


Forensic mental healthcare in Australia is provided in secure hospitals that have higher levels of physical, relational and procedural security than general mental health hospitals. The patient cohort includes three groups: those on a court-based order who have been found, because of their mental illness, to be either not criminally responsible of an offence or unfit for trial; those who have been transferred for in-patient mental healthcare from the criminal justice system; and those who have problematic behaviours that cannot be effectively managed in general mental health wards. Forensic patients are generally diagnosed with chronic psychotic illnesses such as schizophrenia, and are treated with medications that have a range of side-effects including weight gain. Across Australia there are seven forensic hospitals with varying levels of security (low, medium and high). These forensic hospitals play a critical role within the broader mental health system by providing secure and specialised care for these individuals that pose risks to the community, thereby protecting community safety while supporting rehabilitation and recovery. Although these hospitals provide important interventions for patients, they have been criticised for lacking consistent standards of care, neglecting human rights and relying on insufficient quality evidence for interventions. Reference Tully, Hafferty, Whiting, Dean and Fazel1
Australia’s National Mental Health Commission has highlighted that equity in health is a fundamental human right. 2 Although there is no national Human Rights Act, the Australian Capital Territory, Victoria and Queensland have all passed their own state and territory legislation. 3 In light of human rights principles, it is important to highlight that forensic patients are entitled to equivalency of care, that is, healthcare of the same standard and quality as that available to individuals in the broader community. The challenge is that forensic hospitals are highly structured environments. Strict security protocols govern access into the hospital environment. Access to hospital wards is also tightly controlled.
There is already a significant life expectancy gap of at least 11 years for those who access mental health-related treatments compared with the rest of the population. Reference Roberts, Wong, Lawn, Lawrence and Johnson4 Older estimates have reported a gap of up to 20 years for those with severe mental illness. Reference Lawrence, Hancock and Kisely5 Cardiovascular disease and poor physical health are contributing factors. Research considering forensic in-patient populations, frequently subject to long in-patient stays, has highlighted the risks of being overweight/obese, gaining weight during admissions and developing metabolic syndrome and associated medical illnesses. Reference Andersson, von Schreeb, Johansson, Sturidsson, Wetterborg and Sorjonen6,Reference Jeandarme, Goktas, Claessens, Michem, Van Poucke and Verbeke7 Further, forensic in-patients have reported low levels of physical activity, Reference Moss, Meurk, Steele and Heffernan8 putting them at increased risk of a range of conditions, including cardiometabolic disorder, which increases the risk of premature death. Reference Druss, Zhao, Von Esenwein, Morrato and Marcus9 In a Queensland cohort, patients’ length of stay ranged from 55 to 6852 days (median 741 days, interquartile range 1322.5), with some patients staying up to 18.8 years, illustrating the prolonged duration of forensic in-patient care. Reference Moss, Meurk, Steele and Heffernan8
Evidence from forensic populations highlights the severity of these risks. Rees and Thomson Reference Rees and Thomson10 followed a Scottish forensic cohort for a mean of 21.1 years and found that 36.9% of patients died at an average age of 55.6 years, with 70.8% of deaths occurring prematurely. Men lost on average 14.9 years and women 24.1 years of potential life. These findings underscore the critical need for forensic hospitals to have a structured and comprehensive approach to physical health management, with strategies in place for screening and monitoring physical health.
There is widespread recognition of the need for effective intervention strategies to address health screening findings. 11,Reference Perry, Holt, Chew-Graham, Tiffin, French and Pratt12 Lifestyle interventions targeting diet, physical activity and behaviour modification have been shown to improve body weight, fitness, psychiatric symptoms and physical activity levels. Reference Martland, Teasdale, Murray, Gardner-Sood, Smith and Ismail13,Reference Deenik, Tenback, Tak, Rutters, Hendriksen and van Harten14 However, research on the effectiveness of these interventions in forensic populations remains limited. Reference Moss, Meurk, Steele and Heffernan15,Reference Rogers, Kinnafick and Papathomas16 Although some studies in forensic settings have explored approaches including technology, education and exercise, they lack randomised control groups and do not consistently report on physical health outcomes, leaving a significant gap in the literature.
Emerging literature highlights the perspectives of both patients and staff on physical health and activity in forensic hospitals. Studies have explored how adolescent and adult in-patients perceive the role and significance of physical activity, as well as their experiences and preferences. Anthony and colleagues found widespread agreement among patients and staff that physical activity offers multiple benefits, including improved mood, increased engagement and enhanced pro-social behaviours. Reference Anthony, Papathomas, Annandale, Breen and Kinnafick17 They concluded that health promotion and physical health support should be integrated into service provision, with staff collaboration being essential. Similarly, the authors of this current study recently emphasised the importance of social and environmental factors in encouraging physical activity and further supported its inclusion within a comprehensive treatment framework. Reference Moss, Meurk, Steele and Heffernan18
Given gaps in physical healthcare for forensic in-patients, and government undertakings at both state and federal levels to better support the physical health needs of mental health consumers, a national examination is timely. 19,20 Currently, there is no national approach to assessing and monitoring physical health or providing physical activity opportunities for forensic in-patients. This study had three aims:
-
(a) to examine the physical health and activity data collected by staff at forensic hospitals;
-
(b) to evaluate how physical health issues are managed, the available physical activity opportunities, and who supervises, prescribes and monitors these activities;
-
(c) to assess staff perspectives on facilitators and challenges of addressing the physical health and activity needs of forensic in-patients.
Method
Context
The setting for this national study included the forensic hospitals across Australia, comprising the High Secure Inpatient Service in Queensland, Forensic Hospital in New South Wales, Thomas Embling Hospital in Victoria, James Nash House in South Australia, Frankland Centre in Western Australia, Dhulwa Secure Mental Health Unit in the Australian Capital Territory and Wilfred Lopes Centre in Tasmania.
Study design
A mixed-methods study was undertaken, including an online survey and focus groups. The conduct and reporting of the qualitative elements of the study adhere to the Standards for Reporting Qualitative Research. Reference O’Brien, Harris, Beckman, Reed and Cook21
Ethics
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human patients were approved by the Royal Brisbane and Women’s Hospital Research Ethics Committee (HREC/2021/QRBW/78458) and ratified by the University of Queensland. It was applied for under the multi-site National Mutual Acceptance scheme. Seven sites were included in the application including the High Secure Inpatient Service in Queensland, Forensic Hospital in New South Wales, Thomas Embling Hospital in Victoria, James Nash House in South Australia, Frankland Centre in Western Australia, Dhulwa Secure Mental Health Unit in the Australian Capital Territory and Wilfred Lopes Centre in Tasmania.
Informed consent (either written or verbal) was obtained for all participants. Verbal consent was witnessed and formally recorded.
Sample and data collection
The clinical directors of each forensic hospital were contacted by the investigators and informed of the study. The clinical directors then nominated key stakeholders (senior staff members including psychiatrists, nurse unit managers and allied health team leaders) to assist in the identification of participants. Participants were eligible if they had expertise in the prescription, supervision and/or management of physical health and activity of forensic in-patients and had worked within a forensic hospital for more than 6 months. The investigators were then provided with the email addresses of potential participants who were emailed and invited to take part in the study.
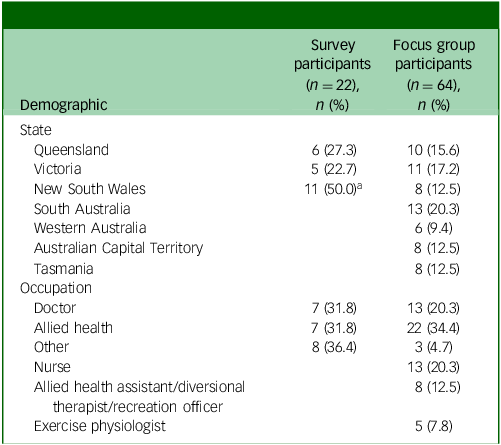
The online survey was completed by participants who consented to the study, via a link that was sent by email to participants. Focus groups were organised by the principal investigator (K.M.) and the site coordinators at each of the forensic hospitals. Participation in the survey and focus groups was independent, as the survey was anonymous apart from state/territory and occupation. Therefore, overlap between survey and focus group participants cannot be determined, although some participants may have contributed to both. The number of participants per hospital in each data source was as follows: survey participants (Queensland: 6, New South Wales: 3, Victoria: 5, South Australia: 2, Western Australia: 2, Australian Capital Territory: 3, Tasmania: 1; n = 22 total); and focus group participants (Queensland: 10, New South Wales: 8, Victoria: 11, South Australia: 13, Western Australia: 6, Australian Capital Territory: 8, Tasmania: 8; n = 64 total).
Of the 17 focus groups conducted, 16 were held via Microsoft Teams and recorded and transcribed using the platform, whereas one was conducted face-to-face. Group size varied because of participant availability, but data were analysed at the state/territory level, supporting thematic saturation within and across jurisdictions. Data collection occurred between September 2023 and January 2025.
Both the survey and focus group schedule were developed by K.M., C.M. and M.L.S., based on the Royal Australian and New Zealand College of Psychiatry’s clinical practice guidelines for schizophrenia and related disorders and the expert consensus statement for the treatment, management and monitoring of the physical health of people with an enduring psychotic illness. Reference Galletly, Castle, Dark, Humberston, Jablensky and Killackey22,Reference Lambert, Reavley, Jorm and Oakley Browne23 Both the online survey and interview script are available in the Supplementary Material available at https://doi.org/10.1192/bjo.2026.12013.
Survey
The survey was created in Checkbox (2023 release, web-based platform, Checkbox Technology Inc., San Francisco, California, USA; https://www.checkbox.com), an online survey platform, and comprised questions regarding the following:
-
(a) health measures on initial assessment and monitoring, and documentation;
-
(b) physical activity measures, opportunities and data tracking;
-
(c) staffing and support available;
-
(d) facilities and equipment available;
-
(e) patient and carer education and involvement.
Focus group
The focus group included questions posed in the online survey and covered the following topics:
-
(a) physical health assessment and monitoring;
-
(b) patient and carer engagement;
-
(c) data collected regarding physical health and/or activity measures and lifestyle interventions;
-
(d) physical activity and obesity management;
-
(e) adherence to guidelines and best practice;
-
(f) facilitators and barriers.
Data analysis
The study utilised a fully mixed concurrent equal status design, integrating qualitative and quantitative data collected simultaneously through an online survey and focus groups. Reference Leech and Onwuegbuzie24 Both types of data were analysed independently before being integrated for comprehensive interpretation.
Responses to the survey were automatically recorded in Checkbox. The responses were also exported to Microsoft Excel and manually reviewed. Of the 32 survey questions completed by 22 participants, 63 responses were missing across 25 questions. Missing data were handled on a per-question basis: for descriptive analyses, available responses were used to calculate totals and percentages, without imputing missing values. Given that multiple respondents contributed information from each hospital, missing responses were assumed to reflect gaps in individual knowledge rather than systematic non-response bias. This approach allowed hospital-level patterns to be reliably assessed despite occasional missing data.
Challenges arose for consistent data representation when staff working within the same facility provided varied responses to survey questions. To address this, it was decided that the presence of a particular practice or resource would be accepted if at least one staff member endorsed it. This approach was based on the understanding that not all staff would be equally informed about all aspects of service provision, and that endorsement by a single respondent was more likely to reflect accurate knowledge based on their specific expertise or role.
The responses from the online survey and focus groups were analysed using an established thematic framework method. Reference Gale, Heath, Cameron, Rashid and Redwood25 One researcher (K.M.) performed the coding and analysis, following the five stages of the method. The first stage involved becoming familiar with the data by reading and rereading it, noting down initial observations. In the second stage, data were coded using both inductive and deductive approaches. The initial coding was conducted in Microsoft Excel. The subsequent stages focused on grouping the codes into potential themes, which were visually represented on a thematic map to aid in the process. This helped to identify broad initial themes and their related subthemes. A final review of the themes ensured clarity and distinctiveness between them. The finalised themes and sub-themes were discussed and agreed upon by all study authors, and representative excerpts were selected for inclusion.
The identified themes will structure the presentation of findings from the study.
Results
A total of 22 surveys were completed between March 2023 and January 2025. There was a range of experience for survey participants working in a forensic hospital environment, from 0.5 to 15 years, with a mean of 5.0 years (s.d. 3.5). Sixty-four individuals participated in 17 focus groups between September 2023 and November 2024. Participant demographic data are shown in Table 1. Survey and focus group participants were broadly similar, and comprised senior clinical staff such as psychiatrists, nurses, occupational therapists, allied health practitioners, and other professionals involved in physical health and activity management (Table 1). Focus groups explored the same thematic areas as the survey, but in a qualitative, discussion-based format. Data from surveys and focus groups were combined at the state/territory level in Tables 3 to 5 to provide a more complete view of staff perspectives while maintaining confidentiality for sites with very small survey numbers.
Demographics of participants

a. Combined across New South Wales, South Australia, Western Australia, Australian Capital Territory and Tasmania.
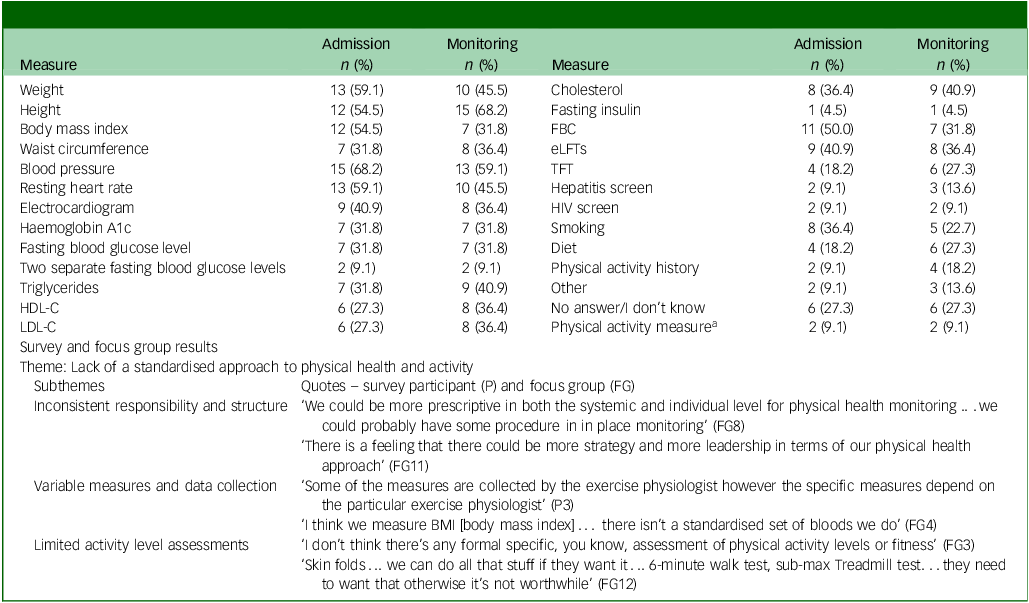
Physical health and activity measures on admission and monitoring in forensic hospitals

FBC, full blood count; eLFTs, electrolytes and liver function tests; TFT, thyroid function tests; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
a. Six-minute walk test, the International Physical Activity Questionnaire and/or Simple Physical Activity Questionnaire.
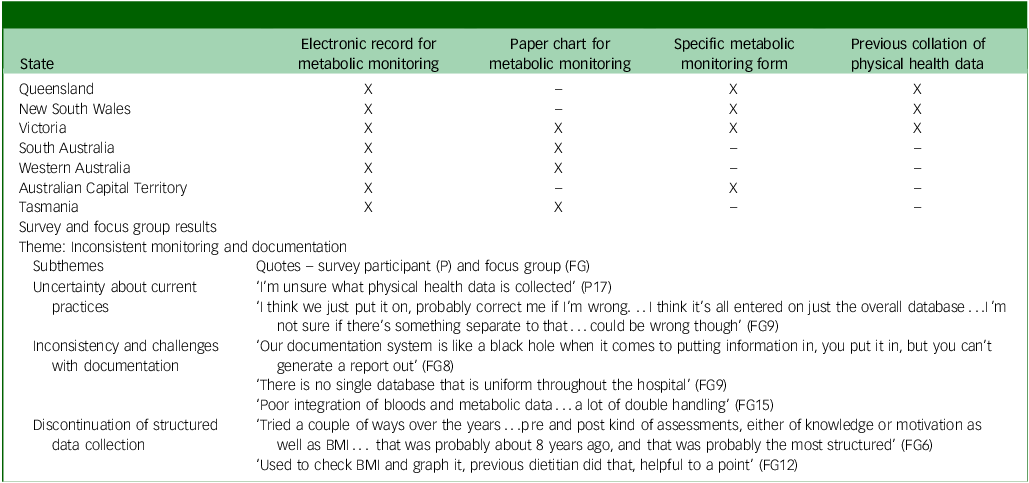
Metabolic monitoring, documentation and data collation practices in forensic hospitals

X, endorsed by at least one participant from forensic hospital in state/territory; –, no survey participants from the site endorsed this response; BMI, body mass index.
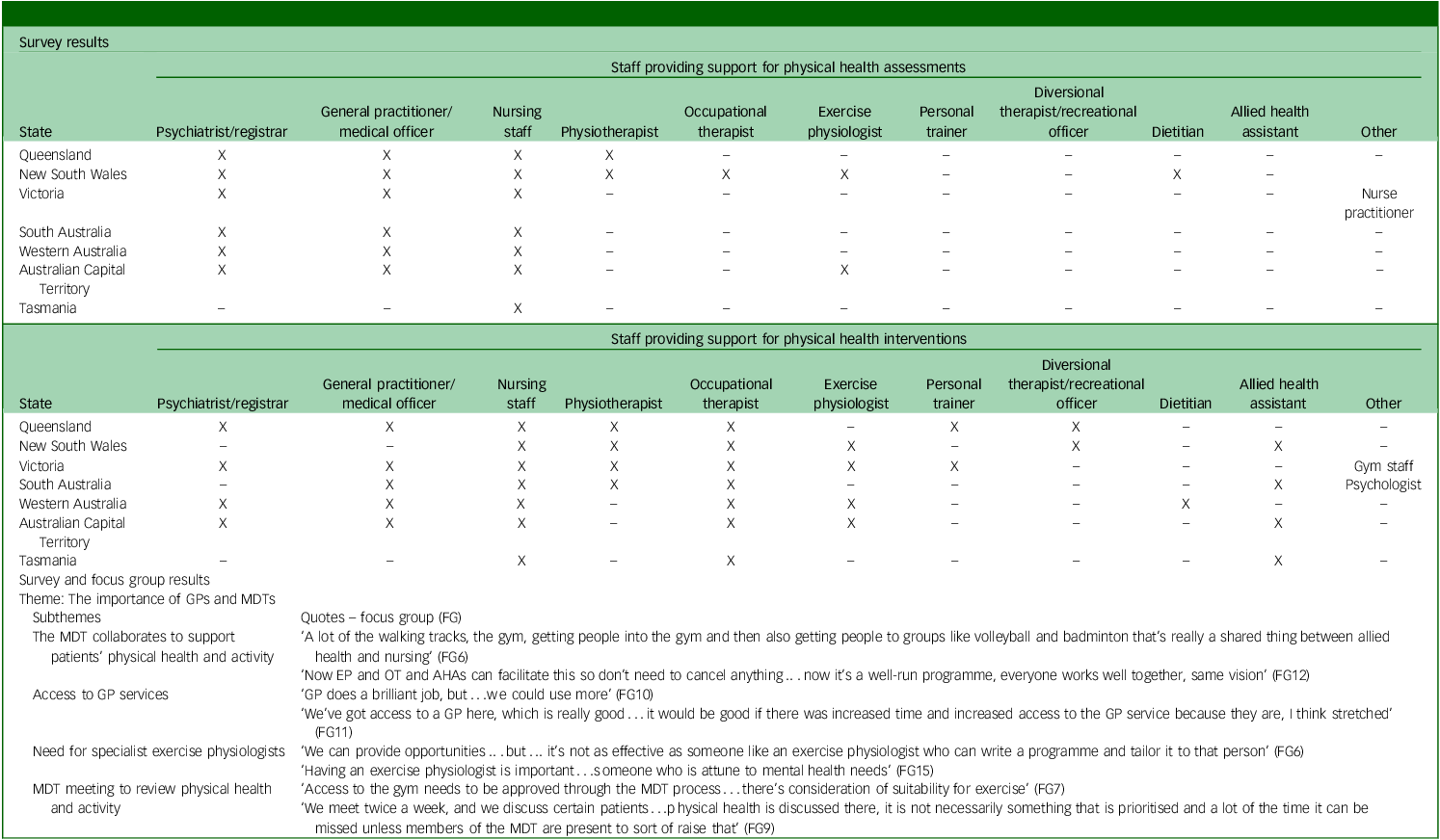
Staff providing support for physical health assessments and physical health interventions

X, endorsed by at least one participant from forensic hospital in state/territory; –, no survey participants from the site endorsed this response. GP, general practitioner; MDT, multidisciplinary team; EP, exercist physiologist; OT, occupational therapist; AHA, allied health assistant.
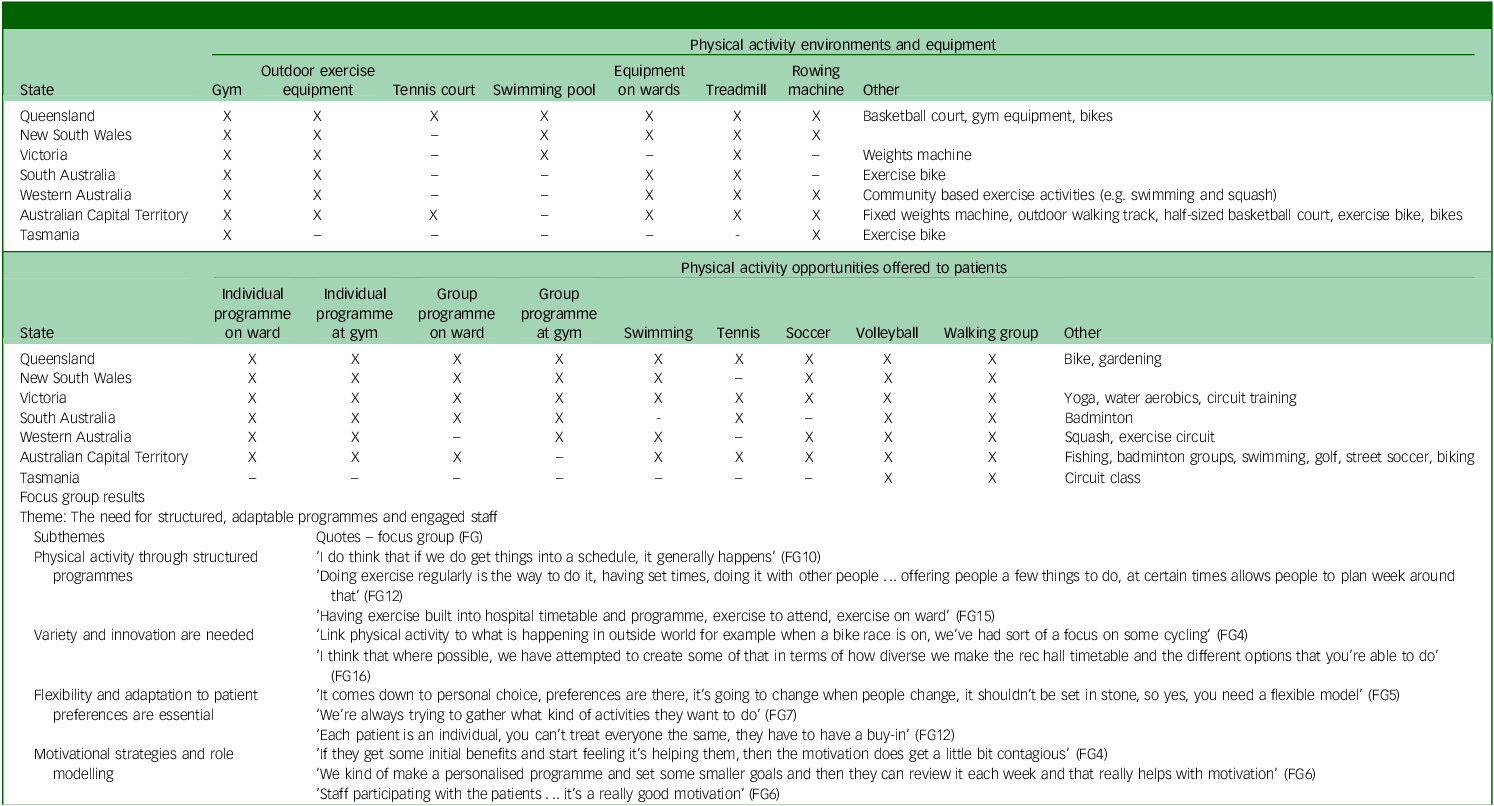
Physical activity environments, equipment and opportunities for patients under forensic mental healthcare

X, endorsed by at least one participant from forensic hospital in state/territory; –, no survey participants from the site endorsed this response.
Quantitative survey responses were integrated with qualitative focus group themes to provide contextual information and illustrate variability in practices across hospitals. Percentages indicate the proportion of survey participants reporting awareness of specific practices and are presented alongside thematic qualitative findings to augment interpretation. In Tables 3 to 5, a dash (–) indicates that no survey participants from a given site endorsed the response.
Our thematic analysis identified eight key themes: (a) lack of a standardised approach to physical health and activity; (b) inconsistent monitoring and documentation; (c) importance of general practitioners (GPs) and multidisciplinary teams (MDTs); (d) need for structured, adaptable programmes and engaged staff; (e) challenges related to patients, staff, ethics and infrastructure; (f) gaps in education, engagement and awareness; (g) need to balance nutrition and eating autonomy; and (h) importance of developing and implementing interventions.
Lack of a standardised approach to physical health and activity
Table 2 presents the anthropometric, physiological, and lifestyle measures that participants reported as being recorded upon admission and during monitoring. The number (n) associated with each measure represents the number of respondents who indicated that the specific measure was conducted. Despite variability in responses from staff within the same facility, the data are still informative. The most common measures taken on admission and monitoring included blood pressure (admission: 68.2%, monitoring: 59.1%), resting heart rate (admission: 59.1%, monitoring: 45.5%), weight (admission: 59.1%, monitoring: 45.5%), height (admission: 54.5%, monitoring: 68.2%), body mass index (admission: 54.5%, monitoring: 31.8%) and full blood count (admission: 50%, monitoring: 31.8%). Two hospitals with exercise physiologists reported taking a physical activity history on admission. Additional tests such as vitamin B12, folate and strength assessments were also reported by a small number of participants. Survey and focus group data highlighted challenges in physical health assessments, including inconsistent responsibilities, variability in measures and limited use of fitness assessments. More than half of the participants were unaware of whether physical activity data were collected, although two hospitals used objective activity measures like the 6-min walk test, International Physical Activity Questionnaire and Simple Physical Activity Questionnaire, alongside other tests such as the Astrand Test and strength tests.
Inconsistent monitoring and documentation
Table 3 presents findings on physical health monitoring practices. Staff from four hospitals reported recording metabolic monitoring data in both electronic and paper records, and staff from four hospitals also reported using a specific metabolic monitoring form, although only one participant indicated consistent use of this form.
Health monitoring frequency varied widely, with responses ranging from ‘unsure’ to specific time frames like ‘3–6 months’ or ‘monthly’. Some participants also used more general terms like ‘regularly’ or ‘on request’. Focus group discussions further revealed uncertainty about practices, inconsistent documentation and a lack of data system integration. Staff from Queensland, South Australia and Western Australia noted that regular data collection (e.g. body mass index) had discontinued, creating gaps in monitoring and evaluating patient health trends.
The importance of GPs and MDTs
Survey responses outlining staff involvement in supporting physical health assessments and interventions across forensic hospitals are summarised in Table 4. There was variability noted across states/territories. A range of staff occupations were reported to provide support for physical health assessments, with psychiatrists, GPs and nursing staff being the most frequently endorsed roles. Physical health interventions saw broader participation from allied health professionals, with notable involvement from exercise physiologists, occupational therapists and physiotherapists in several states/territories.
Survey and focus group responses emphasised the collaborative efforts of the MDT in supporting patients’ physical health and activity. Allied health professionals, nursing staff and other team members work together to provide physical activities and support such as gym access, group activities and tailored exercise programmes. Access to GPs was viewed as essential for effective physical health monitoring. Exercise physiologists were seen as vital for tailoring physical activity programmes to patients’ needs. Physical health was discussed in MDT meetings, but its prioritisation varied. Although some teams included physical health as a key domain in care planning and reviewed it regularly, other teams reportedly did not prioritise it unless raised by specific MDT members.
The need for structured, adaptable programmes and engaged staff
Table 5 outlines the physical activity environments and equipment available in forensic hospitals. All seven hospitals (n = 7) reported having access to a gym, and six provided outdoor exercise equipment. Less common facilities included tennis courts (n = 2) and swimming pools (n = 3). Other available equipment included stationary options such as treadmills (n = 6) and rowing machines (n = 5), as well as basketball courts, bicycles and weight machines.
A variety of individual and group programmes were offered, with all hospitals providing walking groups and volleyball. Six hospitals offered individual programmes and five provided group programmes, both on the ward and at the gym. Team sports like tennis and soccer, along with specialised activities such as badminton, yoga and water aerobics, were available in some settings.
Survey and focus group data emphasised the need for structured and adaptable activities that align with patient preferences to foster engagement. A mix of scheduled and spontaneous activities was seen as effective, with walking and volleyball being popular. Participants also highlighted the role of motivational strategies and role modelling in improving patient participation.
Challenges related to patients, staff, ethics and infrastructure
Table 6 highlights the challenges of managing forensic patients’ physical health. Staff identified a range of patient-related barriers including low motivation, poor self-esteem, illness-related symptoms, body image concerns and gender issues.
Staff perspectives on managing patients’ physical health and activity in forensic hospitals

Lack of staff, resources and infrastructure to support physical health initiatives was a noted subtheme. Staffing shortages and limited access to GPs, dietitians, physiotherapists and exercise physiologists affect physical health initiatives. Infrastructure changes, such as a change to a multi-story building, may further restrict access to physical activities.
Another subtheme was the tension related to balancing patient autonomy with institutional policy and ethical considerations. Examples of concerns raised included restrictions on food at activities, balancing patient choice with structured exercise mandates and balancing patient autonomy with institutional policies.
Forensic hospitals face challenges in balancing mental and physical healthcare, with focus group participants noting that physical health and activity are often deprioritised with mental health and risk management takes precedence over physical health.
This challenge is further underscored by the impact of risk concerns on both assessment and physical activity opportunities. Safety issues have restricted access to outdoor activities and gyms, although limitations on equipment (e.g. free weights, therabands, and boxing) have reduced the range of physical activity options available.
Finally, organisational barriers, including scheduling conflicts, movement restrictions and delays in equipment repairs, further complicate the integration of physical activity into patient care.
Gaps in education, engagement and awareness
Gaps in education, engagement and awareness hinder physical health promotion in forensic hospitals, as outlined in Table 6. Challenges include inconsistent and inaccessible physical health education for patients. Although some staff integrate education into group programmes and develop resources, there is no standardised approach. Staff noted that education should be ongoing. One participant noted that providing health information can sometimes disempower patients who have limited control over their treatment.
Patient and carer involvement in education and physical health initiatives was limited. Survey data showed that many participants did not provide information about obesity risks related to the forensic environment (40.9%). About half were unsure or provided no answer, whereas 31.8% reported offering general health education, including food choices and medication side-effects. Staff were more likely to discuss strategies for improving health outcomes (68.2%). Staff reported varying levels of confidence in supporting patients’ physical health, suggesting that there is a need to improve staff confidence. Implementing more structured education, targeted training and clear procedures such as those for metabolic monitoring and medication management were offered as strategies that could enhance staff competence and foster greater health promotion.
There was a lack of awareness of physical activity guidelines, and most survey participants were unsure about patient adherence to physical activity recommendations.
The need to balance nutrition and eating autonomy
Staff consistently highlighted challenges related to nutrition and autonomy (Table 6). Issues around food choice and institutional influence highlighted the limited control staff had over food provision as well as the role of ‘buy-ups’ and the focus of leave being related to food. There was growing recognition of the need for dietitians to improve patient dietary care.
Education on healthy eating for both staff and patients was another subtheme. Staff valued prior training on using non-stigmatising language around food and suggested more individual and group discussions to improve food literacy.
A shift away from food-based incentives toward alternative motivators was also suggested. Staff noted that they had historically reinforced unhealthy eating habits by facilitating extra snack requests and allowing poor food choices, often as a way to compensate for patients’ restricted freedoms.
Balancing eating autonomy with dietary health posed ethical challenges for staff. Some staff argued that the right to eating autonomy must be balanced with the duty of care, as evidence shows that forensic patients often gain weight, which increases cardiometabolic risk and leads to poorer health outcomes.
The importance of developing and implementing interventions
Staff reported limited trials of structured lifestyle interventions and emphasised the need for better implementation and evaluation (Table 6). Staff highlighted lessons from past programmes, noting challenges in execution and measuring effectiveness. Specific initiatives such as Group Occupation, Health, Exercise and Rehabilitation Treatment (GO HEART) and Self-directed Treatment for Obesity Reduction and Diabetes Education (STRIDE) were mentioned, along with a Fitbit-based intervention that successfully increased activity levels, reduced metabolic age and encouraged sustained gym participation.
Several forensic hospitals were expanding health and activity initiatives. The High Secure Inpatient Service in Queensland planned to pilot the Healthy Eating Active Lifestyle (HEAL) programme, integrating nutrition and exercise. The Dhulwa Secure Mental Health Unit in the Australian Capital Territory recently established a physical health group to develop new interventions, whereas the Forensic Hospital in New South Wales has established a metabolic clinic to support patients at risk of, or diagnosed with, metabolic syndrome.
Discussion
Our findings contribute to the growing literature focussing on the health of forensic in-patients. From survey and focus group responses eight themes emerged: (a) lack of a standardised approach to physical health and activity; (b) inconsistent monitoring and documentation; (c) importance of GPs and MDTs; (d) need for structured, adaptable programmes and engaged staff; (e) challenges related to patients, staff, ethics and infrastructure; (f) gaps in education, engagement and awareness; (g) need to balance nutrition and eating autonomy; and (h) importance of developing and implementing interventions.
No forensic hospital had a clear, comprehensive approach to health assessment and monitoring. Assessments are challenging, as individuals are often severely unwell at admission, making physical examinations and blood tests difficult. Current recommendations include physical health screening as soon as feasible, ideally within 24 h of admission. Guidelines from New South Wales Health, the Royal Australian and New Zealand College of Psychiatrists and expert consensus statements outline minimum standards for screening, including body mass index, waist circumference, blood pressure, glucose regulation, fasting lipids and blood-borne viruses. 11,Reference Galletly, Castle, Dark, Humberston, Jablensky and Killackey22,Reference Lambert, Reavley, Jorm and Oakley Browne23 Online survey results indicated these standards were not being met, with waist circumference monitoring reported in less than half of surveyed hospitals.
Staff from two forensic hospitals reported using a physical assessment template. Similarly, staff from four forensic hospitals noted the availability of a specific metabolic monitoring form, yet only one participant reported consistent use. Although adherence with metabolic monitoring has been studied in general psychiatric populations, no known research has focused specifically on forensic settings. Reference Benson, Kisely, Korman and Moss26,Reference Tso, Kumar, Jayasooriya, Kisely and Siskind27 Studies indicate that simple interventions, such as staff training and education, can improve monitoring rates. Reference Michael and MacDonald28 Some services recorded metabolic monitoring in both electronic records and paper charts, leading to duplication. Innovative technological solutions such as integrated platforms with automated reminders for due assessments and alerts for out-of-range measures could enhance adherence and streamline documentation.
A key finding of this research is the need for greater staff expertise. This aligns with recent calls from Dietitians Australia and Exercise and Sports Science Australia for expanded access to accredited exercise physiologists and practicing dietitians as part of comprehensive mental health treatment plans. 29 Participant responses highlighted that services with exercise physiologists were better equipped to offer a broader range of physical activities and more personalised interventions. Recent research supports the role of exercise physiologists and dietitians in delivering lifestyle interventions for individuals with mental illness. Reference Korman, Fox, Skinner, Dodd, Suetani and Chapman30,Reference Wynaden, Barr, Omari and Fulton31 Although exercise physiologists contribute specialised expertise in physical activity prescription within Australian forensic services, this professional role is not universally available across international settings. In other jurisdictions, similar functions may be undertaken by other health professional such as physiotherapists, occupational therapists or nursing staff with additional training in physical activity and health promotion. Regardless of professional background, the presence of staff with dedicated expertise in physical activity prescription appears critical to addressing the substantial physical health burden experienced by forensic in-patients.
A range of barriers to engagement in physical activity including patient-related factors (motivation, self-esteem and illness-related symptoms) were identified by staff. This is in line with patient perspectives who noted that lack of motivation and resourcing, staffing issues and problems with equipment hindered engagement. Reference Moss, Meurk, Steele and Heffernan18 Forensic hospitals face challenges in prioritising physical health. Risk concerns affect physical activity initiatives, restricting outdoor and gym access, and limiting equipment options. Organisational barriers, such as scheduling conflicts, patient movement restrictions and delays in equipment repairs, further hinder the integration of physical activity into care. Reference Anthony, Papathomas, Annandale, Breen and Kinnafick17
Concerns about human rights and patient autonomy in forensic mental health settings have been highlighted. Reference Johnson, Day, Moholkar, Gilluley and Goyder32,Reference Markham33 These issues were raised by focus group participants, particularly regarding patient food choices, restrictions on kiosk access and participation in physical activity interventions. There is a growing shift away from using food as an incentive and toward implementing strategic, organisation-wide policies that balance patient autonomy with health promotion. Research on diet and nutrition within forensic populations remains limited, requiring services to rely on findings from general hospitalised populations. Reference Osman, Md Nor, Md Sharif, Hamid and Rahamat34 Efforts to modify food access must carefully consider ethical implications while ensuring that interventions are evidence-based and promote long-term health improvements.
Forensic hospitals should consider adapting evidence-based lifestyle interventions from general mental healthcare. Reference Moss, Meurk, Steele and Heffernan15 For example, HEAL, part of the Australian Government’s Healthy Communities Initiative, has demonstrated significant benefits, including increased physical activity, reduced sitting time, improved diet and reductions in body mass index, waist circumference and blood pressure. Reference Hetherington, Borodzicz and Shing35 Given the well-documented challenge of low motivation among individuals with mental illness, forensic hospitals must actively implement techniques such as positive encouragement to foster sustained participation. Reference Bacon, Farnworth and Boyd36–Reference Verhaeghe, De Maeseneer, Maes, Van Heeringen and Annemans38 Autonomy-supportive approaches, which allow patients some control over their activity choices, have been shown to enhance motivation. Reference Beebe, Smith, Burk, McIntyre, Dessieux and Tavakoli39,Reference Vancampfort, Stubbs, Venigalla and Probst40 The MDT plays an important role in fostering motivation through structured goal-setting, continuous support and reinforcing progress.
This study has several limitations. The online survey relied on self-reported data, making it susceptible to recall bias and participants’ reflective perceptions rather than verified site information. Responses to some survey questions showed substantial variability both within and across sites, particularly in relation to staffing levels, thereby limiting the reliability of quantitative findings for certain themes. Although 63 responses were missing across the 25 survey questions, analyses were based on the available data for each question. Given the presence of multiple respondents per site and the assumption that missing responses largely reflected individual knowledge gaps rather than systematic non-response, the impact of missing data on overall findings is likely minimal. In addition, participation was voluntary, and respondents may therefore not be fully representative of all forensic hospital staff. Although survey and focus group participants were broadly similar in professional roles, quantitative and qualitative data were collected from different individuals, which may have influenced the perspectives captured. Further, while the integration of survey and focus group findings enabled a more comprehensive interpretation of hospital practices, the combined presentation of quantitative data and qualitative themes reflects participants’ knowledge and perceptions rather than objective verification, and should be interpreted accordingly. Finally, the focus groups provided valuable qualitative insights, but they were also limited by sample size and may not have fully captured the diversity of experiences across forensic hospitals. This study did not include direct patient perspectives; however, patient views and experiences have been explored in prior research. Reference Anthony, Papathomas, Annandale, Breen and Kinnafick17,Reference Moss, Meurk, Steele and Heffernan18
Future research could focus on evaluating physical health monitoring practices in forensic hospitals, including the effectiveness of electronic health record integration in improving documentation, adherence and follow-up care. Assessing the impact of targeted training programmes on staff confidence, knowledge and adherence with physical health screening and intervention protocols could be another key area of inquiry. Longitudinal studies could explore the long-term health trajectories of forensic patients, comparing those who receive structured physical health interventions with those who do not, to assess their impact on health outcomes, lifestyle measures, morbidity and mortality. Comparative research across jurisdictions could help identify best practices and highlight areas for improvement, with the development of key performance indicators facilitating meaningful cross-site evaluations. Benchmarking of key performance indicators is promoted in the mental health field as a means of improving service quality. Reference Meehan, Stedman, Neuendorf, Francisco and Neilson41 However, benchmarking physical health and activity has not yet formally been undertaken in Australia.
In conclusion, our study highlights the need for systemic reforms in forensic hospitals to ensure consistent physical health assessment and monitoring, better integration of multidisciplinary care and enhanced patient engagement. To successfully integrate improved physical health management into forensic hospitals, a collaborative and multifaceted approach is required, combining policy reform, resource investment, workforce training and patient-centred programme design. It is recommended that key performance indicators be developed to monitor service quality and outcomes, with the aim of enhancing patient care through increased accountability and a focus on continuous improvement.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.12013
Data availability
The data-sets used and/or analysed during the current study are available from the corresponding author, K.M., on reasonable request.
Acknowledgements
The authors wish to thank the staff participants, who contributed their time and provided specialist knowledge to this study, from the following forensic hospitals: High Secure Inpatient Service (Queensland), Forensic Hospital (New South Wales), Thomas Embling Hospital (Victoria), James Nash House (South Australia), Frankland Centre (Western Australia), Dhulwa Secure Mental Health Unit (Australian Capital Territory) and Wilfred Lopes Centre (Tasmania). Gratitude is also expressed to the following site coordinators for their support for the study: Dr Angela Voita (Queensland); Dr Andrew Ellis and Law Edwards (New South Wales); Dr Jacques Claassen, Dr Anthony Hew and Isaac Daramola (Victoria); Dr Owen Haeney (South Australia); Dr Elizabeth Tate and Samantha Amato (Western Australia); Dr Ahmed Mashood (Australian Capital Territory); and Darren West and Amy Mansell (Tasmania).
Author contributions
All authors listed contributed to the review article and are in agreement with the manuscript. K.M. contributed to study conceptualisation, methodology, data curation, analysis and interpretation, and wrote the original draft of the manuscript. C.M. contributed to study methodology, analysis and interpretation, verification and supervision, and reviewing and editing the manuscript. M.L.S. contributed to study supervision, analysis and interpretation, and reviewing and editing the manuscript. E.H. contributed to study supervision and and reviewing and editing the manuscript.
Funding
K.M. was awarded the Royal Australian and New Zealand College of Psychiatrists Early Research Career Grant (2022000131), which funded the site visits.
Declaration of interest
None.




 Open access
Open access
eLetters
No eLetters have been published for this article.