
Introduction
The following exercise is a case study of a girl (‘Rachel’) with cleft palate who was studied by Howard (Reference Howard1993). Rachel has grossly impaired speech and a severely reduced phonological system. Yet, she retains a high level of intelligibility. Her speech disorder has only been minimally responsive to prolonged therapy. The case study is presented in five sections: primer on cleft lip and palate; speech, language and hearing in cleft lip and palate; client history; focus on phonological analysis – part 1; and focus on phonological analysis – part 2.
Primer on cleft lip and palate
Cleft lip and palate is a congenital malformation of the upper lip and gum and hard and soft palates. A cleft of the lip can be complete, extending through the lip and into the nose, or incomplete, involving a variable degree of notching of the lip. A cleft lip may be unilateral or bilateral as is shown in Figure 1.1. A cleft of the palate may also be complete or incomplete. In a complete palatal cleft, the cleft extends the full length of the palate. In an incomplete palatal cleft, the cleft may involve just the uvula and soft palate. A palatal cleft may also be submucous (see Case study 2 for further discussion). Several methods of classifying cleft lip and palate have been proposed. A system that continues to be used in many cleft centres is the one proposed by Kernahan and Stark (Reference Kernahan and Stark1958). This system recognises the embryological division of the primary and secondary palates at the incisive foramen. If a palatal cleft occurs in front of the incisive foramen, it is called a primary palate or prepalate cleft. If a palatal cleft occurs behind the incisive foramen, it is called a secondary palate or simply palate cleft. Primary palate clefts may be unilateral (left or right), bilateral or median. Figure 1.2 shows different types of palatal clefts.
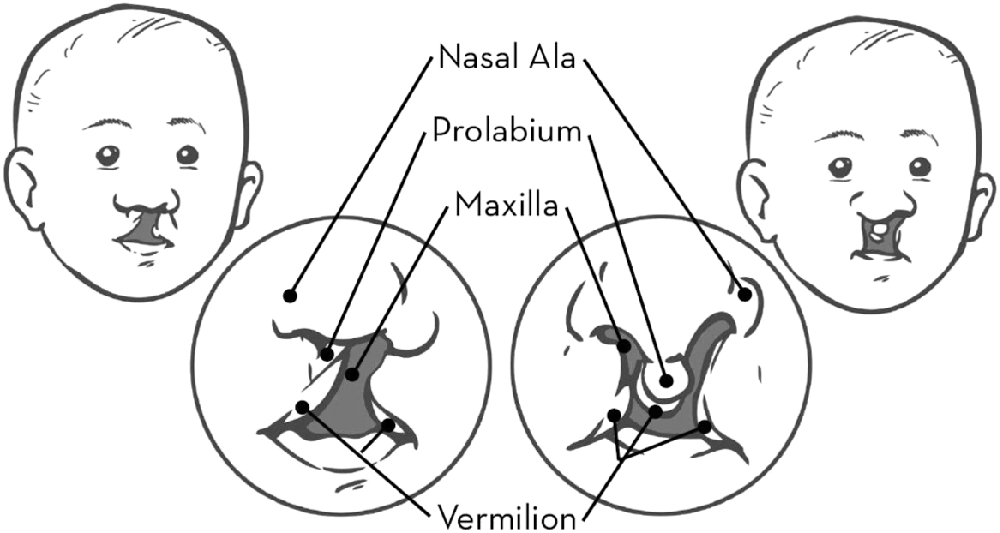
Figure 1.1 Unilateral and bilateral cleft lip and nose.
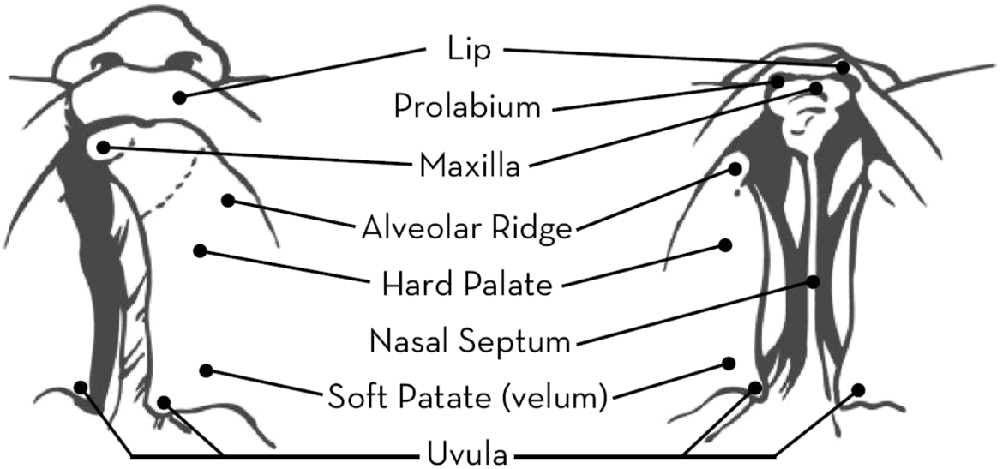
Figure 1.2 Unilateral and bilateral cleft palate.
Some forms of cleft are more common than others. Cleft lip and palate is the most common diagnosis, accounting for 46% of cases. Isolated cleft palate and isolated cleft lip account for 33% and 21% of cases, respectively. Unilateral clefts are nine times as common as bilateral clefts. They also occur twice as frequently on the left side than on the right (Hopper et al., Reference Hopper, Cutting, Grayson and Thorne2007). The epidemiology of cleft lip and palate has been extensively investigated. Matthews et al. (Reference Matthews, Oddone-Paolucci and Harrop2015) examined the epidemiology of cleft lip and palate in Canada between 1998 and 2007. The mean birth prevalence was 0.82 per 1,000 live births for cleft lip with or without cleft palate, and 0.58 per 1,000 live births for cleft palate. Cleft lip with or without cleft palate was significantly higher in boys, with a boy to girl ratio of 1.75:1. Cleft palate was significantly greater in girls, with a boy to girl ratio in 2007 of 0.59:1. The incidence of oral clefts varies among different ethnicities. Saad et al. (Reference Saad, Parina, Tokin, Chang and Gosman2014) found that the incidence of any cleft disease was highest in the white (non-Hispanic) population in the state of California at 16.2. Lower incidence rates were reported in the Hispanic population (12.26), Asian/Pacific Islanders (11.57), the African American population (8.9) and the Native American population (8.15).
The exact causes of cleft lip and palate are still unknown. What is clear is that genetic factors and environmental teratogens increase the likelihood that a child will develop a cleft. Several genes have been implicated in the aetiology of orofacial clefts (Simioni et al., Reference Simioni, Araujo, Monlleo, Maurer-Morelli and Gil-da-Silva-Lopes2015). Cleft lip and palate is also a clinical feature of many genetic syndromes. The most common syndrome associated with cleft lip and palate is van der Woude syndrome. Isolated cleft palate is most commonly associated with microdeletions of chromosome 21, resulting in velocardiofacial, DiGeorge, or conotruncal anomaly syndromes (Hopper et al., Reference Hopper, Cutting, Grayson and Thorne2007). Several teratogens and other environmental factors have been implicated in the aetiology of cleft lip and palate. Reduced folic acid levels, alcohol consumption, active and passive smoking, and antiepileptic drugs (e.g. topiramate) have all been associated with non-syndromic cleft lip and palate (Bezerra et al., Reference Bezerra, Oliveira, Soares, Cardoso, Ururahy, Neto, Lima-Neto, Luchessi, Silbiger, Fajardo, Oliveira, Almeida, Hirata, Rezende and Hirata2015; Margulis et al., Reference Margulis, Mitchell, Gilboa, Werler, Mittleman, Glynn and Hernandez-Diaz2012; Sabbagh et al., Reference Sabbagh, Hassan, Innes, Elkodary, Little and Mossey2015).
Unit 1.1 Primer on cleft lip and palate
(1) Respond with true or false to each of the following statements about cleft lip and palate:
Cleft lip and palate is an embryological malformation that arises in the first trimester of pregnancy.
Cleft lip and palate is a clinical feature of Pierre Robin syndrome.
An isolated cleft palate is more common in boys than in girls.
Cleft lip and palate is a clinical feature of Down's syndrome.
A bilateral cleft lip results in isolation of the prolabium.
(2) A cleft of the palate can be submucous in nature. Describe this type of cleft.
(3) Why do you think it is important for speech-language pathologists to know if a child has a syndromic cleft of the palate?
(4) There is considerable discussion about the optimal timing of surgical repair of a cleft of the palate. What two factors are central to the debate about the merits and disadvantages of early versus late palatal surgery?
(5) On account of its embryological significance, the incisive foramen is an important anatomical landmark in the classification of cleft lip and palate. Which of the following statements is true of the incisive foramen?
The incisive foramen is located in the maxilla bone.
The incisive foramen transmits blood vessels between the nasal cavities.
The incisive foramen transmits blood vessels and nerves between the nasal and oral cavities.
The incisive foramen is located in the midline of the palate posterior to the central incisors.
Speech, language and hearing in cleft lip and palate
Speech-language pathologists and audiologists must assess and treat the speech, language and hearing impairments that occur in cleft lip and palate. The primary speech defect is hypernasal speech related to velopharyngeal incompetence, although abnormal dentition and the presence of fistulae can also have phonetic consequences during speech production. Phonetic anomalies may have an adverse impact on a child's developing sound system (i.e. phonology). For example, the child who adopts a backed pattern of articulation in an effort to achieve closure and a build-up of air pressure in the vocal tract may eventually adopt backing as an organising principle within his system of sound contrasts. Such a child has a phonological disorder as well as a phonetic disorder. In a study of 80 children aged 6–15 years with cleft lip and palate, Albustanji et al. (Reference Albustanji, Albustanji, Hegazi and Amayreh2014) reported speech abnormalities including articulation and resonance deficits in 74% of subjects. Productive phonological processes in these children were consonant backing, final consonant deletion, gliding and stopping.
Although speech can improve following palatal surgery, phonetic and phonological defects may persist for many years. Nyberg et al. (Reference Nyberg, Peterson and Lohmander2014) examined the speech of 69 children who had a one-stage palatal repair at a mean age of 13 months. At 5 years of age, more than mild hypernasality, weak pressure consonants and perceived incompetent velopharyngeal function were present in 19 to 22% of children. This improved to less than 5% at 10 years of age. Audible nasal air leakage was present in 23% at 5 years and did not improve by 10 years. Frequent or persistent compensatory articulation was present in 30% at 5 years of age and in 6% at 10 years. At 5 years, 57% of children gave an impression of normal speech. This increased to 89% at 10 years. A high prevalence of distorted /s/ was present in these children at 5 and 10 years of age.
Children with cleft lip and palate often experience expressive language delay. Morris and Ozanne (Reference Morris and Ozanne2003) reported delayed expressive language in 9 of 20 cleft children aged 3 years. Eight of these children achieved a mean length of utterance (MLU) which was below average for their age. There is considerable evidence of delayed lexical development in children with cleft palate. Hardin-Jones and Chapman (Reference Hardin-Jones and Chapman2014) found that the size of the expressive lexicon of toddlers with cleft palate was significantly smaller than that of a noncleft group at 21 and 27 months of age. Discourse deficits have also been reported in children with cleft palate. Klintö et al. (Reference Klintö, Salameh and Lohmander2015) examined narrative retelling in 29 children with unilateral cleft lip and palate. An information score below 1 standard deviation from the norm value was obtained by 65.5% of these children. This compared with 30% in a comparison group of children. Several studies have found evidence of reading impairments in children with cleft palate. Conrad et al. (Reference Conrad, McCoy, De Volder, Richman and Nopoulos2014) found that subjects with non-syndromic cleft of the lip and/or palate performed significantly worse on a test of word reading than control subjects. Word reading deficits were not associated with measures of speech or hearing, but were correlated with auditory memory impairments.
Hearing loss is commonly found in children with cleft palate. In a retrospective audit of 123 newborns with cleft deformities, Tan et al. (Reference Tan, Hee, Yeoh, Lim, Tan, Yeow and Daniel2014) reported the incidence of hearing loss to be 24.4%. This was significantly higher than the hospital incidence of 0.3%. Hearing loss is most often conductive in nature and is associated with the development of otitis media with effusion. However, sensorineural hearing loss can also occur, particularly in children with syndromic cleft palate. Ventilation tube insertion is beneficial to the recovery of hearing in children with cleft palate and otitis media with effusion (Kuo et al., Reference Kuo, Tsao, Cheng, Lien, Hsu, Huang and Shiao2014). However, even after the placement of tubes, hearing loss may persist. Chen et al. (Reference Chen, Messner and Curtin2008) reported that of 30 newborns who failed hearing screening and had tympanostomy tubes placed, 43% had persistent hearing loss. Factors, which predicted persistent hearing loss, were cleft palate alone, female infants and the presence of an associated syndrome.
Unit 1.2 Speech, language and hearing in cleft lip and palate
(1) Which of the following factors is associated with velopharyngeal incompetence in children with cleft palate?
(2) Explain why the oral plosives /p, b, t, d, k, g/ are often substituted by the glottal stop /ʔ/ in the speech of children with cleft palate.
(3) In their study of the expressive lexicon in children with cleft palate, Hardin-Jones and Chapman (Reference Hardin-Jones and Chapman2014) reported that toddlers with cleft palate produced significantly more words beginning with sonorants and fewer words beginning with obstruents in their spontaneous speech samples. Why do you think this is the case?
(4) Give three reasons why children with cleft palate are at risk of language delay.
(5) Respond with true or false to each of the following statements about otitis media with effusion (OME) in children with cleft palate:
Client history
Rachel is 6 years old. She was born 11 weeks prematurely with a central cleft of the hard and soft palates. At 2;2 years, she underwent surgical repair of her palatal cleft. Rachel has a severe speech disorder, although her receptive language and expressive language have developed normally. Rachel has a history of fluctuating, mild to moderate, conductive hearing loss (average 45–55 dB). At 3;0 years, grommets were inserted. These were inserted again at 4;0 years. Auditory ability improved significantly following grommet insertion. At 5;11 years, T-tubes were inserted with reported improvements in hearing levels. Notwithstanding improvements in hearing, Rachel's performance in assessments of auditory discrimination for speech sounds remained inconsistent. There was no evidence of either oral apraxia or developmental apraxia of speech.
Rachel had received speech therapy for approximately three years by the time of the study. However, her speech problems had remained largely resistant to change and little progress had been made in therapy. There was also concern that Rachel had reached a plateau and that any further change in her speech would be difficult for her to achieve. Rachel had deficits across several aspects of speech production. She had difficulty initiating, maintaining and coordinating phonation. Her voice was breathy and she displayed high pitch. In relation to resonance, she exhibited hypernasality, nasal emission and nasal friction. A pharyngoplasty was performed at 5;5 years. However, it had had little effect in reducing her nasal emission. In terms of articulation, Rachel displayed glottalisation of consonants. There was also a lack of alveolar and post-alveolar segments in her speech. Rachel exhibited greater difficulty with the articulation of obstruents than nasals and approximants.
Unit 1.3 Client history
(1) Which feature of Rachel's history is frequently found in newborns with oral clefts?
(2) Is Rachel's cleft type consistent with the findings of studies of sex differences in clefting?
(3) Respond with true or false to each of the following statements about grommets and T-tubes:
Both devices are used to treat Eustachian-tubal insufficiency.
Grommets remain in situ for longer than T-tubes.
Both devices reside in the middle ear.
Both devices are naturally extruded by the tympanic membrane.
T-tubes are used when multiple grommet insertions have failed to provide adequate middle ear ventilation.
(4) Rachel had a breathy voice quality and other phonatory disturbances. Why are children with cleft palate at an increased risk of voice disorder?
(5) At 5;5 years, Rachel underwent a pharyngoplasty. Describe this procedure and state what it is intended to achieve.
Focus on phonological analysis – part 1
Audio- and video-recordings were made of Rachel's speech production during two clinical sessions over a period of five days. To obtain comprehensive coverage of the entire phonological system, the Sheffield Test of Phonetics and Phonology (Eastwood, Reference Eastwood1981) was used. The nearly 100 words from this test were supplemented by words recorded during spontaneous speech and picture description tasks. A detailed phonetic transcription of all words was completed. Symbols from the IPA and extensions to the IPA were used in the transcription. Following transcription, the PACS framework (Grunwell, Reference Grunwell1985) was used to carry out a phonological analysis of Rachel's speech. The data that was used in this analysis is examined in this unit and in the next unit.
Phonotactic structure
| glasses | [ˈɴᴡæç͋əç͋] |
| string | [ˈʩɁωɪɴ] |
| matches | [ˈmaɁjəħ͋] |
Oral–nasal contrast
| letter | [ˈɰeɁə] | nose | [ɴəʊҫ͋] |
| ladder | [ˈɰæɁə] | ring | [ʊɪɴ] |
| sugar | [ˈҫ͋ʊɁə] | fine | [f͉:aɪɴ] |
| down | [Ɂaʊɴ] | penny | [ˈp͡ʔeɴɪ] |
| dog | [ɁɒɁʰ] | singing | [ˈҫ͋ɪɴɪɴ] |
| cat | [ɁæɁʰ] | teaspoon | [ˈʔiҫ͋ᵬuɴ] |
Bilabials
| pig | [ʘɪʔʰ] | mud | [məʔʰ] |
| pen | [ʔeɴ] | mum | [məm] |
| tap | [ʔæʔ͡ʘ] | mouth | [maʊɵ] |
| paper | [ˈp͡ʔeɪp͡ʔə] | thumb | [ɵəm] |
| big | [mɪʔʰ] | jam | [ʔjæm] |
| baby | [ˈᵬeɪbɪ] | hammer | [ˈħæmə] |
| bike | [maɪʔʰ]/[ᵬaɪʔʰ] | shop | [ҫ͋jɒp̃ʰ] |
Unit 1.4 Focus on phonological analysis – part 1
(1) Describe the phonotactic structures of the words ‘glasses’, ‘string’ and ‘matches’. Is Rachel able to replicate these structures in her spoken productions? What does your answer to this question reveal about Rachel's phonological knowledge?
(2) Is Rachel able to maintain a broad oral–nasal contrast in her use of alveolar segments? Use examples from the above data to support your response.
(3) Is Rachel able to maintain a broad oral–nasal contrast in her use of velar segments? Use examples from the above data to support your response.
(4) Is there any similarity in the way in which Rachel realises alveolar and velar segments and the way in which she realises bilabial segments? What additional clue does Rachel provide for listeners to assist them in the identification of target bilabial segments? Use examples from the above data to support your response.
(5) Not all of Rachel's bilabial segments are realised as glottal stops. In what other ways are bilabial segments realised within her speech? What do most of these realisations have in common? One realisation is particularly unusual. Which one is it, and why do you think it occurs?
Focus on phonological analysis – part 2
Several other aspects of the manner of articulation were examined in Rachel's speech. They included her ability to signal the stop–fricative–approximant continuum and the stop–affricate continuum. These continua tell us something about Rachel's ability to signal the difference between open and close sounds and, in the case of the stop–affricate continuum, the timing of release of closure. Contrasts of place of articulation and the voicing of segments were also examined.
Stop–fricative–approximant continuum and stop–affricate continuum
| tap | [ʔæʔʰ] | zip | [ҫ͋ɪʔʘ] |
| down | [ʔaʊɴ] | cup | [ʔʊʔʰ] |
| chair | [ʔjɛə] | go | [ʔəʊ] |
| jam | [ʔjæm] | yes | [jɛʔ] |
| sock | [ҫ͋ɒʔʰ] | why | [waɪ] |
| shop | [ҫ͋jɒp̃ʰ] |
Place of articulation
| baby | [ƀeɪbɪ] | bucket | [ˈƀʊʔɪʔʰ] |
| toy | [ʔɔɪ] | Sue | [ç͋u] |
| cat | [ʔæʔʰ] | daddy | [ˈʔæʔɪ] |
| tap | [ʔæʔʘ] | dog | [ʔɒʔʰ] |
| paper | [p͡ʔeɪp͡ʔə] | sugar | [ˈç͋ɬʊʔə] |
| kick | [ʔɪʔʰ] | shoe | [ç̫͋u] |
Voicing
| pig | [ʘɪʔʰ] | bib | [ƀɪb̥ʰ] |
| baby | [ˈƀeɪbɪ] | tea | [ʔi] |
| letter | [ˈɰeʔə] | ladder | [ˈɰæʔə] |
| Sue | [ç͋u] | zoo | [ç͋u] |
| watch | [wɒʔç͋] | jam | [ʔjæm] |
| four | [f͉ɔ] | a van | [ə ˈf͈æɴ] |
| feather | [ˈf͉eʋə] | laughing | [ˈæf͉ɪɴ] |
| dig | [ʔɪʔʰ] | chair | [ʔjɛə] |
| key | [ʔi] | fridge | [fʋɪʔħ] |
| go | [ʔəʊ] | cover | [ˈʔʊʋə] |
Unit 1.5 Focus on phonological analysis – part 2
(1) Is Rachel able to signal a contrast between stop, fricative and approximant sounds? Use examples to illustrate how she signals this contrast.
(2) Does Rachel succeed in signalling a contrast between stops and affricates? Support your answer with examples from the above data.
(3) Prior to speech therapy, alveolar and postalveolar fricatives had pharyngeal realisations in Rachel's speech. Does Rachel effectively signal an alveolar–postalveolar contrast between these sounds following therapy? In what way does Rachel's post-therapy production of alveolar and postalveolar fricatives represent an improvement on her pre-therapy production?
(4) Is Rachel able to signal a voicing contrast for bilabial, alveolar and velar plosives? Does Rachel succeed in signalling a phonological contrast between /f/ and /v/?
(5) Which of the following statements best characterises Rachel's speech production?
Rachel is severely unintelligible on account of her use of segments that are phoneti-cally distant from target phonemes.
Rachel is severely unintelligible because of a lack of consistency in her use of phonemes.
Rachel is severely unintelligible because she is unable to signal a number of phonological contrasts in her speech.
Rachel is more intelligible than expected because she makes consistent use of phonetically deviant phonemes.
Rachel is more intelligible than expected because she is able to signal a contrast between plosive and fricative sounds.
Introduction
The following exercise is a case study of a girl (‘Louise’) aged 3;8 years with Kabuki make-up syndrome who was studied by Van Lierde et al. (Reference Van Lierde, Van Borsel and Van Cauwenberge2000). Kabuki make-up syndrome is a rare genetic syndrome which is characterised by a dysmorphic face, postnatal growth retardation, skeletal abnormalities, intellectual disability and unusual dermatoglyphic (fingerprint) patterns (Matsumoto and Niikawa, Reference Matsumoto and Niikawa2003). For those with the disorder, speech, language and hearing can be adversely affected. The case study is presented in five sections: history and clinical presentation; clinical assessment; communication and cognition profile; focus on speech production; and clinical intervention.
History and clinical presentation
Louise is the second child of healthy, non-consanguineous parents. Her sister, who is 2 years older, is healthy. After a complicated pregnancy, Louise was born at 37 weeks of gestation weighing 2.610kg. A fetal right chylothorax was detected at 20 weeks of pregnancy. (A chylothorax is the presence of lymphatic fluid in the pleural space secondary to leakage from the thoracic duct or one of its tributaries.) Karyotyping by amniocentesis was undertaken and was found to be normal. At birth, Louise was observed to have a high-arched palate with a submucous cleft. She also exhibited generalised hypotonia. The following postnatal investigations were normal: an electroencephalogram, a computed tomography scan of the brain, electromyography and metabolic screening. An internal strabismus with mild nystagmus was revealed during an ophthalmologic examination. Louise had transtympanic drains fitted at 11 months, 18 months and 2 years. At 2;4 years, a hearing examination revealed pure-tone thresholds within the normal range. This examination was repeated at 3;0 years and again revealed normal hearing. Oto-acoustic emissions were also detected. A team of geneticists and dysmorphologists diagnosed Louise at 3;1 years as having Kabuki make-up syndrome (KMS). The diagnosis was based on the presence of facial characteristics (e.g. arched eyebrows), a high-arched palate with submucous cleft, fingertip pads, a foot deformity, broad thumbs, a mild to moderate delay in motor development, and postnatal growth deficiency. At 3;4 years, an assessment of motor skills showed Louise to be at percentile 1 on the gross and fine motor scales of the Peabody Developmental Motor Scales (Folio and Fewell, Reference Folio and Fewell1983). A slight, general hypotonia was also observed.
Unit 2.1 History and clinical presentation
(1) There is evidence of an otological abnormality in Louise's clinical history. You should (a) state what that evidence is, (b) indicate what type of hearing loss (conductive or sensorineural) is associated with the otological defect in question and (c) explain how the placement of transtympanic drains can serve to correct the hearing loss.
(2) The history states that oto-acoustic emissions were detected during a hearing examination. What is the significance of these emissions?
(3) Is Louise's middle ear defect related to her palatal abnormality? If you answer ‘yes’, provide an explanation.
(4) Is there any evidence in the history to suggest that Louise may experience a speech disorder of neurogenic aetiology?
(5) KMS is a genetic disorder. The American Speech-Language-Hearing Association (ASHA) states that as genetic research continues ‘it will become increasingly critical that audiologists and speech-language pathologists understand principles of genetics, genetic testing and genetic counselling’ (ASHA, 2005a). Describe one way in which knowledge of the genetics of this syndrome might assist a speech-language pathologist in understanding the features of Louise's clinical history.
Clinical assessment
The Dutch version of the McCarthy Developmental Scales (Van der Meulen and Smrkovsky, Reference Van der Meulen and Smrkovsky1986) was used to assess Louise's cognitive level. Language was assessed by means of the Dutch version of the Reynell Developmental Language Scales (Schaerlaekens et al., Reference Schaerlaekens, Zink and Van Ommeslaeghe1993). Louise's voice was assessed by an otorhinolaryngologist and two voice therapists. The otorhinolaryngologist conducted nasolaryngoscopy. The voice therapists used the GRBAS scale (Hirano, Reference Hirano1981) to assess Louise's voice. In order to determine the fundamental frequency of Louise's voice, she was asked to sustain the vowel /a/ for 4 seconds into a microphone. The instrumentation used in this analysis was the Multi-Dimensional Voice Program (model 4305) from Kay Elemetrics Corporation. A picture naming test which consisted of 135 black-and-white drawings of common objects and actions was used to assess Louise's articulation skills. The speech data obtained from this assessment were analysed independently of their relation to the adult targets as well as in relation to the adult standard forms. Three relational analyses were used: phonotactic analysis; phonetic analysis; and phonological process analysis.
Unit 2.2 Clinical assessment
(1) Which of the above tests is (a) a standardised assessment of receptive and expressive language, (b) a perceptually based assessment of voice and (c) an assessment of a child's IQ?
(2) One of the instrumental techniques used to assess Louise's voice was nasolaryngoscopy. Describe how this procedure is performed and what it may be used to assess.
(3) The fundamental frequency of Louise's voice was assessed. Which perceptual attribute of voice is fundamental frequency related to?
(4) Only common objects and actions were depicted by the drawings in the picture naming test. Why is this important?
(5) Which of the following statements best describes what is involved in a phonotactic analysis?
consonant and vowel productions are compared with target productions and ana-lysed for error types at the segmental level
an analysis is undertaken of the child's productions to establish if they retain the correct syllable structure of words
the child's productions are analysed for error types beyond the segmental level
Communication and cognition profile
Louise was found to have normal cognitive functioning. Her mean cognitive score was 98. Louise scored at the 60th percentile for receptive language on the Dutch version of the Reynell Developmental Language Scales. She was able to understand a range of named objects, verbs and adjectives. She was also able to respond correctly to instructions that involved an action–object semantic relation. Certain ‘wh’ questions were understood and there was evidence of emerging comprehension of passive sentences. However, it was still difficult for Louise to understand sentences such as ‘The dog is bitten by the rabbit’. Louise was able to understand utterances such as ‘John pushes the baby. Who is naughty?’, a number of spatial prepositions and some terms relating to the size of objects. She could also comprehend primary colours. Louise's expressive language skills exhibited strengths and weaknesses. She was at the 75th percentile in her ability to produce the names of items in the Reynell and to define concrete words (e.g. soap) and abstract words (e.g. being hungry). Louise performed at the 30–40th percentile on the expressive semantics subtest of the Reynell. She was able to express semantic relations of two elements (e.g. ‘prepare dinner’) during story telling based on pictures (e.g. setting the table). However, she was unable to capture the general theme of the depicted situations. Louise's worst area of expressive language (20th percentile) was her morphosyntactic abilities. Nouns, verbs and personal pronouns were the only word classes produced. She made use of singular and plural nouns, but did not use irregular plural forms. Louise also used some nouns with diminutive endings. Verbs only occurred in infinitive form. There were no examples of third-person singular verbs, past participles or future tense verbs. Compound sentences involving either coordination or subordination were completely absent. A negative sentence was occasionally produced. Louise's expressive output only contained sentences of two or three words, with an average of 2.4 words per sentence.
Nasolaryngoscopy failed to reveal any organic or functional voice disorder. Normal results were obtained on all perceptual and instrumental analyses of the voice. The results of the articulation assessment are examined below.
Unit 2.3 Communication and cognition profile
(1) Louise displayed relatively strong receptive language skills on the Reynell Developmental Language Scales. Based on the above description of these skills, how would you characterise her comprehension of each of the following items? kiss the doll; beside; smallest.
(2) Explain why Louise struggled to comprehend sentences like ‘The dog is bitten by the rabbit’ despite showing emerging comprehension of passive sentences.
(3) Louise was able to comprehend utterances such as ‘John pushes the baby. Who is naughty?’ Which of the following is suggested by her comprehension of these utterances?
Louise has intact comprehension of relative clauses.
Louise is able to understand semantic relations of two elements.
Louise is able to draw inferences based on language and world knowledge.
Louise has intact comprehension of subordinate clauses.
Louise has intact comprehension of locative prepositions.
(4) Louise's expressive language skills were most impaired in the area of morphosyntax. Based on the above description of these skills, which of the following forms was Louise able to produce and which forms did she not use? Explain your response in each case: will come; cups; mice; dog; gone; she; run; walks; John likes oranges and Mary likes apples.
(5) Louise was unable to capture the general theme of a depicted situation. Impairments of several cognitive and language skills might account for this difficulty. Which of the following deficits might explain Louise's specific difficulty in this area?
Focus on speech production
Phonetic inventory: Louise could correctly produce all Dutch vowels and 68% of Dutch consonants. She could not produce correctly the nasal /ɲ/ and the fricatives /f/, /v/, /ʃ/, /Ʒ/ and /h/.
Phonotactic analysis: Target syllables were usually retained. A change in syllable structure occurred in only 10% of words.
Phonetic analysis: Compared to target productions at the segmental level, 55% of Louise's consonants were in error and 21% of her vowels. Consonant errors included omissions, substitutions, distortions and additions. Substitutions were the most common error type. The most common types of distortion errors were dentalisation, labiodentalisation, devoicing, weak articulation, mild to moderate hypernasality and moderate nasal emission. Vowel errors included lowering, backing, neutralisation (replacement by a schwa) and unrounding of a target rounded vowel.
Phonological process analysis: Syllable structure processes are present including cluster reduction (affecting /s/-, /t/- and /R/-blends), final and initial consonant deletion (the former chiefly affecting final /k/) and deletion of unstressed syllables. The following substitutions were in evidence, some of which are shown in the table below.
(a) /p/ → /f/; /b/ → /v/; /k/ → /X/; /k/ → /s/; /t/ → /f/
(b) /s/ → /t/; /z/ → /b/
(c) /k/ → /t/; /ɣ/ → /p/
(d) /f/ → /j/
| Dutch word | English word | Phonemic norm | Client production |
|---|---|---|---|
| sigaret | cigarette | [siˠɑRɛt] | [sizɑRɛt] |
| boekentas | satchel | [bukəntɑs] | [pupətɑs] |
| fiets | bicycle | [fits] | [sis] |
| kapstok | clothes hanger | [kɑpstɔk] | [tɑtɔk] |
| zwart | black | [zwɑrt] | [vɑt] |
| gieter | watering-pot | [ˠitər] | [Ritə] |
| kraan | tap | [kra:n] | [ka:n] |
| kruis | cross | [krœYs] | [Xœys] |
| worsten | sausages | [wɔrstən] | [wəs] |
| borstal | brush | [bɔrstəl] | [bɔtəl] |
| wolken | clouds | [wɔlkən] | [wɔk] |
| jongen | boy | [jɔŋən] | [ɔŋə] |
| kop | head | [kɔp] | [tɑp] |
| klok | clock | [klɔk] | [slɔk] |
Unit 2.4 Focus on speech production
(1) Louise's speech production displays mild to moderate hypernasality and moderate nasal emission. Which feature(s) of her clinical presentation might explain this articulatory deviance?
(2) Which phonological processes are exemplified by the substitutions in (a) to (d) above? Which of these processes occur in ‘kruis’ and ‘kop’ in the table?
(3) Give one example of each of the following phonological processes in the above data.
Progressive assimilation
Regressive assimilation
Metathesis
Syllable deletion
Final consonant deletion
(4) What feature do the following productions have in common?
Word initial /kr/ in ‘tap’ and ‘cross’
Word medial /rst/ in ‘sausages’ and ‘brush’
Final syllable /ən/ in ‘clouds’ and ‘boy’
Word initial /k/ in ‘head’ and ‘clock’
Clinical intervention
Van Lierde et al. (Reference Van Lierde, Van Borsel and Van Cauwenberge2000) recommend the use of ‘tailor-made’ therapy with children who have KMS. They consider this approach to be warranted by the considerable variation that occurs in communication skills both between children with KMS and within individual children with this syndrome. The latter was particularly evident in Louise's case. She displayed a number of intact skills and areas of performance that were within normal limits. For example, Louise had normal cognitive functioning, good receptive language skills and her production of speech sounds was within normal limits for her age. There were also no vocal or laryngeal abnormalities. However, Louise also had considerable difficulties. For example, she had particularly poor expressive language skills in the area of morphosyntax. Although Louise's hearing was within normal limits, she had a history of otitis media that required the placement of transtympanic drains. She also had a submucous cleft palate, slight general hypotonia and poor gross and fine motor skills. Also, her speech sound production was highly variable, and she displayed persisting normal phonological processes, and processes that are uncharacteristic of normal development. Louise also exhibited hypernasality and moderate nasal emission. According to Van Lierde et al., this pattern of communication abilities and impairments cannot be explained by general developmental delay, structural deviations of the speech apparatus, hearing loss or specific language impairment. This pattern, these authors argue, is ‘somewhat reminiscent’ of a phonologic–syntactic disorder.
Unit 2.5 Clinical intervention
(1) Which of the following interventions might play a part in Louise's ‘tailor-made’ therapy?
(2) Is there any basis for the inclusion of a treatment that is based on principles of motor learning of the type used to treat apraxia of speech? Justify your response.
(3) The presence of persisting normal phonological processes, and processes which are uncharacteristic of normal development, suggests the need for some type of phonological treatment as part of Louise's wider communication intervention. Name one such treatment. Also, what evidence is there to support the efficacy of the phonological treatment that you have chosen?
(4) The presence of hypernasality and nasal emission suggests that Louise has velopharyngeal dysfunction (VPD). Blowing and sucking exercises are often used in the treatment of VPD. Are these techniques considered to be effective in the treatment of VPD?
(5) One of the reasons it is so difficult to decide on an appropriate course of intervention in Louise's case is that the diagnosis of her communication disorder is not without complication. In this way, Van Lierde et al. state that her communication problems do not occur (a) as part of a general developmental delay or (b) are a form of specific language impairment. Explain why the diagnoses in (a) and (b) are not appropriate in Louise's case.
Introduction
The following exercise is a case study of a 13-year-old girl (‘CB’) with spastic dysarthria who was studied by Marchant et al. (Reference Marchant, McAuliffe and Huckabee2008). CB has a medical diagnosis of spastic hemiplegic cerebral palsy. She received speech and language therapy for her communication disorder between 6 and 11 years of age. The case study is presented in five sections: primer on developmental dysarthria; client history and communication status; focus on spastic dysarthria; intervention; and speech outcome.
Primer on developmental dysarthria
Hodge (Reference Hodge and Cummings2014) defines developmental dysarthria as ‘a group of speech disorders caused by dysfunction of the immature nervous system that delays speech onset and impairs the strength, speed, accuracy, coordination and endurance of the muscle groups used to speak. Depending on the extent of impairment, one or more of the speech processes of respiration, phonation, resonance, articulation and prosody may be affected’ (26). A child with developmental dysarthria may have reduced breath support for speech (respiration), with the result that only short utterances are possible. The vocal folds may fail to adduct normally during phonation, causing the child to speak with a breathy voice. Closure of the velopharyngeal port may not be adequate during speech production, with the result that the child produces hypernasal speech (resonation). Impairments of the strength, speed and accuracy of articulatory movements may lead to the production of weak and distorted consonants and vowels (articulation). The child with dysarthria may be unable to vary the pitch and loudness of the voice, both of which can compromise intonation (prosody). The resulting speech impairment may be mild in nature, and have few implications for a child's intelligibility. Alternatively, the speech disorder may be so severe that no intelligible speech production is possible. In cases of anarthria, an alternative means of communication may need to be found for the client.
A large range of medical conditions, illnesses and events can give rise to developmental dysarthria. Cerebral palsy is the single largest cause of developmental dysarthria. However, other causes of this motor speech disorder include traumatic brain injury (TBI), infections (e.g. encephalitis), cerebral neoplasms, birth anoxia, brain damage related to metabolic disorders (e.g. phenylketonuria), cranial nerve damage in syndromes (e.g. Möbius syndrome) and neurodegenerative disorders (e.g. Duchenne's muscular dystrophy and Friedreich's ataxia). On account of these diverse aetiologies, it is difficult to obtain figures for the prevalence and incidence of developmental dysarthria. Typically, such figures are reported in relation to particular clinical groups within the dysarthria population. In this way, Morgan et al. (Reference Morgan, Mageandran and Mei2010) reported a low incidence of dysarthria (1.25) in a cohort of 1,895 children following TBI. In children with severe TBI, this incidence figure rose to 205. Mei and Morgan (Reference Mei and Morgan2011) reported the incidence of post-surgical dysarthria in 27 children with posterior fossa tumour to be 30%. Sigurdardottir and Vik (Reference Sigurdardottir and Vik2011) found severe dysarthria in 16% of 152 Icelandic children with congenital cerebral palsy. Developmental dysarthria should be distinguished from acquired dysarthria in childhood. It is only in the former type of dysarthria that the neurological injury has its onset prior to the acquisition of speech skills.
Unit 3.1 Primer on developmental dysarthria
(1) Each of the following diseases, injuries or disorders is a cause of developmental dysarthria. For each one, indicate if it is a traumatic, infectious or genetic cause of dysarthria:
(2) Each of the following statements describes a speech feature of developmental dysarthria in children. Relate each statement to an impairment of one or more of these five speech production subsystems: respiration; phonation; resonation; articulation; prosody.
A child with dysarthria uses fricative strictures in place of stops.
A child with dysarthria places stress on the wrong syllables in words.
A child with dysarthria has a strained–strangled voice.
A child with dysarthria produces heavily nasalised vowels.
A child with dysarthria speaks in short, truncated utterances.
(3) Cerebral palsy is the single largest cause of developmental dysarthria. Name three disorders in children with cerebral palsy other than dysarthria which are assessed and treated by speech-language pathologists.
(4) Respond with true or false to each of the following statements:
(5) Some dysarthrias in children improve over time. Other dysarthrias in children deteriorate over time. Still other dysarthrias remain static over time. For each of the following conditions, indicate whether the associated dysarthria improves, deteriorates or remains static over time:
Client history and communication status
CB is a 13-year-old girl with spastic hemiplegic cerebral palsy. She has spastic dysarthria. CB attends a mainstream school, and is a native speaker of New Zealand English. Speech is her primary means of communication. Her vision and hearing are within normal limits, and her cognitive skills are sufficient for study participation. Although CB had not received speech and language therapy (SLT) for her dysarthria for one year prior to the study, she received continuous SLT between the ages of 6 and 11 years. However, her parents reported limited success from this intervention. There was little information available on the nature of this intervention other than that it took place for only 30 minutes once a week. Parental report suggested that it involved sound production drills. CB is currently receiving instruction in the use of an augmentative communication device. However, she is resistant to using it, and wishes to continue using speech as her primary means of communication.
An oromotor analysis of CB was undertaken. CB displayed severely restricted lingual and labial movement. This included inadequate tongue elevation, tongue lateralisation, tongue retraction, lip pursing and lip seal. The Goldman–Fristoe Test of Articulation (Goldman and Fristoe, Reference Goldman and Fristoe1986) was conducted. This revealed significantly impaired consonant accuracy, particularly in fricative and affricate production. Perceptual analysis by a listener experienced in dysarthria research confirmed a severe spastic dysarthria, characterised by excessively slow rate, strained–strangled phonation, and imprecise consonant and vowel articulation. CB's expressive language was assessed by means of the Language Assessment Remediation and Screening Procedure (LARSP; Crystal, Reference Crystal1997), the conversation analysis profile (Fey, Reference Fey1986) and the profile in semantics (Crystal, Reference Crystal1997). These assessments revealed a severe language delay. The results of the LARSP indicated a severe syntactic delay. CB's attempts at more complex sentences were highly unintelligible and could not be analysed. During conversational exchanges, CB's reduced speech intelligibility led to frequent communicative breakdowns. This resulted in the use of simplified sentences, and the repetition and rephrasing of utterances. Communication partners frequently sought clarification of CB's utterances. This increased the occurrence of her responsive utterances, and reduced the frequency of her attempts to communicate.
Unit 3.2 Client history and communication status
(1) CB was receiving instruction in the use of an augmentative communication device. Give two examples of such a device, one low-tech and the other high-tech. In assessing the suitability of a device for CB, a number of non-communicative factors need to be considered. Name four such factors.
(2) CB was resistant to using an augmentative communication device and wished to use speech as her primary means of communication. How typical is this attitude of AAC users with cerebral palsy?
(3) CB has spastic dysarthria. At what level of the motor pathway for speech is there neurological damage to cause this type of dysarthria?
(4) CB displayed strained–strangled phonation. What is the phonatory basis of this type of voice production?
(5) Explain the sequence of events which leads from CB's reduced speech intelligibility to her assumption of a passive role in communication.
Focus on spastic dysarthria
Spastic dysarthria is more common than other forms of dysarthria in cerebral palsy (Nordberg et al., Reference Nordberg, Miniscalco, Lohmander and Himmelmann2012). Hodge (Reference Hodge and Cummings2014) describes the pathophysiological signs and speech features of spastic dysarthria in children. Pathophysiological signs include slow movements that are limited in range, muscle weakness, excessive muscle tone, muscle rigidity, persisting primitive oral–pharyngeal reflexes and hyperactivity of reflexes that normally persist into adulthood (e.g. jaw stretch, gag). The speech features of this form of dysarthria include vowel and consonant articulation errors, hypernasality, slow speaking rate and short breath groups. During the production of utterances, there are uncontrolled changes in voice quality. The pitch of the voice is lower than expected for the child's age. Speakers with spastic dysarthria exhibit extended word durations. Abnormal resting postures of the lips, tongue and jaw are common.
These speech features of spastic dysarthria have been confirmed in a number of studies. Platt et al. (Reference Platt, Andrews, Young and Quinn1980) examined the speech intelligibility and articulatory impairment of 50 adult males with cerebral palsy. Spastic cerebral palsy and dysarthria were present in 32 of these subjects. The performance of these subjects on two intelligibility measures – accurate recognition of single words and a prose intelligibility rating – was impaired. Indices of articulatory impairment – DDK syllable rates and percentage of correctly articulated phonemes – were also reduced in these subjects. Specific phonemic features in the dysarthric speech of these subjects included anterior lingual place inaccuracy, reduced precision of fricative and affricate manners, and an inability to achieve the extreme positions in the vowel articulatory space. In a later study, Wit et al. (Reference Wit, Maassen, Gabreëls, Thoonen and de Swart1994) compared the performance of two children with TBI-related spastic dysarthria to that of two children with perinatal-onset spastic dysarthria on a number of maximum performance tasks. The three tasks examined maximum sound prolongation, fundamental frequency range and maximum repetition rate. The performance of the children with perinatal-onset spastic dysarthria on all three tasks was poorer than that of their peers with normal speech. The subjects with TBI-related spastic dysarthria performed within normal limits on maximum sound prolongation and fundamental frequency range. However, their maximum repetition rate was extremely slow.
Unit 3.3 Focus on spastic dysarthria
(1) Which of the following are pathophysiological signs of spastic dysarthria?
(2) The speaker with spastic dysarthria exhibits hypernasality. In what two ways is palatal elevation disrupted in spastic dysarthria to result in this speech defect?
(3) Some of Platt et al.'s subjects had perinatal-onset spastic dysarthria. What is the likely cause of these subjects’ dysarthria?
(4) Which of Wit et al.'s findings accounts for the reduced pitch of children with spastic dysarthria?
(5) Respond with true or false to each of the following statements:
Vowel centralisation is a feature of spastic dysarthria.
Reduced DDK rates are related to slow articulatory movements.
Inaccuracy of anterior lingual placement in spastic dysarthria is evident in the articulation of /k, g/.
The articulatory control needed for frication is difficult to achieve in spastic dysarthria.
Intervention
CB received a six-week intervention that consisted of phonetic placement therapy (PPT) and surface electromyography (sEMG)-facilitated biofeedback relaxation therapy. PPT focused on articulation, with five consonant sounds selected for treatment: /t/, /s/, /f/, /ð/ and /ʃ/. The selection of these sounds was based on several factors, including CB's developmental stage, the effect of the sound upon intelligibility, and the results of the Goldman–Fristoe Test of Articulation. All sounds were targeted during each PPT session. However, one sound was the focus of the session and received 30 minutes of treatment. CB was informed of the target sound at the start of the session, and was given an auditory and visual representation of it. A mirror was used to help CB place her articulators. Speech drills and specific feedback were employed. CB was also required to provide feedback about her sound productions. Traditional articulation hierarchies were used, with CB progressing to the next level when an accuracy rate of 80% was achieved for a specific target. For all targeted speech sounds, CB did not progress beyond the sounds-in-words level.
sEMG-facilitated biofeedback relaxation therapy was used with the aim of reducing CB's orofacial spasticity. A portable biofeedback device was used during therapy. In a quiet room at home or at school, CB was seated upright and surface electrodes were applied to the skin. Electrodes were placed in three locations: under the chin, on the left top lip and on the right top lip. These locations corresponded, respectively, to the submental (floor of mouth) muscles, the left superior orbicularis oris muscle, and the right superior orbicularis oris muscle. The submental and orbicularis oris muscles were selected for treatment in order to establish if a reduction in muscle tone could improve the articu-lation of consonants and vowels. The first 20 minutes of treatment focused on the reduction of submental amplitude measures during rest and non-speech postures. The equipment's software provided visual feedback in the form of an animated character. To control this character, CB received the following instructions: ‘I want you to make the man sit on his chair for 10 seconds. Remember, to do this you need to try and stay relaxed.’ The aim was to achieve a consistent response at different thresholds. This process was repeated multiple times for all lingual and labial postures.
Unit 3.4 Intervention
(1) Five consonant sounds were selected for therapy. Aside from the factors described above, explain why these sounds were chosen for treatment. Your answer should address two phonetic features of these sounds.
(2) Traditional articulation hierarchies were employed during PPT. Explain what is involved in these hierarchies.
(3) The aim of sEMG-facilitated biofeedback relaxation therapy was to improve the articulation of consonants and vowels through a reduction in muscle tone during non-speech postures. What assumption underlies this aim? Is this assumption valid?
(4) The orbicularis oris muscles were targeted in sEMG-facilitated biofeedback relaxation therapy. Which of the following are true statements about these muscles?
The function of the orbicularis oris muscles is to retract the lips at the corners.
The orbicularis oris muscles receive innervation from the facial nerve (CN VII).
The orbicularis oris are paired upper (orbicularis oris superior) and lower (orbicularis oris inferior) muscles.
The orbicularis oris muscles receive innervation from the vagus nerve (CN X).
The orbicularis oris is primarily involved in mastication.
(5) CB's intervention was designed in order to adhere to the principles of motor learning. Describe two such principles. Give one example of how each of these principles was implemented in CB's treatment.
Speech outcome
The effects of PPT and sEMG were variable, with positive and negative findings resulting from both therapies. At rest, there were no significant differences in sEMG amplitudes across the treatment phases. However, there was a trend towards reduced submental amplitude post-sEMG treatment. There were also considerably smaller standard deviations for all submental values post-sEMG, indicating greater stability. During non-speech postures, amplitude measures decreased significantly for both tongue protrusion and lip pursing tasks post-sEMG.
These therapies also produced variable perceptual effects. There was a significant increase in single-word intelligibility post-PPT that was maintained following sEMG-facilitated biofeedback. However, on Duffy's perceptual rating scale (Reference Duffy1995), there was no change to any articulatory parameters or to overall intelligibility. Imprecise consonants and overall intelligibility were rated as severely deviant. Vowel distortions were also considered to be markedly deviant. Phonemes were still rated as prolonged following both therapies. The subject's self-perception of her speech impairment remained unchanged following intervention. CB still had moderate concern about her speech disorder.
Acoustic measures of vowel and consonant articulation were also made following intervention. There were significant changes in the second formant (F2) for /æ/ and /u/ following PPT and sEMG, respectively. However, there were no changes in any other formant values. In terms of consonant articulation, there were no significant differences in CV durational measures across any of the targeted syllables. There was only one significant decrease in alternate motion rates, and that was for /kə/ post-sEMG. There was also a significant decrease in inter-syllable gap durations for /pə/ and /tə/ following both PPT and sEMG.
Unit 3.5 Speech outcome
(1) Both treatments in this study failed to bring about improvement in sentence- or paragraph-level intelligibility. Is this finding consistent with the evidence based on the efficacy of interventions available to individuals with developmental dysarthria?
(2) Within an ICF framework for measuring health and disability (World Health Organization, 2001), clinicians must consider the impact of a communication disorder on an individual's quality of life and participation in daily activities. Is there any evidence that CB's functioning or psychological well-being was enhanced by the treatments she received in this study?
(3) Amplitude measures decreased significantly for both tongue protrusion and lip pursing tasks post-sEMG. However, this did not lead to any corresponding improvement in CB's overall intelligibility. How might these findings be explained?
(4) Alternate motion rates did not decrease significantly following PPT. How might these rates be assessed? Why is this finding not entirely unexpected?
Introduction
The following exercise is a case study of a boy (‘Zachary’) who was studied by Powell (Reference Powell1996). Zachary's speech delay was first noted at 30 months of age. Subsequent assessment revealed a pattern of speech behaviours which was consistent with a diagnosis of developmental apraxia of speech and oral apraxia. The case study is presented in five sections: primer on developmental apraxia of speech; client history; neurological, adaptive and cognitive evaluation; speech, language, hearing and oral mechanism evaluation; and intervention and outcome.
Primer on developmental apraxia of speech
Developmental apraxia of speech (DAS), which is also known as childhood apraxia of speech (CAS) and developmental verbal dyspraxia (DVD), is a complex motor speech disorder which has its onset in early childhood. A position statement published by the American Speech-Language-Hearing Association (2007) defines CAS as:
a neurological childhood (pediatric) speech sound disorder in which the precision and consistency of movements underlying speech are impaired in the absence of neuromuscular deficits (e.g., abnormal reflexes, abnormal tone). CAS may occur as a result of known neurological impairment, in association with complex neurobehavioral disorders of known or unknown origin, or as an idiopathic neurogenic speech sound disorder. The core impairment in planning and/or programming spatiotemporal parameters of movement sequences results in errors in speech sound production and prosody.
Although DAS has been extensively investigated, little is still known about the epidemiology of the disorder. Shriberg et al. (Reference Shriberg, Aram and Kwiatkowski1997) stated that DAS occurs in 1–2 children per 1,000. The prevalence of DAS is considerably higher in certain metabolic and genetic disorders. Shriberg et al. (Reference Shriberg, Potter and Strand2011) reported the prevalence of CAS in the metabolic disorder galactosaemia to be 18 per 100. This is 180 times the estimated risk for idiopathic CAS. DAS is more commonly found in boys than in girls. Hall et al. (Reference Hall, Jordan and Robin1993) found an average male:female ratio of approximately 3:1 in a review of 24 group studies and 11 single-subject studies. DAS has been reported in several chromosomal and genetic syndromes including cri du chat syndrome, Down's syndrome and 7q11.23 duplication syndrome (Kumin, Reference Kumin2006; Marignier et al., Reference Marignier, Lesca, Marguin, Bussy, Sanlaville and des Portes2012; Velleman and Mervis, Reference Velleman and Mervis2011). The presence of DAS in these syndromes and many others confirms the neurogenetic origins of the disorder.
The speech features of DAS are well characterised. Children with DAS produce a range of consonant errors. These errors include the deletion of initial and final consonants, cluster reductions, voicing errors and substitutions (Lewis et al., Reference Lewis, Freebairn, Hansen, Iyengar and Taylor2004; Jacks et al., Reference Jacks, Marquardt and Davis2006). The vowel system in DAS is often severely disordered. Lewis et al. (Reference Lewis, Freebairn, Hansen, Iyengar and Taylor2004) found that 100 per cent of the children with CAS in their study produced vowel errors. Davis et al. (Reference Davis, Jacks and Marquardt2005) charted the vowel inventory and accuracy patterns of three children with suspected DAS over a three-year period. Vowel accuracy was impaired in all children, although accuracy did show a moderate increase from the first data recording to the final data recording. Errors consisted mainly of vowel substitutions and de-rhoticisation. No consistent pattern of errors was found in the substitutions. Prosodic disturbances, including anomalies of rate, intonation and stress, have been reported in children with DAS (Odell and Shriberg, Reference Odell and Shriberg2001). Children with DAS also display reduced diadochokinetic rates and poor sequencing of sounds and syllables (Moriarty and Gillon, Reference Moriarty and Gillon2006). There is often an accompanying oral apraxia (Alcock et al., Reference Alcock, Passingham, Watkins and Vargha-Khadem2000). Language problems are also present, with receptive language skills superior to expressive skills (Aziz et al., Reference Aziz, Shohdi, Osman and Habib2010; Grigos and Kolenda, Reference Grigos and Kolenda2010).
Client history
A developmental and medical history was taken, using Zachary's mother as an informant. Zachary was a full-term baby who had a normal delivery. He developed influenza when he was 8 months old. This caused diarrhoea and a high fever. Zachary became dehydrated during his illness as he would not consume liquids. He developed middle ear infections and chickenpox when he was 3 years old. At 30 months of age, a speech delay was noted. As a result, a communication evaluation was conducted. The speech-language pathologist reported that Zachary's behaviours were consistent with DAS and oral dyspraxia. Zachary was enrolled in a course of speech and language therapy. However, his progress was reportedly slow. At 38 months of age, Zachary underwent a comprehensive multidisciplinary evaluation.
Unit 4.2 Client history
(1) Zachary developed influenza at 8 months and chickenpox at 3 years of age. What implications might these infections have had for Zachary's development?
(3) A speech delay was noted when Zachary was 30 months old. Which of the following speech and language skills are acquired by normally developing children by 30 months of age?
(4) The speech-language pathologist reported that Zachary's behaviours were consistent with DAS and oral dyspraxia. Describe three behaviours which are indicative of oral dyspraxia.
(5) At 38 months of age, Zachary underwent a comprehensive multidisciplinary evaluation. Aside from speech and language, describe three areas which should be examined by such an evaluation.
Neurological, adaptive and cognitive evaluation
As part of his neurological evaluation, Zachary had a CT scan and an EEG. The scan results were normal, while the EEG was ‘mildly diffusely slow for age’. The paediatric neurologist concluded that Zachary exhibited ‘developmental delay, language greater than motor, of unknown etiology’. At 47 months of age, Zachary underwent a second neurological examination. His sensory examination was normal. Zachary's motor skills were characterised as ‘generally normal, although he [was] minimally hypotonic and [had] a generalized decrease in coordination with running’. The neurologist concluded that Zachary was ‘afflicted with an organic static, probably prenatal encephalopathy resulting in a developmental expressive aphasia, tongue apraxia, and possibly a mild developmental delay’.
On the Vineland Adaptive Behavior Scales (Sparrow et al., Reference Sparrow, Balla and Cicchetti1984), Zachary performed in the low range relative to same-age peers on ‘daily activities required for personal and social sufficiency’. His intellectual functioning was in the low average to borderline range on standardised testing. At 63 months of age, Zachary's non-verbal intellectual functioning was evaluated. Zachary was required to place blocks into a wooden frame to complete visual problems. These problems increased in complexity from simple concretistic matching to conceptual items that required reasoning and problem-solving skills. Zachary displayed some incoordination on this task, especially when smaller or irregularly shaped blocks were used. When Zachary had to combine two or more smaller blocks into a larger one that could be fitted into the frame, his responses were frequently mirror images of the stimuli.
Unit 4.3 Neurological, adaptive and cognitive evaluation
(1) Is there any evidence that Zachary may have a generalised dyspraxia in addition to his apraxia of speech?
(2) Zachary's motor skills were reported to be minimally hypotonic. What is hypotonia? In what motor speech disorder in children can hypotonia be a feature?
(3) Zachary's adaptive functioning was assessed by means of the Vineland Adaptive Behavior Scales. Name two neurodevelopmental disorders which this assessment may be used to diagnose. Is there any evidence that Zachary has these disorders?
(4) What two sets of skills are required in order to place blocks into a wooden frame so that they match a visual pattern?
(5) Zachary struggled to bring two or more smaller blocks together in order to fit them into the frame. This task requires skills beyond those that you identified in your response to question (4). What are these skills?
Speech, language, hearing and oral mechanism evaluation
Zachary's language skills were assessed using standardised tests on four occasions between 4;0 years and 6;1 years. On all occasions, his comprehension was in the extremely low to low average range. At 5;1 years, Zachary's score on the Peabody Picture Vocabulary Test (PPVT; Dunn and Dunn, Reference Dunn and Dunn1981) placed him in the 8th percentile. One year later at 6;1 years, Zachary's score on the PPVT placed him in the 14th percentile. Zachary appeared to follow most verbal commands that did not require a verbal response. His comprehension was facilitated by the use of gestures alongside verbal commands. In relation to expressive language, Zachary had fewer than 10 single words at 4 years of age. He imitated single words inconsistently, and produced car-like noises as he played with a toy car. Zachary had such limited expressive speech skills that an articulation test could not be performed. At 4 years of age, he was only able to produce six consonants ([m], [p], [b], [d], [k], [h]) and four vowels ([i], [o], [ɑ], [u]). Syllable structure was adversely affected, with Zachary producing words with a CV structure or reduplicated CVCV structure. His speech displayed frequent homonymous forms.
An examination of the oral mechanism revealed that Zachary's speech structures were symmetric and functioning. There were no apparent organic abnormalities of the oral structures that might interfere with speech production. However, oral motor functioning was difficult for Zachary. He was able to perform most simple voluntary movements. Exceptions were puffing his cheeks, lateralising and elevating his tongue inside his mouth, and pushing the examiner's finger when it was placed against his cheek. It was unclear to what extent Zachary's comprehension problems compromised his performance on these tasks. The production of alternating nonsense syllables was also difficult for him. Zachary had one episode of otitis media at 3 years of age. He passed pure-tone hearing screening.
Unit 4.4 Speech, language, hearing and oral mechanism evaluation
(1) Zachary's scores on the PPVT placed him in the 8th percentile at 5;1 years and the 14th percentile at 6;1 years. Explain what these percentiles mean.
(2) By 4 years of age, Zachary had fewer than 10 single words. How much of a developmental delay does this represent?
(3) Zachary's speech displayed frequent homonymous forms. What does this mean?
(4) Name three behaviours which suggest the presence of an oral dyspraxia.
(5) What type of communication intervention would be appropriate in Zachary's case?
Intervention and outcome
For over a year, Zachary received individual speech and language therapy at two different institutions. The content of this therapy was consistent with some of the published literature on DAS. However, it resulted in only modest gains in Zachary's communicative competence at which point Powell (Reference Powell1996) undertook an alternative intervention. This new intervention emphasised the early stimulation of unknown aspects of phonology with a view to encouraging broadening of the phonetic inventory and distribution of sounds. It was delivered in four, one-hour treatment sessions per week (Zachary's previous treatment involved two, 30-minute sessions per week). Therapy sessions were modular in nature. One such module, which is taken from Powell (Reference Powell1996: 325), is shown below.
Warm-up activity
Stimulate imitation of sounds and/or syllables using pictured stimuli. Note that activity should initially be play-like and relatively indirect. Successful imitations may be acknowledged. To maintain a high level of motivation, the use of phonetic placement cues is avoided.
| Sample targets: | Stimulus photo: |
| [pʌpʌpʌ] | Popcorn being popped |
| [gʌgʌgʌ] | Drinking water |
| [f:::] | Balloon leaking air |
| [ʒ:::] | Sewing machine |
| [ʧʧʧ] | Train |
| [ɝ:::] | Growling dog or bear |
| [m:::] | Bowl of ice cream |
Goal 1
Elicitation of a new sound in CV or VC syllables (imitation) using visual, tactile or auditory cues as needed. Example: Imitation of [iz], [ɑz], [uz], [æz] using a drill-play paradigm.
Goal 2
Stabilisation of inconsistently used sounds in words. Vary the position and phonetic context. Stimulus items may also be used to reinforce vocabulary development. Example: Elicited production of [k] in words: ‘key’, ‘keep’, ‘eek’, ‘peek’, etc. Fade cues and increase speed to encourage automaticity.
Goal 3
Generalisation of ‘known’ sounds in ‘known’ positions at a more conversational level. Tasks may be relatively flexible provided frequent opportunities are provided for the production of targeted sounds. Example: ‘Shopping’ activity where items on sale are chosen on the basis of their sound shapes: ‘pie’, ‘map’, ‘tea’, ‘baby’, etc. Design of the activity may also address language goals.
Goal 4
Maintenance of previously taught sounds embedded in language stimulation activity. The activity may be less structured than the preceding in terms of phonological stimuli. The focus of this goal may be on language skill with planned opportunities to monitor production of previously generalised targets.
Cool-down activity
Repeat the warm-up activity or some similar variant
At the outset of this intervention, Zachary had only 11 consonants in his phonetic inventory. After three months of this new treatment, his phonetic inventory had increased to 17 consonants. Not only had the size of his phonetic inventory increased, but its complexity had also increased. Zachary's consonant inventory had initially included stops, nasals and glides. By 5;1 years, his inventory had increased in complexity to include fricatives and affricates. By 5;4 years, its complexity had increased further by the addition of the liquid /l/. The complexity and range of syllabic structure also increased following this new intervention. Before intervention, Zachary only produced CV syllables and reduplicated CVCV strings. However, by 5;4 years he was also using VC, CVC, CCVCV and CVCC syllables.
Unit 4.5 Intervention and outcome
(1) In what respect does the new intervention that Zachary received differ from other therapies for sound production disorders in children?
(2) To what extent do you think the intensity of Zachary's earlier treatment contributed to its limited success?
(3) The type and frequency of feedback are acknowledged by clinicians to play an important role in interventions for DAS. What kind of feedback is used in this new intervention? What other forms of feedback can facilitate speech production in children with DAS?
(4) Zachary's language skills, particularly his expressive language skills, are severely impaired. How does this new intervention embed language stimulation alongside its speech goals?
(5) Respond with true or false to each of the following statements:
This new intervention uses multi-sensory cues to facilitate production of speech targets.
This new intervention provides Zachary with multiple opportunities for the production of target sounds.
This new intervention aims to enhance the range and strength of articulatory movements.
This new intervention prioritises speech goals over language goals.
Introduction
The following exercise is a case study of a man (‘GS’) who was studied by Morrish (Reference Morrish1988). GS underwent a total glossectomy for the treatment of a carcinoma at the base of his tongue. His post-operative speech production was examined in detail. The case study is presented in five sections: primer on oral cancer and glossectomy; speech and swallowing following glossectomy; client history; focus on articulation and intelligibility; and focus on instrumental and acoustic analyses.
Primer on oral cancer and glossectomy
Glossectomy is the surgical removal of whole or part of the tongue (total and partial glossectomy, respectively). The procedure is typically performed to treat tongue cancer, although in a smaller number of cases it may also be used to correct congenital macroglossia (Choi et al., Reference Choi, Kim, Park and Kwon2013). The tongue is the most common intraoral site for oral cancer worldwide (Moore et al., Reference Moore, Johnson, Pierce and Wilson2000). In 2013, there were 13,590 estimated new cases of oral tongue cancer in the United States and 2,070 estimated deaths. The most common type of tongue cancer is a squamous cell carcinoma. Less commonly found carcinomas of the tongue include adenoid cystic carcinoma and mucoepidermoid carcinoma (Leong et al., Reference Leong, Pinder, Sasae and Mortimore2007; Luna-Ortiz et al., Reference Luna-Ortiz, Carmona-Luna, Cano-Valdez, Mosqueda-Taylor, Herrera-Gómez and Villavicencio-Valencia2009). As well as tobacco smoking and alcohol consumption, other risk factors for tongue cancer include certain viruses (e.g. Epstein–Barr virus and human papilloma virus (HPV) 16 and 18), cultural practices – prevalent in parts of India – such as reverse smoking (the burning end of cigars is within the mouth) and dipping (placing a mixture of Khaini tobacco and slaked lime in the lower gingival groove), and sexual behaviours including oral sex (although this is likely to be related to HPV infection) (Heck et al., Reference Heck, Berthiller, Vaccarella, Winn, Smith, Shan'gina, Schwartz, Purdue, Pilarska, Eluf-Neto, Menezes, McClean, Matos, Koifman, Kelsey, Herrero, Hayes, Franceschi, Wünsch-Filho, Fernández, Daudt, Curado, Chen, Castellsaqué, Ferro, Brennan, Boffetta and Hashibe2010; Stich et al., Reference Stich, Parida and Brunnemann1992; Zheng et al., Reference Zheng, Xia, Zheng, Takahashi, Masuda and Takano2010).
On account of the serious implications of glossectomy for speech and swallowing, this operation is performed as a last resort when other treatment options (e.g. radiotherapy) have failed to treat a tumour. The defect that is created by glossectomy is reconstructed with a local closure, a local flap or a free flap. A local closure is used when the defect is small. If the defect is relatively large, then it is closed with the use of a flap. To form local flaps, tissue can be raised from the neck (platysma muscle), chest (pectoralis muscle) and forehead (frontalis muscle). Free flaps can be formed using tissue from the radial forearm, inside of the thigh (gracilis flap) and the abdomen (rectus abdominis muscle). The oral surgeon must consider a range of factors in the choice of flap, including the size of defect to be reconstructed, the aesthetic appearance of the tongue and the functional outcome for the patient in terms of speech and swallowing. The radial forearm free flap has emerged as the standard for partial glossectomy as it provides the desired bulk and contour for reconstruction. For total glossectomy, the more bulky anterolateral thigh flap and rectus abdominis can achieve greater propulsion of food into the pharynx during swallowing, the greater volume of these flaps compensating for the lack of motor function (Allan et al., Reference Allan, Van Haren, Wang, Thaller, Taub, Patel, Buchman and Cohen2015).
Advanced carcinoma of the tongue can necessitate additional surgical procedures including laryngectomy, mandibulectomy and pharyngectomy. These procedures also have serious implications for swallowing and the production of speech and voice. Van Lierop et al. (Reference Van Borsel and Vandermeulen2008) studied eight patients who underwent total glossectomy. Three patients also required a total laryngectomy for a tumour involving the pre-epiglottic space or larynx. Five patients had a marginal mandibulectomy, one underwent segmental mandibulectomy and one required partial pharyngectomy. For patients with advanced squamous cell carcinoma of the tongue, Sinclair et al. (Reference Sinclair, Carroll, Desmond and Rosenthal2011) reported reduced disease recurrence at 12 months postoperatively for patients who underwent total laryngoglossectomy (40%) compared to total glossectomy (61%). Disease-free survival at 12 months was also higher in patients with total laryngoglossectomy (50%) than in patients with total glossectomy (40%). However, intelligible speech was less often achieved by patients with total laryngoglossectomy (10%) than by patients with total glossectomy (30%).
Unit 5.1 Primer on oral cancer and glossectomy
(1) Respond with true or false to each of the following statements about glossectomy:
Glossectomy is used before radiotherapy and chemotherapy to treat tongue cancer.
Glossectomy may be used to treat macroglossia in children with Down's syndrome.
Glossectomy and laryngectomy are often used in combination to treat early-stage tongue cancer.
Total glossectomy is often accompanied by oesophagectomy.
Glossectomy may be used to treat macroglossia in children with Beckwith–Wiedemann syndrome.
(2) Quality of life is an important concept in the management of clients who undergo glossectomy. Which two factors are consistently reported by these clients to be most significant to their quality of life?
(4) A range of different flaps may be used to correct the defect that is caused by glossectomy. Give one advantage and one disadvantage of the use of a bulky flap following total glossectomy.
Speech and swallowing following glossectomy
Clients who undergo glossectomy are under the care of a multidisciplinary team. Included in this team are oral surgeons, radiation and medical oncologists, otolaryngologists, prosthodontists and speech-language pathologists. It is the role of the speech-language pathologist to assess and treat swallowing and speech problems in clients with glossectomy. SLP management of the client should begin at the point of diagnosis and continue until the best possible speech and swallowing outcomes have been achieved. However, the duration and intensity of intervention can vary markedly between healthcare systems and treatment centres.
Even the very best surgical results following glossectomy will involve some degree of compromise of swallowing and speech function. Dziegielewski et al. (Reference Dziegielewski, Ho, Rieger, Singh, Langille, Harris and Seikaly2013) examined functional outcome data in 12 patients who underwent total glossectomy with laryngeal perseveration. These investigators also conducted a systematic review of the literature. Fifty per cent of the patients in this study, and 24% with systematic review, were still using gastrostomy tubes at one year post-surgery. In patients who could swallow, swallowing transit times more than doubled, but aspiration did not occur. On average, spoken sentence intelligibility was 66%. The best swallowing and speech functional outcomes occurred in patients who attended over 80% of swallowing and speech rehabilitation sessions. Vega et al. (Reference Vega, León, Cervelli, Pons, López, Fernández, Quer and Masià2011) examined 39 patients who underwent glossectomy (24 total glossectomy, 15 subtotal glossectomy). Oral feeding was resumed in 33 (85%) of these patients. Speech was judged to be good or acceptable in 27 (87%) patients. Improved speech and swallowing outcomes following glossectomy are associated with flap reconstructions which have sufficient bulk and vertical height to allow for contact with the palate (Rigby and Hayden, Reference Rigby and Hayden2014).
Speakers who undergo glossectomy can achieve relatively good intelligibility through the use of unusual labial, mandibular and pharyngeal speech compensations (Kazi et al., Reference Kazi, Prasad, Kanagalingam, Georgalas, Venkitaraman, Nutting, Clarke, Rhys-Evans and Harrington2007). A number of these compensations occurred in the speech of seven German patients who were studied by Barry and Timmermann (Reference Barry and Timmermann1985). These patients were aged 32 to 62 years and each underwent a partial glossectomy. Plosive sounds involving the tongue were substituted by fricatives, glottal stops or bilabial stops. Kaipa et al. (Reference Kaipa, Robb, O'Beirne and Allison2012) examined speech produced by a 31-year-old female in the three-month period following glossectomy. Acoustic analysis revealed improvements in the vowel space area during this time. However, there was deterioration in the perception of this speaker's consonants, with anterior sounds being perceived more correctly than medial and posterior sounds. Bressmann et al. (Reference Bressmann, Jacobs, Quintero and Irish2009) assessed speech acceptability in 22 patients with partial glossectomies. These investigators found that the amount of tongue tissue resected predicted 41 per cent of the variance in post-surgical speech acceptability. Moreover, a defect size of more than 20.4 per cent of tongue tissue was found to be the critical cut-off point for poorer speech acceptability.
Unit 5.2 Speech and swallowing following glossectomy
(1) Which of the medical and health professionals described above manages the following aspects of care of clients with tongue cancer?
This professional oversees the surgical removal of the larynx.
This professional oversees the assessment and treatment of dysphagia.
This professional oversees the type of radiotherapy to be administered.
This professional oversees the use of prosthetic devices by clients.
This professional oversees the surgical removal of the tongue and defect reconstruction.
(2) Many patients who have a glossectomy need to use a gastrostomy tube for a period of time after surgery. Describe what this tube is, and explain why it is necessary in patients who have a glossectomy.
(3) The German speakers with partial glossectomy who were studied by Barry and Timmermann (Reference Barry and Timmermann1985) produced the following sound substitutions for the voiceless alveolar plosive: /t/ → [ʔ] and /t/ → [p]. Explain the basis of these substitutions.
(4) Barry and Timmermann's subjects make a number of other substitutions for plosive sounds that involve the tongue. These substitutions include /d/ → [s], /k/ → [x] and /g/ → [ɣ]. Explain the basis of these substitutions.
(5) Bressmann et al. (Reference Bressmann, Jacobs, Quintero and Irish2009) found that the amount of tongue tissue resected was significant in post-surgical speech acceptability. Which other factor plays an important role in speech acceptability following glossectomy?
Client history
Subject ‘GS’ is a 69-year-old white man who underwent total glossectomy eight years earlier. This procedure was necessitated by a diagnosis of invasive squamous cell carcinoma at the base of the tongue. The epiglottis was preserved and there was no mandibular involvement. Dentition also remained unaffected, although GS's lower teeth had been replaced by dentures. The defect created by glossectomy was reconstructed using a forehead flap. Frontalis muscle was introduced through the cheek. There was no free edge to this flap – it was entirely set in. Following glossectomy, GS received speech therapy for two years. Notwithstanding the radical nature of GS's surgery, a speech and language therapist judged his speech to be good.
Unit 5.3 Client history
(1) Are the age, ethnicity and sex of GS typical of clients who are diagnosed with oral squamous cell carcinoma?
(2) Respond with true or false to each of the following statements about GS's tumour:
GS has the least common type of tongue cancer.
GS has been diagnosed at an early stage in tumour development.
GS has the most common type of tongue cancer.
GS has a type of tongue cancer which is mostly found in young adults.
GS has a tumour at the base of the tongue when most tumours affect the oral tongue.
(3) Is there a high or a low probability that GS resumed oral feeding after total glossectomy? What factors are influential in your decision?
(4) A forehead flap was used to reconstruct the defect caused by glossectomy. This is a type of local flap. What does this mean?
Focus on articulation and intelligibility
To determine GS's intelligibility, 16 phonetically naive subjects listened through headphones to an audio-recording of 10 randomly devised sentences. All sentences were played once in full and then singly, with no repetition permitted. Subjects also listened to an extract of conversation with GS. Repetition of the recording was permitted, although subjects were advised not to spend more than five or six minutes on this task. Subjects then orthographically transcribed what they heard. The transcription had to be 100% correct in order for a subject to be said to have understood what GS said. Intelligibility scores across the sentences and conversational passage were high at 65% and 58%, respectively. There was considerable variability between listeners, however, with intelligibility scores on the conversational passage ranging from 15% to 71%. A second intelligibility test was conducted. Because it had been observed that GS used a bilabial place of articulation for all plosive sounds, the focus of this test was on his production of initial plosive consonants. Subjects listened to audio-recordings of GS as he produced the following CVC monosyllables – kit, beat, tick, deep, dip, bill, peat, keep, pit, gill and teak. Although the bilabial plosives /p, b/ were identified at a rate better than chance, the alveolar plosives /t, d/ and the velar plosives /k, g/ did not even reach chance, and were overwhelmingly identified as bilabial plosives.
In the absence of a tongue, GS used a complete bilabial closure to articulate all plosive sounds. To establish if he varied this closure to signal different plosives, a close-up video analysis of GS during speech production was performed. The degree of bilabial protrusion, jaw retraction/protrusion and jaw elevation/lowering was measured in millimetres as deviations from a rest position. The same CVC monosyllables as above were used during this examination. Although there was little difference between alveolar and velar plosives, there was a consistent and statistically significant difference between bilabial and alveolar plosives in terms of jaw lowering. A lower posture was adopted for bilabial plosives. These same plosives also showed a statistically significant difference in terms of jaw protrusion, with bilabial plosives more protruded than alveolar plosives. There was a slight statistically significant difference between bilabial and alveolar plosives in terms of bilabial protrusion. GS used a more protruded posture for /t, d/ than for /p, b/.
Unit 5.4 Focus on articulation and intelligibility
(1) Intelligibility scores were based solely on audio-recordings of GS's speech. Ratings of intelligibility normally increase when speakers can be seen as well as heard. Is that likely to happen in this case?
(2) Video analysis revealed that GS used bilabial protrusion, jaw protrusion and jaw lowering to signal differences between bilabial and alveolar plosives. How would you characterise these articulatory adjustments on GS's part?
(3) The substitutions used by Barry and Timmermann's German speakers as they attempted to produce alveolar and velar plosives were examined at page 34. Is GS's production of these same plosive sounds similar to, or different from, the productions of these speakers?
(4) How might the substitutions produced by GS and Barry and Timmermann's subjects be explained in terms of the surgical procedures that these subjects underwent?
Focus on instrumental and acoustic analyses
Instrumental analyses using electromyography (EMG) and a strain gauge apparatus were used to confirm the results of the video analysis of GS's speech. During EMG, surface electrodes were placed on either side of the philtrum from where they measured the activity of the orbicularis oris muscle. GS read CV monosyllables in which the vowels were neural for lip position. There was a high statistical difference in the activity of the orbicularis oris muscle during the articulation of /t, d/ and /p, b/, with greater activity observed during alveolar plosives. Through use of the strain gauge apparatus it was confirmed that jaw lowering was greater for /p, b/ than for /t, d/. These instrumental techniques confirmed that GS was using certain postures consistently during the production of bilabial and alveolar plosives, and that these postures were detectable during video and instrumental analyses, even if they were not always perceived by listeners.
Videofluoroscopy was used to assess GS's articulation of high and low vowels. For high vowels, the pharynx widens and the grafted flap rises slightly. There is slight protrusion of the jaw which retains a close position. The soft palate closes firmly and is raised to a position well above Passavant's ridge. For low vowels, pharyngeal narrowing is achieved by a strong retraction of the anterior wall and the epiglottis. The flap rises and bunches and is carried back with the anterior wall of the pharynx to approximate the posterior wall. The jaw moves downwards and backwards, with downward movement exaggerated in comparison with normal speakers. GS's production of vowels and consonants also underwent acoustic analysis. GS repeated randomly ordered CVC words which were analysed on a sound spectrograph. Formant frequencies were measured and compared with those from a normal speaker. GS was unable to differentiate between high and low vowels acoustically. Spectrograms were also made of all the CVC words used in the intelligibility tests. Several acoustic characteristics were examined. However, none were judged to correspond to GS's articulatory differences between bilabial and alveolar plosives.
Unit 5.5 Focus on instrumental and acoustic analyses
(1) During electromyography, GS read CV monosyllables in which the vowels were neutral for lip position. Why is a neutral lip position important in the context of this examination?
(2) GS's production of high and low vowels was assessed through the use of videofluoroscopy. Which of the following statements is true of this technique?
Videofluoroscopy can be used to assess velopharyngeal function.
Videofluoroscopy makes use of a palatal plate that contains electrodes.
A radio-opaque bolus must be swallowed during videofluoroscopy.
Videofluoroscopy measures nasal airflow during speech production.
Videofluoroscopy may be used in the assessment of dysphagia.
(3) A structure which is not normally active during articulation was used by GS during the production of vowels. What is that structure? What function does it serve during vowel production?
(4) GS was unable to use any acoustic feature to distinguish alveolar from bilabial plosives. Given that this is the case, what earlier finding is unsurprising?
Introduction
The following exercise is a case study of a 39-year-old man (‘AB’) who was studied by Grunwell and Huskins (Reference Grunwell and Huskins1979). AB suffered a cerebrovascular accident in December 1972 which resulted in dysarthria and other neurological sequelae. The case study is presented in five sections: primer on acquired dysarthria; client history and clinical presentation; speech evaluation; focus on mixed dysarthria; and assessment issues.
Primer on acquired dysarthria
‘Acquired dysarthria’ is a collective term for a group of motor speech disorders which are caused by damage to the central and/or peripheral nervous systems. Typically, these disorders have their onset in adulthood, although acquired dysarthria may also arise in childhood. The perceptual anomalies that occur in acquired dysarthria reflect impairments in one or more speech production subsystems, namely, articulation, resonation, phonation, respiration and prosody. Acquired dysarthria may minimally disrupt speech intelligibility. Alternatively, the disorder may compromise speech production to such an extent that the client is severely unintelligible and must use an alternative means of communication.
The incidence and prevalence of acquired dysarthria in the general population is largely unknown. To understand the epidemiology of this motor speech disorder, it is necessary to examine its incidence and prevalence in relation to specific clinical populations. Adults who sustain a cerebrovascular accident or stroke are most at risk of acquired dysarthria. Using the Registry of the Canadian Stroke Network's database, Flowers et al. (Reference Flowers, Silver, Fang, Rochon and Martino2013) estimated the incidence of dysarthria in a sample of 221 patients with acute ischaemic stroke to be 42%. Another significant cause of acquired dysarthria in children and adults is traumatic brain injury (TBI). Safaz et al. (Reference Safaz, Alaca, Yasar, Tok and Yilmaz2008) reported the presence of dysarthria in 30.2% of 116 persons with TBI who were followed at a single centre in the five-year period between 2000 and 2006. Aside from stroke and TBI, other neurological disorders associated with acquired dysarthria include multiple sclerosis, Parkinson's disease, and motor neurone disease (also known as amyotrophic lateral sclerosis). The incidence and prevalence of acquired dysarthria in several of these disorders has also been investigated. Danesh-Sani et al. (Reference Danesh-Sani, Rahimdoost, Soltani, Ghiyasi, Haghdoost and Sabzali-Zanjankhah2013) reported the presence of dysarthria in 42.1% of 500 patients aged 11 to 69 years with multiple sclerosis. Perez-Lloret et al. (Reference Perez-Lloret, Nègre-Pagès, Ojero-Senard, Damier, Destée, Tison, Merello and Rascol2012) estimated the prevalence of dysarthria in 419 patients with Parkinson's disease to be 51%.
All aspects of speech production may be compromised in dysarthria. In terms of articu-lation, a speaker with dysarthria may produce weak and distorted consonant and vowel sounds. Problems with resonation may arise on account of mistiming of the closure of the velopharyngeal port. A breathy voice may reflect inadequate glottal valving of the pulmonary airstream during phonation. A speaker with dysarthria may produce short, truncated utterances on account of impaired respiration. In terms of prosody, a speaker with dysarthria may place stress on the wrong syllables within words, and the wrong words within sentences. Each of these speech production difficulties are related to neuromuscular deficits which affect the range, speed, force and timing of movements of the articulators and other organs of speech.
Dysarthria may occur in isolation in clients. However, it is often the case that it is found alongside dysphagia and other neurogenic communication disorders, principally aphasia and apraxia of speech. In their study of 221 clients with acute ischaemic stroke, Flowers et al. (Reference Flowers, Silver, Fang, Rochon and Martino2013) found that the highest co-occurrence of any two impairments was 28% for the presence of dysphagia and dysarthria. Dysarthria in combination with dysphagia and aphasia was present in 10% of these clients. A combination of dysarthria, sialorrhoea (drooling) and dysphagia was present in 136 (33%) of 419 patients with Parkinson's disease examined by Perez-Lloret et al. (Reference Perez-Lloret, Nègre-Pagès, Ojero-Senard, Damier, Destée, Tison, Merello and Rascol2012). These additional disorders are significant in that they can make a differential diagnosis of dysarthria difficult (particularly if apraxia of speech is present), and they provide additional obstacles to the successful rehabilitation of clients.
Unit 6.1 Primer on acquired dysarthria
(1) Which of the following conditions is a cause of acquired dysarthria?
(2) The following statements describe cases of acquired dysarthria in children and adults. For each statement, indicate if the dysarthria has a traumatic, infectious, neoplastic and/or iatrogenic aetiology.
A 10-year-old child develops speech problems following excision of a posterior fossa tumour.
A woman experiences speech problems following a prolonged illness with herpes simplex encephalitis.
A 15-year-old boy has reduced intelligibility following a head injury.
A man who sustains recurrent laryngeal nerve damage during thyroidectomy has speech production difficulties following surgery.
A 12-year-old boy has unintelligible speech following cranial irradiation for a medulloblastoma.
(3) Dysarthria is a feature of neurodegenerative disorders such as multiple sclerosis, Parkinson's disease and motor neurone disease. Which of the following types of dysarthria are associated with these disorders?
(4) The following statements describe impairments in dysarthria. Relate each statement to one of the following speech production subsystems: articulation; resonation; prosody; respiration; phonation.
Client history and clinical presentation
AB is 39 years old. In December 1972, he had a cerebrovascular accident (an intracerebral haematoma). He has a history of hypertension. Following his CVA, he presented with right-sided weakness. He displayed right upper and lower facial weakness, some dysphasia, dysphonia and dysarthria of brainstem origin. AB's wife reported that his speech had been somewhat nasal and difficult to understand prior to his CVA. In January 1974, AB's speech musculature was examined. It was found to be bilaterally affected, with greater impairment on the right. There was spastic weakness of the lips and tongue. The palate was atrophied and foreshortened. The palatal impairment was attributed to flaccid weakness. All articulatory movements, but especially those involving the palate, were impaired. AB was given a speech diagnosis of mixed dysarthria owing to the presence of both bulbar and suprabulbar signs.
Unit 6.2 Client history and clinical presentation
(1) AB suffered a cerebrovascular accident. Describe the type of CVA he experienced.
(2) AB displayed both spastic and flaccid weakness. What are the lesion sites which give rise to this type of weakness?
(3) Which of the following are clinical signs of lower motor neurone damage?
Speech evaluation
AB's speech production underwent a comprehensive assessment. The slow movement of the articulators contributed to a general slow speaking rate. There was articulatory imprecision in the production of consonants and vowels which was related to slowness of movement and weakness of articulation. AB frequently failed to reach target positions. This resulted in errors of vowel quality and the use of a fricative stricture in place of a stop. In terms of phonation, AB displayed a breathy voice. The loudness of the voice did not vary. There was also a lack of pitch variation, and the pitch of the voice was abnormally high. AB exhibited audible nasal emission, which was evident on a spectrogram as a high frequency noise trace. Excessive nasal resonance was evident during voiced segments.
The interaction of these deviant features reduced the intelligibility of AB's speech. AB's uneconomical use of air meant that he was only able to speak in short phrases. His slow rate of articulatory movements also contributed to the restricted length of his utterances. The lack of variation in pitch and loudness and poor breath control compromised the use of stress, rhythm and intonation. Breathy voice and excessive nasal resonance limited AB's ability to produce qualitative distinctions between vowels. A reduction in intra-oral air pressure compromised consonant production, particularly plosives and fricatives.
Unit 6.3 Speech evaluation
(1) Which of the following is a feature of AB's speech production?
(2) AB was reported to make ‘uneconomical use of air’. Describe two ways in which this description applies to AB's speech production.
(3) A spectrogram was used in the assessment of AB's speech production. It is one of several techniques which can be used to analyse dysarthric speech. Several others are listed below. For each technique, indicate if it is a type of perceptual, acoustic or physiological assessment:
(4) Describe two ways in which the articulation of plosive sounds is compromised in AB.
(5) Explain how disturbances at the phonatory level produce prosodic anomalies in AB's speech.
Focus on mixed dysarthria
AB's speech disorder was diagnosed as a mixed flaccid-spastic dysarthria. Individual deviant speech parameters could be attributed to spasticity and/or flaccidity. AB's slow rate of speech and articulatory imprecision could be attributed to spasticity which limits the range, force and speed of articulatory movements. Poor adduction and abduction of the vocal folds, manifested in a breathy voice and audible inspiration, was suggestive of a flaccid condition of the vocal folds. However, an indirect laryngoscopy was not performed and so this impression could not be confirmed. AB's breathiness might also be explained by spasticity. A spastic condition of the vocal folds, manifested in extreme tension of the folds and their reduced elasticity, could also explain AB's problems with high monopitch and monoloudness.
AB's palatal abnormality, which is responsible for his nasal emission and hypernasality, can be attributed to the combined effects of spasticity and flaccidity. The effect of spasticity on the palate is to produce a tendency towards downward movement. Flaccidity makes the palate too weak to counteract this movement. Because a flaccid weakness of the palate tended to predominate in AB, he had an incompetent velopharyngeal sphincter. AB's spasticity was exacerbated by the increased muscular effort needed to counteract the effects of his weak and fatiguing speech musculature. His general body tension rose as he made more effort to speak. As he made more effort to speak, the imbalance created by the asymmetrical nature of his spasticity was also exaggerated. The effect of these factors was heard as increasing inefficiency and weakening of articulations, the loss of control over coordination of breathing and phonation leading to increasing air wastage, and continuous nasal escape related to a breakdown of control over velopharyngeal valving.
Unit 6.4 Focus on mixed dysarthria
(1) AB appeared to have both flaccid and spastic involvement of the laryngeal musculature. Impairment of which of the following cranial nerves accounts for a flaccid weakness of the laryngeal musculature?
(2) Describe three effects of spasticity on AB's articulatory movements.
(3) Name one articulator in which there is combined flaccid and spastic involvement. Describe the effects of flaccidity and spasticity on this articulator. What type of prosthetic intervention might be appropriate in the case of this articulator?
(4) That a flaccid condition of the vocal folds is responsible for AB's phonatory abnormalities was suggested by the noticeable lower motor neurone involvement of the palate bilaterally. Explain the basis of this suggestion.
(5) The clinical impression of flaccidity of the vocal folds could not be confirmed by means of an indirect laryngoscopy. Explain what is involved in this procedure.
Assessment issues
The assessment of AB's speech focused on the functioning of speech production subsystems and the impact of deviant speech parameters on AB's intelligibility. The functioning of physiological mechanisms such as phonation and respiration and the impact of impairment of these mechanisms on speaker intelligibility correspond to the ‘body’ and ‘activity’ levels of the International Classification of Functioning, Disability and Health (ICF; World Health Organization, 2001). Lowit (Reference Lowit and Cummings2014: 400) states that ‘[a]t the body level, the functioning of the various speech subsystems, i.e. respiratory, laryngeal, and velopharyngeal function and oral musculature are investigated. In terms of the activity level, a variety of data elicitation methods are available to assess intelligibility, ranging from evaluations of single words and phrases to reading passages and spontaneous speech.’ The evaluation of these levels typically proceeds by means of published assessment protocols such as the Frenchay Dysarthria Assessment-2 (FDA-2; Enderby and Palmer, Reference Enderby and Palmer2008), which examines speech production under the following 11 sections: reflex; respiration; lips; jaws; palate; larynx; tongue; intelligibility; rate; sensation; and associated factors.
Today, dysarthria assessment is as likely to consider the impact of this speech disorder on an individual's participation in daily activities (the third level of the ICF framework) as it is on a speaker's intelligibility. During an assessment of dysarthria, it is at least as important for clinicians to consider the impact of dysarthria on an individual's self-esteem, quality of life and social participation as it is to assess the effect of respiratory, phonatory and articulatory impairments on a client's intelligibility. The need for assessment of the impact of dysarthria on a client's psychological wellbeing and participation could not be clearer. Piacentini et al. (Reference Piacentini, Mauri, Cattaneo, Gilardone, Montesano and Schindler2014) reported that dysarthria-related quality of life is significantly compromised in patients with multiple sclerosis and dysarthria, while Skolarus et al. (Reference Skolarus, Burke, Brown and Freedman2014) found that dysarthria is a predictor of participation restrictions in stroke survivors. A number of clinical tools have been validated for the purpose of assessing impact and participation, not all of which are designed specifically for clients with dysarthria. (The reader is referred to Lowit (Reference Lowit and Cummings2014) for a list of scales for the assessment of the psychosocial effects of communication disorders.)
Unit 6.5 Assessment issues
(1) Which of the following statements are true of dysarthria assessment according to the ICF framework?
The ICF framework addresses an individual's functioning and disability related to dysarthria within the context of activities and social roles.
The ICF framework considers poor respiratory support in dysarthria under body structure and function.
The ICF framework only addresses the relationship between physiological impairments and speech intelligibility in dysarthria.
The ICF framework considers environmental factors that can help or hinder participation in activities by the person with dysarthria.
The ICF framework does not address the speed, range and force of articulatory movements for speech production in dysarthria.
(2) Explain why an assessment of the intelligibility of the speaker with dysarthria should use different listeners, and scripted and unscripted speech tasks.
(3) What anomalies might you expect to record under the reflex and jaw sections of the FDA-2 in speakers with dysarthria?
(4) Describe how AB's dysarthria might adversely affect his participation in daily activities.
Introduction
The following exercise is a case study of a 35-year-old man (‘R’) who was studied by Day and Parnell (Reference Day and Parnell1987). R was diagnosed at 23 years of age with Wilson's disease. He has had a 10-year contact with speech-language pathology since his diagnosis. The case study is presented in five sections: primer on Wilson's disease; client history and presentation; speech intervention: part 1; speech intervention: part 2; and speech outcome.
Primer on Wilson's disease
Wilson's disease is an autosomal recessive disorder that affects copper metabolism, leading to toxic accumulation of copper in the liver, central nervous system and kidneys (Beinhardt et al., Reference Beinhardt, Leiss, Stättermayer, Graziadei, Zoller, Stauber, Maieron, Datz, Steindl-Munda, Hofer, Vogel, Trauner and Ferenci2014). The disorder is also known as ‘hepatolenticular degeneration’, a term which reflects damage to the liver (‘hepato’) and the lenticular nucleus of the basal ganglia (‘lenticular’) as a result of copper deposits. Wilson's disease is caused by mutations in the ATP7B gene (Lorincz, Reference Lorincz2010). The prevalence of the disorder is estimated to be 1:49,500 (Møller et al., Reference Mei and Morgan2011). Lai and Tseng (Reference Lai and Tseng2010) estimated the annual incidence rate to be 0.27 per 100,000. There is evidence of gender differences in Wilson's disease, with more men than women developing the neuropsychiatric form of the disorder, and more women than men developing the hepatic form (Litwin et al., Reference Litwin, Gromadzka and Członkowska2012). There is a good, long-term prognosis for those individuals with Wilson's disease who receive adequate care (Beinhardt et al., Reference Beinhardt, Leiss, Stättermayer, Graziadei, Zoller, Stauber, Maieron, Datz, Steindl-Munda, Hofer, Vogel, Trauner and Ferenci2014).
Neurological and psychiatric symptoms are a common feature of Wilson's disease. In a sample of 126 patients with the disease, Mihaylova et al. (Reference Mihaylova, Todorov, Jelev, Kotsev, Angelova, Kosseva, Georgiev, Ganeva, Cherninkova, Tankova, Savov and Tournev2012) reported neurological signs in 82 subjects. The most frequently observed signs were tremor and dysarthria. Rigidity, bradykinesia and pyramidal signs were found in over 25% of patients. Dystonia, chorea, athetosis, ballismus and epilepsy were rarely observed in these patients. Moores et al. (Reference Moores, Fox, Lang and Hirschfield2012) examined 48 adult patients with Wilson's disease, 21 of whom presented with neurological symptoms. Diagnostic magnetic resonance imaging revealed basal ganglia and brainstem abnormalities and atrophy in 64%, 64% and 36%, respectively. At follow-up, 50% exhibited basal ganglia lesions and 55% displayed atrophy. Individuals with Wilson's disease have an increased lifetime prevalence of psychiatric disorders, including major depressive disorders and bipolar disorders (Carta et al., Reference Carta, Sorbello, Moro, Bhat, Demelia, Serra, Mura, Sancassiani, Piga and Demelia2012).
There has been little systematic investigation of dysarthria in Wilson's disease. This is despite the fact that dysarthria is a common neurological symptom of the disorder. Machado et al. (Reference Machado, Chien, Deguti, Cançado, Azevedo, Scaff and Barbosa2006) reported dysarthria in 91% of a sample of 119 patients with Wilson's disease. An early study of 20 patients with Wilson's disease reported the presence of a mixed dysarthria, with prominent ataxic, spastic and hypokinetic features (Berry et al., Reference Berry, Darley, Aronson and Goldstein1974). The 10 most common speech production errors in these individuals were reduced stress, monopitch, monoloudness, imprecise consonants, slow rate, excess and equal stress, low pitch, irregular articulatory breakdown, hypernasality and inappropriate silences. Speakers with Wilson's disease exhibit an impaired speech rate and impaired control of speech rate (Pernon et al., Reference Pernon, Trocello, Vaissière, Cousin, Chevaillier, Rémy, Kidri-Osmani, Fougeron and Woimant2013). Dysarthria in Wilson's disease has been found to correlate with lesions of the putamen and caudate (Starosta-Rubinstein et al., Reference Starosta-Rubinstein, Young, Kluin, Hill, Aisen, Gabrielsen and Brewer1987).
Unit 7.1 Primer on Wilson's disease
(1) Wilson's disease is an autosomal recessive disorder. Using your knowledge of genetics, explain what is meant by the term ‘autosomal recessive disorder’.
(2) Individuals with Wilson's disease can exhibit bradykinesia. Which of the following statements best captures this neurological sign?
Bradykinesia describes rapid, erratic movement in Wilson's disease.
Bradykinesia describes slowness of movement in Wilson's disease.
Bradykinesia describes involuntary, writhing movement in Wilson's disease.
Bradykinesia describes an intention tremor in Wilson's disease.
Bradykinesia describes a postural tremor in Wilson's disease.
(3) Depending on the underlying neuropathology, some forms of acquired dysarthria are static in nature (they may change in their features but not in severity over time). Other forms of acquired dysarthria are progressive in nature (they worsen over time as the underlying disorder which causes them deteriorates). Still other forms of acquired dysarthria ameliorate over time (they display improvement as the underlying disorder which causes them improves). Is dysarthria in the well-managed client with Wilson's disease likely to remain static, deteriorate or improve over time?
(4) Damage to which of the following neuroanatomical areas and structures appears to be related to the presence of dysarthria in Wilson's disease?
Client history and presentation
In 1974, when R was aged 23 years, he began to experience dysarthria, drooling, dysphagia, decreased mental function and some dystonia. Subsequently, he went on to develop right foot drop, postural changes, clumsiness of the upper extremities and marked personality changes. These changes manifested as intermittent periods of depression. R was diagnosed as having Wilson's disease. His older sister had been diagnosed two years earlier with the disorder and had died shortly thereafter.
Following diagnosis, R was prescribed Penicillamine (an agent used for the mobilisation and elimination of copper) and was placed on a low-copper diet. However, R did not comply with either his drug or dietary regimen. Between 1974 and 1976, he contacted a number of specialists in psychiatry, internal medicine and speech-language pathology for assistance with his problems. These contacts were of limited duration with the exception of a period of psychiatric treatment for depression which lasted 18 months. R's speech deteriorated significantly during his psychiatric treatment. In April 1976, a psychiatrist remarked that ‘speech (had) deteriorated almost to the point of being completely nonunderstandable…a direct result of the neurological damage associated with the (Wilson's) disease’. The psychiatrist also expressed the view that ‘while (R's) speech might improve slightly, the chances of significant improvement (were) poor’. In the same year, R attempted suicide by means of a drug overdose. He was hospitalised in a mental health facility after a short period in an intensive care unit. His marriage failed during this time.
When R first attended the Columbia Speech and Hearing Clinic at the University of Missouri in 1976, he was already profoundly dysarthric. His speech was described as ‘unintelligible for the most part’. His speech was non-functional, and he relied on written messages and sign language for communication. However, these other modes of communication were also of limited effectiveness. R also presented with drooling and dysphagia, had a fixed, grimace-like expression, and had oral and facial rigidity. On account of his severe speech disorder, R had been unable to work for two years. Accordingly, he received full disability compensation under social security.
Unit 7.2 Client history and presentation
(1) State three features of R's history prior to diagnosis, which are consistent with the clinical profile of Wilson's disease.
(2) R displayed poor compliance with his drug and dietary regimen. Which feature of R's clinical presentation directly contributed to his poor compliance? Does this same feature have any implications for the management of this client in speech-language pathology?
(3) Do you think R is at risk of aspiration pneumonia? Provide support for your answer.
(4) Why do you think written messages and sign language, like speech, were of limited effectiveness for R?
Speech intervention: part 1
At the Columbia Speech and Hearing Clinic, R received intervention for his dysarthria during 22 of 28 consecutive semester sessions over a 10-year period. A range of therapeutic techniques were used to improve intelligibility. Progress was monitored through the use of intelligibility ratings performed by familiar and unfamiliar listeners. During the 10-year period of R's intervention, specific areas of emphasis and therapy procedures, and the length and complexity of target utterances were varied to meet R's changing needs and abilities. Medical supervision of R was maintained throughout this entire time. Even though certain drug and dietary controls were prescribed, R displayed poor compliance with them.
Between admission in 1976 and the winter semester in 1977, R's speech intelligibility in clinic increased significantly. Oral-motor exercises which were aimed at improving the flexibility and precision of the oral structures were attempted initially. However, these produced little gain and were consequently abandoned. There was also an early emphasis on increased vocal volume and differentiation of vowel productions. However, this also made little contribution to the improvement of intelligibility. The focus of therapy then turned for several years to the production of single consonants and consonant blends and clusters. The production of multisyllabic words and word-final consonants was particularly difficult for R and made a large contribution to his reduced intelligibility. R was encouraged to engage in self-monitoring of his productions and, with the assistance of the therapist, to achieve consistency in his standards of judgement. His reliance on gestural communication, which was largely confusing and unsuccessful, was discouraged. Throughout this time, R refused to consider the use of an augmentative or alternative communication system.
Unit 7.3 Speech intervention: part 1
(1) R's progress in therapy was monitored through the use of intelligibility ratings by familiar and unfamiliar listeners. Under which of the following conditions is R's speech likely to be rated as most intelligible?
A familiar listener rates R's production of an unseen list of words.
An unfamiliar listener rates R's speech production during conversation.
A familiar listener rates R's production of an unseen list of sentences.
An unfamiliar listener rates R's production of an unseen list of phrases.
A familiar listener rates R's speech production during a conversation where the topic is known.
(2) Therapy was continually adjusted to meet R's changing needs and abilities. Why is this type of ongoing adjustment important in the context of R's dysarthria?
(3) Oral-motor exercises were attempted early in R's therapy. Which of the following are true statements about these exercises?
Oral-motor exercises aim to improve the strength and range of articulatory movements.
Oral-motor exercises focus on the accurate production of speech targets.
Oral-motor exercises are contra-indicated in progressive dysarthria.
Oral-motor exercises include tasks such as tongue protrusion and elevation.
Oral-motor exercises focus on the accurate production of non-speech targets.
(4) Describe two aspects of this intervention which may have been adversely affected by R's psychiatric problems.
(5) R displayed maladaptive compensatory behaviour in response to his severe speech disorder. What is this behaviour? Why is it described as ‘maladaptive’?
Speech intervention: part 2
After intervention on the production of individual speech sounds proved to have limited benefit for speech intelligibility, the focus of intervention shifted to the use of suprasegmental guidelines on a continuous basis in contextual speech. The first two of these four guidelines emphasised the use of slowed rate and syllable-by-syllable production. This had a marked, positive effect on speech intelligibility for R. In fact, so considerable was the increase in R's intelligibility that he was able to secure part-time employment in 1980 for the first time since his diagnosis. In addition to these techniques, R was encouraged to make use of adequate respiratory support and appropriate pausing. He also received instruction in the use of stress and intonation patterns. However, these latter techniques were not as effective at improving intelligibility as slowed rate and syllable-by-syllable production. The third guideline encouraged the use of overarticulation within R's compensatory techniques. This required R to exaggerate articulatory movements. The fourth and final guideline, which complemented the third guideline, encouraged R to make use of increased mouth opening. This also increased R's intelligibility considerably. Notwithstanding these gains, R's motor speech skills were still highly vulnerable to the effects of physical fatigue. He was advised to rearrange his schedule in order to obtain sufficient rest, especially prior to therapy sessions. Because this advice was not always acted upon, R's compliance with this recommendation became a precondition for his enrolment in further therapy.
R's intelligibility was also compromised by hypernasality. R's hypernasal speech did not respond to traditional therapy techniques. Accordingly, a palatal lift appliance was recommended, which R used for approximately two years. By 1983, R's hypernasality had improved so much that even on days when he did not wear his palatal lift to therapy, his hypernasal speech had diminished considerably. Eventually, R was able to maintain improvements in his velopharyngeal control in the absence of the device, only resorting to its use during periods of fatigue.
Although R made considerable speech gains in clinic, he failed to generalise the use of his compensatory guidelines to communicative situations outside of clinic. Consistent with the therapeutic goal of helping R achieve optimal intelligibility and functional speech that was appropriate to his communicative needs in a range of settings, R was encouraged to assume ever greater responsibility for self-evaluation of his intelligibility and his use of the guidelines. Daily logs, which included ratings of intelligibility and consistency in use of the guidelines, were used for this purpose. Both R and his communicative partners completed these logs on a consistent basis. There was some deterioration in R's speech performance in the summer semester in 1985 when these logs were not completed. R married for the second time in 1983. R's wife occasionally attended therapy sessions in order to become acquainted with objectives and techniques which she could implement at home. It is expected that with greater involvement of R's wife in providing support, behaviour maintenance and feedback to R, he might be able to be discharged permanently from therapy.
Unit 7.4 Speech intervention: part 2
(1) Practice on speech sound production was minimally effective in terms of improving R's intelligibility. Accordingly, the focus of therapy changed to the implementation of suprasegmental guidelines. Which of the following speech production subsystems is targeted by these guidelines?
(2) Explain how slowed rate serves to increase the intelligibility of R's speech.
(3) Traditional therapy techniques did not improve R's hypernasality. Name one such technique. What is known about the efficacy of this particular technique?
(4) R achieved a satisfactory result in terms of resonation through the use of a palatal lift appliance. Explain how this appliance works to reduce hypernasal speech.
(5) Generalisation of improved speech skills beyond the clinic was an area of difficulty for R. What two main approaches were adopted to ensure that generalisation was achieved?
Speech outcome
R received intervention for his dysarthria over a 10-year period. At the outset of therapy, R was judged to have only 5% intelligibility (rated sentence by sentence) in connected speech. By the end of therapy, this had increased to an average of 95% intelligibility. During his 10-year period of intervention, R experienced several episodes when there were significant decreases in his intelligibility. These episodes could be accounted for by factors in R's lifestyle which he did not adequately manage and by R's underlying neurological disorder. When audiotaped samples of R's conversational speech from 1977 and 1985 were analysed and ranked according to the relative prominence of deviant speech features, it was found that whereas reduced intelligibility was first-ranked in 1977, it had dropped to fifth-ranked in 1985. This reflected R's success in using his compensatory techniques to achieve the major goal of treatment, optimal intelligibility and functional speech. The most prominent deviant speech features recorded in 1985 were imprecise consonants and prolonged phonemes. R's improved communicative status has enabled him to engage in full-time employment for the last three years. He has been remarried for two years and is the father of an infant son.
Unit 7.5 Speech outcome
(1) What contribution did R's articulation of individual speech sounds make to his overall intelligibility by the end of therapy?
(2) Throughout the 10-year period of R's intervention, his intelligibility decreased on certain occasions. Describe two factors which contributed to these episodes of reduced intelligibility in R.
(3) Increasingly, speech-language pathologists are asked to defend the cost-effectiveness of their interventions to clients. How would you defend the cost-effectiveness of the intervention that R has received?
(4) Charting R's speech progress over an extended period of time posed a number of challenges. Describe two such challenges.
(5) The decision to continue therapy in order to maximise the intelligibility of R's speech was motivated in part by his refusal to accept a form of augmentative or alternative communication. What does this decision reveal about how therapy can best be conducted?
Introduction
The following exercise is a case study of a man aged 71 years who was studied by Peach and Tonkovich (Reference Peach and Tonkovich2004). This client developed apraxia of speech (AOS) following a cerebrovascular accident. His case is somewhat unusual in that his AOS was caused by a subcortical haemorrhage of the basal ganglia. Most cases of AOS reported in the literature arise on account of cortical damage. The client also had stroke-induced aphasia. The case study is presented in five sections: primer on apraxia of speech; medical history; early post-stroke period; language assessment; and focus on speech.
Primer on apraxia of speech
McNeil et al. (Reference McNeil, Robin, Schmidt and McNeil2009: 264) state that ‘apraxia of speech is a phonetic-motoric disorder of speech production’. This definition is extended to include the locus of breakdown in speech production – AOS is caused when well-formed phonological frames are not efficiently translated into the kinematic patterns that are used for carrying out intended movements. This inefficiency is manifested as temporal and spatial segmental and prosodic distortions both within and between articulators. The durations of consonants and vowels and the time between sounds, syllables and words may be extended as a result. The perceptual consequences may be heard as sound substitutions, the mis-assignment of stress, and other phrase- and sentence-level prosodic abnormalities. The location of speech errors within utterances is relatively consistent and the type of errors is invariable. (It should be noted that some researchers (e.g. Staiger et al., Reference Staiger, Finger-Berg, Aichert and Ziegler2012) state that the invariability or consistency of speech errors is contentious at best, and should not be included as a criterion in the diagnosis of AOS.) AOS is not related to deficits of muscle tone or reflexes. It is also not related to deficits of sensory and language processing. AOS rarely occurs in pure or isolated form. When it does, it is not accompanied by deficits of basic motor physiology, perception or language.
Little is known about the epidemiology – prevalence and incidence – of AOS. Duffy (Reference Duffy2005) reported that AOS accounted for 7.6% of all motor speech disorders diagnosed in the Mayo Clinic Speech Pathology practice between 1987 to 1990 and 1993 to 2001. This figure was based on 6,101 evaluations of people with a primary speech pathology diagnosis of a neurologic motor speech disorder. AOS is most frequently caused by cerebrovascular accidents. However, there is also a neurodegenerative form of AOS called primary progressive AOS (Duffy et al., Reference Duffy, Strand, Clark, Machulda, Whitwell and Josephs2015). There is still no consensus on the neuroanatomical location of the lesion(s) that are associated with AOS. However, potential regions include Broca's area, the lateral premotor cortex, subcortical structures and the anterior insula, all in the left hemisphere (Robin and Flagmeier, Reference Robin, Flagmeier and Cummings2014). As described above, pure AOS is a rare occurrence. AOS is much more likely to be found alongside dysarthria, aphasia and/or oral apraxia. Botha et al. (Reference Botha, Duffy, Strand, Machulda, Whitwell and Josephs2014) reported that non-verbal oral apraxia is very common among patients with progressive AOS, and that the severity of AOS is predictive of oral apraxia. The presence of these other conditions makes a differential diagnosis of AOS difficult. However, there is evidence that specialist speech and language therapists display high intra-rater and inter-rater reliability in diagnosing the presence and severity of AOS in clients with communication difficulties following stroke (Mumby et al., Reference Mumby, Bowen and Hesketh2007).
Unit 8.1 Primer on apraxia of speech
(1) Which of the following are true statements about apraxia of speech?
AOS is a disorder of language encoding.
The production of vowels and consonants is compromised in AOS.
AOS arises on account of muscle atrophy and reduced tone (hypotonia).
Automatic speech production is superior to volitional speech production in AOS.
Prosodic abnormalities in AOS are caused by respiratory difficulties.
(2) It was described above that AOS can be caused by cerebrovascular accidents and neurodegenerative disorders. Name three other causes of AOS.
(3) A Cochrane systematic review of AOS stated that ‘there are no good epidemiological data on the prevalence of apraxia of speech’ (West et al., Reference West, Hesketh, Vail and Bowen2005: 3). Which of the following statements best explains the lack of epidemiological data on AOS, according to the Cochrane reviewers?
AOS is a rare disorder and epidemiological studies are not a priority for funding in consequence.
Epidemiological studies of AOS are not a priority for funding because the disorder has few implications for an individual's quality of life.
Epidemiological studies are hampered by a lack of a universally agreed definition of AOS.
Epidemiological studies of AOS are not a priority for funding because the disorder has few implications for an individual's ability to communicate.
Epidemiological studies are hampered by difficulty in making a differential diagnosis of AOS, dysarthria and aphasia.
(4) Botha et al. (Reference Botha, Duffy, Strand, Machulda, Whitwell and Josephs2014) found that non-verbal oral apraxia is very common among patients with progressive AOS. Why do you think this is the case?
(5) Depending on the condition that causes AOS, the speech disorder may be static or progressive in nature. Name one condition which causes static AOS, and one condition which causes progressive AOS.
Medical history
The client is a 71-year-old, right-handed man. He presented with an acute loss of speech and right hemiplegia following a cerebrovascular accident. Prior to his CVA, his medical history was unremarkable. Three days post-onset a CT scan was performed. It revealed a large, left frontal haemorrhage that probably originated in the region of the basal ganglia and extended into the frontal white matter. The lower half of the primary motor cortex, the posterior portion of the inferior frontal gyrus, the insula and the postcentral opercular structures were not involved.
Unit 8.2 Medical history
(1) Which of the following statements best captures the type of CVA that this client sustained?
The client sustained a cerebral embolism of the left cerebral hemisphere.
The client sustained a brainstem stroke.
The client sustained a cerebral embolism of the right cerebral hemisphere.
The client sustained a cerebral haemorrhage of the dominant hemisphere.
The client sustained a cerebral haemorrhage of the non-dominant hemisphere.
(2) The client developed a right hemiplegia as a result of his stroke. Describe three implications of a right hemiplegia for SLT assessment and intervention.
(3) This client's stroke probably originated in the region of the basal ganglia. Which of the following are true statements about the basal ganglia?
Damage to the basal ganglia only has implications for motor control.
The basal ganglia include the caudate, putamen and globus pallidus.
The basal ganglia are a number of cortical nuclei.
Damage to the basal ganglia can result in dyskinesias.
The basal ganglia are involved in language processing and motor planning and control.
Early post-stroke period
Ten days after his stroke, the client was admitted to rehabilitation. He was alert but inconsistently responsive when an initial speech-language evaluation was performed. The client exhibited muteness and occasionally used simple gestures to refer to his inability to speak and understand questions. He used undifferentiated pointing responses to tasks that required auditory word discrimination and the matching of visual words to pictures. The client displayed no appropriate responses to questions in either formal or informal conversational contexts. Occasionally, when functional commands were presented in an appropriate context, he was able to follow them. Writing was impaired, with the non-preferred hand used to produce an unintelligible scribble.
A programme of speech-language intervention was initiated. During the next two weeks, the client exhibited minimal vocalisation, and spontaneously used a few grammatically well-formed sentences. Bucco-facial apraxia compromised his imitation of oral movements. He began to respond successfully to tasks that elicited automatic verbal responses by the end of the fourth week post-stroke. However, his speech remained aphonic. His inability to imitate speech consistently frequently frustrated him. There was moderate impairment of word recognition and auditory comprehension of yes–no questions. By pointing to an alphabet board, he was able to spell one simple word out of three.
His speech output at five weeks post-stroke was much improved from his initial appearance. However, he continued to be dysfluent – there was reduced phrase length and poor grammatical complexity – and he had substantial difficulty initiating speech. He was echolalic and perseverative. In conversation, there were occasional, but more frequent grammatically well-formed sentences of normal lengths. Although he was able to read sentences aloud, he did so with substantial difficulty. Through the use of self-cuing he was able to increase the consistency of vocalisation during speech production. There was mild impairment of auditory comprehension for word recognition. Limb apraxia made it difficult for him to follow commands using parts of his body. The client's naming was poor and was influenced by linguistic variables such as frequency of occurrence, open versus closed class and concrete versus abstract. Verbal paraphasias were also observed.
Unit 8.3 Early post-stroke period
(1) Is there any evidence that this client has phonatory apraxia? Provide support for your answer.
(2) Respond with true or false to each of the following statements:
(3) Three linguistic variables were found to influence the client's naming. Give one example of each of these variables, and indicate how each variable may be manifested in the client's naming.
(4) By the end of the fourth week post-stroke the client began to produce verbal responses to tasks. Is there anything significant about the responses that the client produced?
(5) Is there any evidence that the client exhibits semantic deficits during naming? Provide evidence to support your answer.
Language assessment
The first formal assessment of the client's speech and language skills was undertaken at 6 weeks post-onset, when the Boston Diagnostic Aphasia Examination (BDAE; Goodglass and Kaplan, Reference Goodglass and Kaplan1983a) was conducted. The client's speech production was aphonic and effortful. He displayed trial and error behaviour, groping articulatory movements and attempts at self-correction. His speech displayed dysprosody which was unrelieved by extended periods of normal rhythm, stress and intonation. He had difficulty initiating utterances and his speech was perceived to contain phoneme substitutions. His description of the cookie theft picture from the BDAE is shown below:
(Examiner: What's happening with her?) With her? She's overflowing the sink…and…he's /s/…(Examiner: How ’bout over there?) Over there? He /kæraher/ it in /e/ /ki/ it's a… (expletive)…/fo folling/ it's cookie jar…he's about to fall off…and hurt hisself.
The client's performance on the various subtests of the BDAE revealed a mild to moderate aphasia. The Rating Scale Profile of Speech Characteristics revealed that articulatory agility and paraphasia in running speech were the two most impaired areas, while repetition and auditory comprehension were areas of relative strength. The client's melodic line, phrase length, grammatical form and word-finding were disrupted, but were not as severely impaired as articulatory ability and paraphasia. This pattern of deficits did not correspond to any of the classical aphasia syndromes. The client's performance on each subtest of the BDAE is shown below:
Auditory Comprehension:
Word discrimination (69/72)
Body part identification (17/20)
Commands (12/15)
Complex ideational material (8/12)
Oral Expression:
Oral agility (10/12)
Verbal agility (14/14)
Automatised sequences (5/8)
Repetition of words (8/10)
Repeating phrases (high probability) (8/8)
Repeating phrases (low probability) (7/8)
Visual confrontation naming (102/105)
Body part naming (29/30)
Reading Comprehension:
Symbol and word discrimination (10/10)
Word recognition (8/8)
Comprehension of oral spelling (7/8)
Word–picture matching (9/10)
Reading sentences and paragraphs (9/10)
Mechanics of writing (1/3)
Primer-level dictation (14/15)
Written confrontation naming (3/10)
Unit 8.4 Language assessment
(1) Give one example from the cookie theft picture description of each of the following features:
(2) How might the client's prosodic difficulties be related to other features of his verbal output?
(3) The client's pattern of deficits did not correspond to any of the classical aphasia syndromes. Five such syndromes are listed below. For each syndrome, indicate one feature which sets it apart from the client's particular language problems.
(4) The following items are taken from the BDAE. Each item is used to assess either limb/hand praxis or bucco-facial/respiratory praxis. Assign each of these items to one of these two categories.
The client is asked: ‘How would you show there is too much noise?’.
The client is asked: ‘Let me hear you cough’.
The client is asked: ‘How would you pretend to stop traffic?’.
The client is told: ‘Pretend to sip through a straw’.
The client is asked: ‘How would you show that you are too cold?’.
Focus on speech
A detailed assessment of the client's speech was undertaken. The client orally read a series of word lists that sampled 45 voiced and unvoiced stop, fricative, affricate, nasal, semi-vowel and consonant cluster phonemes. Each phoneme or blend was sampled in initial, medial and final positions of words. Single phonemes were examined in words which were one to two syllables in length, while blends were examined in words of one to three syllables. Two experienced judges undertook broad phonemic transcriptions of a total of 1,057 audiotaped responses. Two types of phoneme errors were excluded from the analysis. First, phonemes which were produced in place of a target phoneme in a word were not included in the analysis. Second, substitutions of voiceless for voiced cognate phonemes were also omitted. These exclusions resulted in 77 (25%) of the total errors undergoing analysis. It was found that significantly more substitution errors were produced than other error types, followed by additions, repetitions, the use of intrusive schwa and finally omissions. Significantly more phoneme errors occurred in word initial position than in word medial and final positions. There were similar percentages of errors across different phoneme groupings (consonant cluster, fricative, nasal, etc.).
Unit 8.5 Focus on speech
(1) Monosyllabic and multisyllabic words were used to elicit the production of phonemes by the client. From your knowledge of AOS, would you expect speech errors to be more common or less common in monosyllabic versus multisyllabic words?
(2) The client has difficulty initiating speech. In view of this, where would you expect most speech errors to occur? Select one of the following as your answer: word initial position; word-medial position; word-final position.
(3) Why do you think all substitutions of voiceless phonemes for voiced cognate phonemes were omitted from the analysis?
(4) One of the speech errors produced by the client is the use of intrusive schwa. This is a relatively common speech feature of AOS. Why do you think this feature occurs?
Introduction
The following exercise is a case study of a 32-year-old, Dutch-speaking woman (‘TDF’) who was studied by Van Borsel et al. (Reference Van Borsel, Janssens and Santens2005). TDF presented at the neurological department of a university hospital with speech problems of sudden onset. Although her history revealed noteworthy neurological events, her speech problems were considered to be of psychogenic origin. The case study is presented in five sections: primer on foreign accent syndrome; client history and medical investigations; language and oral motor evaluation; focus on articulation and prosody; and focus on accent.
Primer on foreign accent syndrome
Kuschmann and Lowit (Reference Kuschmann and Lowit2012) define foreign accent syndrome (FAS) as a ‘motor speech disorder in which a variety of segmental and suprasegmental errors lead to the perception of a new accent in speech’ (738). To date, there have been no epidemiological investigations of this speech disorder, although there is general consensus that the condition is rare. Typically, the disorder has a neurogenic aetiology. FAS has been reported in adults following cerebral infarction (Sakurai et al., Reference Sakurai, Itoh, Sai, Lee, Abe, Terao and Mannen2015; Trax and Mills, Reference Trax and Mills2013), traumatic brain injury (Lippert-Gruener et al., Reference Lippert-Gruener, Weinert, Greisbach and Wedekind2005) and the development of brain tumours (Tomasino et al., Reference Tomasino, Marin, Maieron, Ius, Budai, Fabbro and Skrap2013). The speech disorder has also been documented in adults with neurodegenerative disorders such as multiple sclerosis (Chanson et al., Reference Chanson, Kremer, Blanc, Marescaux, Namer and de Seze2009). Less commonly, a psychogenic aetiology is presumed to underlie the disorder. Verhoeven et al. (Reference Verhoeven, Mariën, Engelborghs, D'Haenen and De Deyn2005) described FAS in the case of a Dutch-speaking adult with conversion disorder. A developmental form of FAS has been described in two child patients by Mariën et al. (Reference Mariën, Verhoeven, Wackenier, Engelborghs and De Deyn2009).
Linguistic investigations of FAS have focused primarily on the production of segments and use of intonation in speakers with the disorder. Verhoeven and Mariën (Reference Verhoeven and Mariën2010) described pronunciation problems at the segmental level in a female speaker of Belgian Dutch who developed a French/German foreign accent after a left hemisphere stroke. Many of this speaker's vowels had clear creaky voice. There was a substantially smaller vowel space and less acoustic differentiation between [i], [ɪ] and [e]. There was a tendency to devoice fricatives and stops. Velar fricatives were pronounced as velar stops, and the glottal fricative was almost consistently realised as a glottal stop in word-initial position. The alveolar trill was systematically pronounced as a uvular trill, which is a typical feature of French learners of Dutch.
Intonation and other aspects of speech prosody have been extensively examined in FAS. Katz et al. (Reference Katz, Garst and Levitt2008) reported inaccurate and highly variable lexical stress assignment in a 46-year-old, monolingual female who presented with FAS of unknown aetiology. This client's sentence-level intonation also showed occasional deviations from typical American English patterns. Kuschmann and Lowit (Reference Kuschmann and Lowit2012) studied the pragmatic use of intonation in four speakers with FAS. Specifically, the use of phonetic parameters (fundamental frequency, intensity and duration) and phonological categories (pitch accents and de-accentuation) to signal information status was examined. Although speakers with FAS were able to use phonetic parameters to differentiate between given and new information, they frequently placed pitch accents on given information instead of de-accenting these elements. The foreign qualities of the Dutch-speaking adult described by Verhoeven et al. (Reference Verhoeven, Mariën, Engelborghs, D'Haenen and De Deyn2005) extended beyond pronunciation to include features of the lexicon, syntax and pragmatics.
Unit 9.1 Primer on foreign accent syndrome
(1) Respond with true or false to each of the following statements about the aetiology of FAS:
A client may present with FAS in the absence of a known aetiology.
FAS is most often associated with psychogenic factors.
Cerebral neoplasms are part of the neurogenic aetiology of FAS.
FAS may be related to the onset of neurodegenerative disease in adults.
FAS in a client may be associated with neurogenic and psychogenic factors.
(2) The speaker with FAS who was studied by Tomasino et al. (Reference Tomasino, Marin, Maieron, Ius, Budai, Fabbro and Skrap2013) displayed no signs of dysarthria, apraxia of speech, or aphasia. How typical is this case of FAS in general?
(3) The speaker with FAS who was studied by Verhoeven and Mariën (Reference Verhoeven and Mariën2010) was described as producing pronunciation errors that resulted from articulatory ‘overshoot’ of the active articulator (i.e. the active articulator overshoots its target). What two features of this client's speech are examples of articulatory overshoot?
(4) The speaker described in question (3) also produces the following speech errors: [k > x] and [t > s]. How would you characterise these errors?
(5) The speakers with FAS who were studied by Kuschmann and Lowit (Reference Kuschmann and Lowit2012) frequently placed pitch accents on given information. Explain why this is problematic in terms of signalling information status during communication.
Client history and medical investigations
TDF first visited the neurological department of the authors’ university hospital because of speech problems of sudden onset. Her medical history contained several, noteworthy features. Since the age of 6, TDF had a right-sided neurosensory hearing loss with sloping configuration. A head trauma and whiplash injury were sustained nine years earlier. This caused chronic headache with variable lateralisation which was predominant in the occipito-nuchal and parietal region. An otorhinolaryngologist had been consulted one month earlier for a hoarse voice following a minor head trauma. However, a clinical ENT examination was normal: no structural abnormalities were revealed by flexible laryngoscopy and the voice sounded normal to the otorhinolaryngologist. It was shortly after this ENT consultation that TDF's speech problems appeared suddenly during an evening out with friends. TDF was described as being mute for some time after the onset of her speech difficulties. A clinical neurological examination was also normal. There were no motor or sensory impairments. Pathological reflexes were absent, and tendon reflexes were symmetrical. The results of coordination, posture and gait tests were normal. A whole brain CT scan was also normal.
TDF experienced significant psychiatric problems. She was being treated for depression and suicidal ideation at the time of the study. This was related to family problems. Specifically, TDF's husband had rapidly progressing Huntington's disease. Yet, she had been kept unaware of the family history in relation to this condition. TDF had concerns about the implications of this disease for her 10-year-old son who had a learning disorder. TDF took two antidepressants, sertraline and trazodone. However, neither drug is known to have any effect on speech either singly or in combination. A further drug, prazepam, was also administered to TDF. (Prazepam is a benzodiazepine which is used in the treatment of anxiety disorders.) This drug can cause slurred speech when given in high doses. However, TDF did not receive high doses of this drug.
Unit 9.2 Client history and medical investigations
(1) TDF had neurosensory hearing loss with sloping configuration. What does ‘sloping configuration’ mean?
(2) TDF's history reveals two episodes of head injury. Is either episode a likely cause of TDF's speech problems? Provide support for your answer.
(3) A clinical ENT examination of TDF, which included the use of flexible laryngoscopy, revealed no structural laryngeal abnormality. In this case, is a diagnosis of psychogenic dysphonia warranted?
(4) TDF's drug regimen included prazepam. What motor speech disorder is caused by this drug when it is taken in high doses?
Language and oral motor evaluation
The results of a number of language assessments indicated that TDF did not have aphasia. The maximum score was obtained on the Dutch version of the Token Test (Van Dongen et al., Reference Van Dongen, Van Harskamp and Luteijn1976) and on a Dutch aphasia battery, the Stichting Afasie Nederland test (Deelman et al., Reference Deelman, Koning-Haanstra, Liebrand and Van Den Burg1981). TDF had intact comprehension of written language on the Dutch version of the Aachener Aphasie test (Graetz et al., Reference Graetz, De Bleser and Willmes1992). TDF could recite without error the days of the week, months of the year, and could count numbers from 1 to 20. Word and sentence repetition was also intact. There were no word-finding difficulties during confrontation naming or a word retrieval test. TDF could also read aloud without difficulty. Video-recorded speech samples revealed some grammatical difficulties. Some auxiliaries, articles and prepositions were omitted, giving TDF's speech a telegraphic quality at times. Grammatical errors, including the use of singular for plural nouns, incorrect verb conjugation and incorrect word order, were present but not pervasive. There was no paralysis, paresis or oral apraxia during oral motor testing.
Unit 9.3 Language and oral motor evaluation
(1) TDF displayed intact performance on the Dutch version of the Token Test. Which of the following linguistic abilities are assessed by means of this test?
(2) Which aspect of TDF's language performance suggests that (a) phonological long-term memory and (b) phonological short-term memory are intact?
Focus on articulation and prosody
Video-recorded speech samples of TDF were phonetically transcribed and analysed. The samples included recitation of automatic series, word and sentence repetition, reading aloud, confrontation naming, word retrieval, monologue and conversation. TDF displayed no struggle behaviour during speech. The use of auditory masking and delayed auditory feedback during reading aloud did not diminish TDF's accent. A number of articulatory errors were noted, some of which are shown below:
/ma:ntɑx/ for /ma:ndɑx/ (‘Monday’)
/ɑltɛi/ for /ɑltɛit/ (‘always’)
/di/ for /dri/ (‘three’)
/awaji/ for /hawaji/ (‘Hawaii’)
/spre:kə/ for /spre:kən/ (‘talk’)
Other, less common error patterns were the production of the trill sound /r/ with insufficient trill, and the substitution of /ɣ/ or /x/ for /h/. Several errors occurred on a single occasion: /ʃ/ for /s/, /j/ for /r/, /ŋ/ for /n/, /r/ for /n/, the addition of /ɣ/ in word-initial position, and vowel changes such as /ə/ for /ɔ/ and /ɛ/ for /u/.
TDF displayed a number of prosodic anomalies. Word and sentence stress were aberrant and TDF displayed a tendency towards scanning speech. Stress was placed on the wrong syllables in words. Incorrect word stress occurred on 18.1% of two-syllable words, 35.1% of three-syllable words, 62.5% of four-syllable words, and 30% of words of five or more syllables. The speech tasks with the highest level of incorrect word stress were confrontation naming (61.1%) and word retrieval (51.7%). Incorrect sentence stress occurred in 6.8% of the sentences produced. Stress was placed on the wrong word in these sentences.
Unit 9.4 Focus on articulation and prosody
(1) The use of auditory masking and delayed auditory feedback did not diminish TDF's accent. In what speech disorder do auditory masking and delayed auditory feedback have a facilitative effect?
(2) TDF did not display struggle behaviour during speech production. In what motor speech disorder is there considerable struggle behaviour?
(3) Characterise the type of articulatory errors that occur during the production of the following words: Monday; always; three; Hawaii; talk.
(4) TDF is described as displaying a tendency towards scanning speech. What is scanning speech?
Focus on accent
The perception of a foreign accent in TDF was confirmed by a listener experiment. A total of 33 third-year students in speech-language pathology, none of whom were familiar with foreign accent syndrome, listened to a speech sample of 6 minutes 25 seconds’ duration. The speech sample contained fragments of automatic speech, word repetition, reading aloud, monologue, conversation and confrontation naming. The subjects were asked to decide if the speech sample was from a native speaker of Dutch and, if not, which language was the speaker's mother tongue. All subjects expressed the view that TDF's speech was unusual, with 69.7% stating that Dutch was not the speaker's native language. Linguistic features which were judged to be significant in this assessment were prosodic abnormalities (improper word stress, scanning, strange intonation), grammatical errors (deletion of articles, improper word order, errors of pluralisation), use of short sentences and the occurrence of ‘strange sounding’ sounds.
Although nine different accents were perceived in total, most subjects indicated that TDF was likely to be a native of an Eastern European country. TDF's personal history revealed no source for this accent. TDF was born in the Dutch-speaking part of Belgium to parents who were native speakers of Dutch. TDF was raised in a Dutch-speaking environment and attended Dutch schools. She had never lived abroad, and had only ever undertaken short journeys, mainly to Spain. She studied French at introductory level at school. TDF's husband was also a native Dutch speaker.
TDF was seen one year later when she accompanied her husband to a neurological consultation. Her speech was nearly normal at this stage. Her foreign accent had gradually resolved within five months of onset. A second listener experiment was conducted with 13 students in speech-language pathology, none of whom had participated in the first listener experiment. Although all 13 subjects judged TDF's speech to be unusual, only one stated that TDF was not a native speaker of Dutch. However, this subject was unable to identify TDF's mother tongue.
Unit 9.5 Focus on accent
(1) The perception of a foreign accent in TDF's case was based on linguistic features as well as on prosodic and articulatory features. Which language level was particularly influential in this regard?
(2) Van Borsel et al. (Reference Van Borsel, Janssens and Santens2005) describe FAS as a listener-bound epiphenomenon, that is, as a product of the listener and not a syndrome in its own right. What feature of the listener experiments provides support for this view?
(3) The dominance of prosodic disturbances in FAS is somewhat problematic for the view that FAS is a speech disorder associated with left hemisphere damage. Explain why this is the case.
(4) Kuschmann and Lowit (Reference Kuschmann and Lowit2015) have argued that a combination of scripted and unscripted data is required in order to obtain a comprehensive picture of the intonation abilities of a speaker with FAS. How is this realised in the listener experiments in this study?
(5) TDF's foreign accent resolved spontaneously within five months of onset. What does this suggest about the origin of TDF's speech disorder?


