weighting between the mixture models reflects their methodological distinctions: WQS captures unidirectional linear effects(Reference Carrico, Gennings and Wheeler33), whereas QGC detects non-linear interactions(Reference Keil, Buckley and O’Brien47).
Mediation analysis revealed significant indirect pathways through IR in the associations of C6:0, C14:0 and C18:0 with MASLD. Notably, IR explained over 30 % of the total effect, highlighting its role as a key mediator in the SFA-MASLD associations. Serum albumin explained an additional 6–8 % of the total effects, partially offsetting the harmful associations of SFA on MASLD, suggesting a potential inverse association. This inverse association may be weakened if high SFA intake is associated with lower albumin levels(Reference Linciano, Moro and Zorzi48), impairing its anti-inflammatory and antioxidant functions, which could contribute to liver injury and higher odds of MASLD.
Among participants aged 60 years and older, C8:0 and C12:0 intakes were associated with higher odds of MASLD, which may be related to prolonged exposure or age-related declines in mitochondrial function or fatty acid oxidation(Reference Lesnefsky, Chen and Hoppel49). C4:0, C6:0 and C14:0 were associated with higher odds of MASLD among males but not among females. This sex difference may be explained by oestrogen-mediated enhancement of fatty acid oxidation and inhibition hepatic lipid accumulation(Reference Fabre, Tramunt and Montagner50), though no significant interactions were found between sex and individual SFA. Among individuals with BMl ≥ 25 kg/m2, although no significant interaction was observed, C6:0, C14:0, C16:0 and C18:0 were significantly associated with MASLD. Elevated BMI is often accompanied by visceral fat accumulation that may be associated with greater sensitivity to fatty acid exposure(Reference Garg, Kushwaha and Dubey51), which could contribute to MASLD progression. We further explored whether the associations between SFA and MASLD differed according to the presence of cardiometabolic risk factors. In participants with at least one cardiometabolic risk factor, the associations were robust and largely consistent with the main analysis. This observation is in line with the updated definition of MASLD, which is inherently characterised by hepatic steatosis in the presence of underlying metabolic dysfunction(52). In participants without any cardiometabolic risk factors, the number of MASLD cases was very limited, resulting in wide CI. Although a few tertiles of C8:0, C10:0, C12:0 and C14:0 showed positive associations, these findings should be interpreted cautiously given the small number of events; overall, the direction of associations was generally similar to the main analysis. Interaction tests between each SFA and cardiometabolic risk factor status were not statistically significant, indicating no strong evidence of effect modification. Taken together, these findings suggest that the observed associations between SFA and MASLD are largely independent of cardiometabolic risk burden, although the limited number of MASLD cases in the low-risk group reduces the precision of effect estimates, and future studies with larger samples of metabolically healthy individuals with MASLD are warranted to confirm these observations.
This study has several strengths: a large, nationally representative sample ensuring data quality and population representativeness; the combined use of traditional logistic regression and mixture models to ensure robust results; and preliminary mechanistic exploration via mediation analysis to inform future research.
However, several limitations should be noted. (1) Due to the cross-sectional nature of this study, causal relationships cannot be established, and the temporal sequence between SFA intake and MASLD onset remains unclear. Although we observed that HOMA-IR and serum albumin partially mediated the associations between certain SFA and MASLD, these findings do not imply causality. Reverse causality and unmeasured confounding cannot be ruled out, and longitudinal studies are needed to establish temporal sequences. (2) A further limitation is the conceptual overlap between the mediator (HOMA-IR) and the outcome definition (US-FLI), as both formulas incorporate fasting glucose and insulin. This structural overlap may inflate the mediation estimates and should be considered when interpreting the results. Consequently, our mediation findings must be interpreted with extreme caution as exploratory observations rather than definitive mechanistic pathways. Future studies using imaging-based MASLD definitions independent of metabolic parameters are warranted to validate these findings. (3) Dietary intake was assessed using 24-h recalls, which are subject to recall bias and may not capture long-term habitual intake. Such non-differential misclassification would likely bias associations towards the null, suggesting that the observed associations may be conservative estimates. However, the high proportion of participants completing two recalls (84·1 %) and the consistent results in sensitivity analyses restricted to those with two recalls provide reassurance regarding the reliability of the dietary data. (4) MASLD was defined using the US Fatty Liver Index (US-FLI), rather than imaging- or biopsy-based diagnosis. US-FLI is a validated non-invasive surrogate marker that has been widely used in NHANES-based epidemiological studies to identify hepatic steatosis at the population level. Nevertheless, US-FLI may be subject to misclassification, as it cannot directly measure hepatic fat content. Such non-differential misclassification would generally bias associations towards the null, suggesting that the observed associations may be conservative. In addition, because US-FLI is a proxy measure, mechanistic interpretations and mediation findings should be interpreted with caution. Future studies using imaging-based MASLD definitions are warranted to confirm these findings. (5) Very long-chain SFA such as C20:0, C22:0 and C24:0 were not available in the NHANES dietary database; thus, their associations with MASLD could not be evaluated in this study despite their potentially protective metabolic properties. Future studies with access to comprehensive dietary databases or biospecimen-based fatty acid profiling are warranted to evaluate the potential roles of these very long-chain SFA in MASLD. (6) Unmeasured confounding may still exist, despite mixture models accounting for the joint effects of fatty acids. Future studies should validate causal relationships using longitudinal data and explore mechanistic pathways using biospecimens and experimental research to support nutritional interventions and individualised MASLD prevention.
Conclusion
Our study provides evidence that the majority of individual and mixture exposures to SFA are positively associated with MASLD in adults, especially in older adults. Significant linear dose–response relationships were observed for most SFA via RCS analysis. IR and serum albumin may serve as important mediators in the associations between certain SFA and MASLD, indicating that these pathways represent potential targets.
Our findings have important implications for public health practice and nutritional strategies targeting MASLD, suggesting that intakes of long-chain and short-chain SFA should be appropriately limited, and that MCFA intake may require moderation in older adults given their unique metabolic vulnerability. Rather than focusing solely on total fat intake, more attention should be given to the structural characteristics of fatty acids to enable more precise dietary interventions for MASLD prevention. Future well-designed studies are warranted to further elucidate the associations and potential mechanisms linking SFA to MASLD.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526106990
Acknowledgements
The authors thank the reviewers for their insightful comments and suggestions that greatly improved this manuscript.
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
X. L.: Conceptualisation, Data curation, Formal analysis, Methodology, Visualisation, Writing – original draft and Writing – review and editing. F. M.: Supervision and Writing – review and editing. Both authors read and approved the final manuscript.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Not applicable. This study uses only secondary data analyses without any personal information identified using statistical data from the NHANES website. The programme was approved by the National Centre for Health Statistics (NCHS) Research Ethics Review Committee, and informed consent was obtained from the participants.



 Open access
Open access