
Introduction
The following exercise is a case study of a 51-year-old man (‘PT’) with contact granuloma who was studied by Patel et al. (Reference Patel, Pickering, Stemple and Donohue2012). PT is a college professor and speech-language pathologist who had a history of hoarseness and other vocal symptoms. The case study is presented in five sections: primer on organic dysphonia; client history; voice evaluation; voice therapy; and post-intervention vocal function.
Primer on organic dysphonia
An organic dysphonia is a voice disorder which is caused by disease, illness or injury. An organic voice disorder may be structural in nature. Examples include a range of benign and malignant growths which can degrade laryngeal structures or compromise their function. An organic voice disorder may be related to neurological damage such as when a laryngeal nerve is severed during surgery (e.g. thyroidectomy), leading to vocal fold paralysis and paresis. Alternatively, neurodegenerative diseases (e.g. Parkinson's disease) and events such as cerebrovascular accidents (strokes) can give rise to an organic voice disorder. Other causes of organic dysphonias include laryngeal trauma, endocrine disorders, infectious diseases, gastroesophageal reflux, auto-immune diseases (e.g. rheumatoid arthritis), age-related degeneration and pharmacological agents. Any of these conditions and agents can impair the structure and function of the larynx, resulting in organic voice disorders of varying severity.
Organic dysphonias have a high prevalence in the general population and are a significant economic burden to individuals and society. Bhattacharyya (Reference Bhattacharyya2014) reported that 17.9 million adults in the US have a voice problem, a figure which yields a population prevalence of 7.6%. Voice problems resulted in 7.4 lost workdays in a 12-month period. Infectious laryngitis and gastroesophageal reflux disease were present in 17.8% and 8.0% of adults with voice disorders, respectively. Stein and Noordzij (Reference Stein and Noordzij2013) reported a yearly incidence of 3.47 cases of chronic laryngitis per 1,000 people in a population of 40,317 people who were seen at an urban academic medical centre from 2009 to 2010. The prevalence of voice disorders is higher in certain occupations and age groups in comparison to the general population. In a national survey of 1,879 teachers in New Zealand, Leão et al. (Reference Leão, Oates, Purdy, Scott and Morton2015) found the prevalence of self-reported vocal problems on the day of the survey was 13.2%. The prevalence was higher still during the teachers’ careers and over the course of the teaching year (33.2% and 24.7%, respectively). In a systematic review of studies, de Araújo Pernambuco et al. (Reference De Araújo Pernambuco, Espelt, Balata and de Lima2015) reported the prevalence of vocal disorders in persons aged 60 years or more to range from 4.8% to 29.1%.
A contact granuloma is one type of benign growth that can cause an organic voice disorder. Other terms for this disorder in the literature are laryngeal contact ulcer, vocal fold granuloma, post-intubation granuloma and arytenoid granuloma. A contact granuloma typically occurs on the posterior third of the true vocal fold, usually in the area of the vocal process of the arytenoid cartilage. The ulceration may be unilateral or bilateral and may present a ‘cup and saucer’ appearance, with a protuberance on one side and a crater or concavity on the other side (Colton et al., Reference Colton, Casper and Leonard2006: 180). Several factors are associated with the development of contact granulomas including vocal abuse, habitual throat clearing, laryngopharyngeal reflux and intubation. Few studies have examined the prevalence of contact granuloma. The prevalence of intubation granuloma is low, in one study accounting for only 2 of 167 (1.2%) adult patients whose tracheas were intubated during surgery (Jones et al., Reference Jones, Catling, Evans, Green and Green1992). Contact granulomas may be treated by surgery, voice therapy and the pharmacological management of laryngopharyngeal reflux. Recurrence rates following surgical excision have been reported to approach 92% (Carroll et al., Reference Carroll, Gartner-Schmidt, Statham and Rosen2009).
Unit 37.1 Primer on organic dysphonia
(1) The following conditions are all causes of organic voice disorders. For each condition, indicate if the aetiology is an infectious disease, a neurodegenerative disorder, or a laryngeal trauma:
(2) The following scenarios describe clients who have organic voice disorders. For each scenario, indicate if the aetiology is an endocrine disorder, an autoimmune disease or a pharmacological agent:
A 51-year-old woman develops vocal symptoms during the menopause.
A 65-year-old man, who takes aspirin, reports voice problems to his doctor.
A 55-year-old woman with Sjögren's syndrome reports poor voice-related quality of life to her speech pathologist.
A 60-year-old woman with hypothyroidism experiences hoarseness.
A 30-year-old bodybuilder, who uses anabolic steroids regularly, develops vocal symptoms.
(3) Which of the following are true statements about contact granulomas:
Contact granulomas develop at the middle of the vocal folds.
Contact granulomas respond to treatment using proton pump inhibitors.
Contact granulomas are more prevalent in children than in adults.
Contact granulomas are more prevalent in men than in women.
Contact granulomas are an age-related laryngeal pathology.
(4) There is a higher prevalence of voice disorders in people aged over 60 years. State one organic voice disorder that is associated with advancing years.
Client history
PT is a 51-year-old college professor and speech-language pathologist. An otolaryngological examination conducted four months before the start of the study revealed a contact granuloma on the left vocal process. PT has a history of laryngopharyngeal reflux. PT reported a number of vocal symptoms including vocal fatigue, hoarseness after teaching a long class and the occasional sensation of a lump in the throat in the morning. PT was also diagnosed with sulcus vocalis along the anterior one-third margin of the right vocal fold. Following diagnosis, PT was prescribed a proton pump inhibitor which he took once daily. He also adhered to anti-reflux dietary and behavioural precautions. However, a monthly stroboscopic examination of the vocal folds revealed that there was little change in the lesion size and voice quality did not improve significantly. Given the heavy professional demands on PT's voice and the persistence of his hoarseness, PT was recommended to receive voice therapy.
Unit 37.2 Client history
(1) PT has a history of laryngopharyngeal reflux (LPR). The prevalence of voice disorders in individuals with LPR is considerably higher than in the general population (Spantideas et al., Reference Spantideas, Drosou, Karatsis and Assimakopoulos2015). Explain how LPR causes laryngeal damage. State one laryngeal pathology that has been linked to LPR (do not include contact granuloma in your response).
(2) PT reported a number of vocal symptoms. Which of these symptoms is likely to be related to vocal hyperfunction? Which of these symptoms is related to PT's laryngopharyngeal reflux?
(3) PT was also diagnosed with sulcus vocalis. Which of the following are true statements about sulcus vocalis?
Sulcus vocalis is characterised by a loss of the lamina propria, resulting in a deep, linear furrow along the free edge of the vocal fold.
Sulcus vocalis is not associated with phonotraumatic behaviour.
Sulcus vocalis may be treated by a vocal fold augmentation procedure.
Glottic insufficiency is generally not a feature of sulcus vocalis.
A thin band of mucosa (mucosal bridge) can run parallel to the vocal fold in sulcus vocalis.
(4) Respond with true or false to each of the following statements:
Voice evaluation
PT's voice was evaluated pre- and post-therapy using high-speed digital imaging, stroboscopy, acoustic analysis, aerodynamic analysis and perceptual assessments of voice quality.
High-speed digital imaging: A KayPentax high-speed system model 9710 was used to make these recordings. PT was required to sustain phonation of the vowel /i/ at typical pitch and loudness. He also completed a laryngeal diadochokinetic task of repeating /hi/ four times with short breaths between syllables. The following measurements were made pre- and post-therapy: voice onset time; open quotient; maximum amplitude; speed quotient (duration of lateral movement divided by the duration of medial movement); relative peak closing velocity; peak-to-average opening velocity; and peak-to-average closing velocity.
Stroboscopy: A stroboscopic assessment was performed using the KayPentax Digital Stroboscopy system RLS 9100b. Three speech-language pathologists undertook pre- and post-therapy ratings of stroboscopic imaging. These ratings were based on a visual perceptual assessment of glottal closure configuration and phase closure during sustained phonation of the vowel /i/ at comfortable pitch and loudness.
Acoustic analysis: The KayPentax Computerized Speech Laboratory was used to make pre- and post-therapy acoustic measurements of sustained phonation on the vowel /a/. The following measurements were made: maximum phonation time (in seconds); average fundamental frequency (hertz); jitter (%); low fundamental frequency (hertz); high fundamental frequency (hertz); shimmer (decibels); and noise-to-harmonic ratio.
Aerodynamic analysis: Expiratory volumes (millilitre) and mean expiratory airflow (litres per second) were measured using the KayPentax Phonatory Aerodynamic System no. 6600.
Perceptual assessment: The Consensus Auditory–Perceptual Evaluation of Voice (CAPE-V; Kempster et al., Reference Kempster, Gerratt, Verdolini-Abbott, Barkmeier-Kraemer and Hillman2009) was used by three speech-language pathologists to make a pre- and post-therapy perceptual assessment of PT's voice.
Unit 37.3 Voice evaluation
(1) High-speed digital imaging enables clinicians to perform accurate measurements of spatiotemporal vibratory features for the entire vocal fold image. Which of these measurements corresponds to the following descriptions?
Description 1: Duration of the cycle during which the vocal folds remain open divided by the duration of the entire cycle.
Description 2: Duration from initial vocal fold edge motion after complete abduction to the first vocal fold contact which is followed by steady-state cyclic oscillations.
(2) PT underwent a stroboscopic examination of the vocal folds. Explain how this instrumental assessment is conducted.
(3) Jitter and shimmer were two acoustic measurements recorded during voice evaluation. Which of the following statements captures these measurements?
Jitter and shimmer describe the cycle-to-cycle stability of fundamental frequency and amplitude, respectively.
Jitter and shimmer are the difference between the low and high fundamental frequency.
Jitter and shimmer are the difference between the maximum phonation time and the average fundamental frequency.
Jitter and shimmer are calculated by adding the noise-to-harmonic ratio to the maximum phonation time.
Jitter and shimmer describe the cycle-to-cycle stability of amplitude and fundamental frequency, respectively.
(4) Mean expiratory airflow was one of two aerodynamic measurements taken during PT's voice evaluation. How might the presence of a contact granuloma be expected to affect this measurement? How might a successful voice intervention affect this particular measurement?
(5) The CAPE-V was used to perform an auditory perceptual assessment of PT's voice. Which of the following are true statements about the CAPE-V?
The CAPE-V assesses voice across six parameters: overall severity; breathiness; roughness; strain; pitch; and loudness.
The CAPE-V is not suitable for use with paediatric voice patients.
The CAPE-V examines vocal performance during the production of sustained vowels, sentences and conversational speech.
The CAPE-V is not suitable for use with clients who have a neurogenic voice disorder.
The CAPE-V was developed from a consensus meeting sponsored by the American Speech-Language-Hearing Association.
Voice therapy
Over a period of six weeks, PT undertook vocal function exercises (VFEs) twice daily, once in the morning and once in the evening. The VFE approach (Stemple et al., Reference Stemple, Glaze and Klaben2000) is a type of physiological voice therapy which aims to improve: (1) the balance among the subsystems for voice production; (2) laryngeal muscle strength; (3) voice control and stamina; and (4) supraglottic modification of laryngeal tone. The exercises involve four steps: (1) warm-up; (2) stretching – gliding from the lowest note to the highest note; (3) contracting – gliding from the highest note to the lowest note; and (4) adductory power. The latter is achieved by sustaining five musical notes (C–D–E–F–G) for as long as possible on the vowel “o” while pursing to lips to partially occlude the vocal tract.
Unit 37.4 Voice therapy
(1) Vocal function exercises are a type of physiological voice therapy. What is the emphasis of this type of voice therapy?
(2) Stemple et al. (Reference Stemple, Glaze and Klaben2000) state that ‘when any one or more of the voice subsystems is affected by pathology, the remaining subsystems must adjust to accommodate the change of the affected part’ (331). Which of the above aims of VFE attempts to address this accommodation?
(3) Before therapy, PT had an incomplete glottal closure along the entire membranous part of the vocal fold with complete closure of the posterior glottis. How might vocal function exercises be expected to improve this glottal closure pattern?
Post-intervention vocal function
Post-therapy, PT's performance on all the vocal measurements discussed in unit 37.3 was recorded. These measurements are detailed below.
High-speed digital imaging: Voice onset time was reduced from 140 to 77 milliseconds post-therapy. The mean maximum amplitude of vibration increased from 7.8% to 10%. The open quotient post-therapy was 0.674. Open quotient calculations were not applicable for the pre-therapy recordings. The mean speed quotient was also reduced for the right vocal fold (0.90–0.48) and left vocal fold (0.58–0.53). The mean peak closing velocity, measured in glottal lengths per second, increased for both folds as the vocal folds were moving greater distances over a shorter period of time. There was a decrease in the mean peak-to-average velocity during opening and closing phases following treatment.
Stroboscopy: Pre-therapy, glottis closure had a small anterior glottal gap and a complete posterior closure. Following therapy, there was a small posterior glottal gap and improved closure of the membranous vocal folds.
Acoustic analysis: Following VFEs, there was a 26.7% increase in mean intensity level. The following measures were all within normal limits pre- and post-therapy: average fundamental frequency; jitter; low and high extent of fundamental frequency; and noise-to-harmonic ratio.
Aerodynamic analysis: Following VFEs, PT demonstrated a 4.07% increase in respiratory volume and a 54.16% decrease in mean expiratory airflow.
Perceptual assessment: Before VFEs, PT had a mean overall severity rating on the CAPE-V of 18.33/100mm (a mildly deviant voice quality). Following VFEs, the mean overall severity rating on the CAPE-V was 0/100mm (a normal voice quality).
Unit 37.5 Post-intervention vocal function
(1) Why do you think open quotient calculations were not applicable for the pre-therapy recordings?
(2) Stroboscopic findings revealed a small anterior glottal gap and complete posterior closure before treatment, and a small posterior glottal gap and improved closure of the folds following therapy. Which of the following imagesFootnote 1 corresponds to the pre-therapy description and which corresponds to the post-therapy description?

(3) Most acoustic measurements showed no change following VFEs. Moreover, these measurements were within normal limits even before treatment when PT complained of rough voice and vocal fatigue. Describe one implication of these findings.
(4) Is there any evidence that VFEs were successful in training PT how to breathe to his maximum capacity for the production of voice?
Introduction
The following exercise is a case study of a 50-year-old woman (‘Ms S’) who was studied by Sudhir et al. (Reference Sudhir, Chandra, Shivashankar and Yamini2009). This client was diagnosed with psychogenic dysphonia. Detailed case history and assessment revealed significant marital difficulties and other psychological stressors in this woman's life. The case study is presented in five sections: primer on psychogenic dysphonia; client history; voice assessment; psychological assessment; and therapeutic programme.
Primer on psychogenic dysphonia
Within the nosology of voice disorder, psychogenic dysphonia is a functional voice disorder alongside muscle tension dysphonia and voice disorders that result from phonotrauma (Connor and Bless, Reference Connor, Bless and Cummings2014). Psychogenic dysphonia is defined as the ‘loss of voice where there is insufficient structural or neurological pathology to account for the nature and severity of the dysphonia, and where loss of volitional control over phonation seems to be related to psychological processes such as anxiety, depression, conversion reaction, or personality disorder’ (Baker, Reference Baker2003: 308). An organic pathology is typically excluded as a cause of the voice disorder by means of a comprehensive laryngological examination. An equally comprehensive psychological examination is needed to reveal the complex psychological processes which may play a causative role in the onset of the voice disorder. Regardless of the triggers for psychogenic dysphonia, this voice disorder is known to have a significant adverse impact on an individual's quality of life and occupational and social functioning (Merrill et al., Reference Merrill, Anderson and Sloan2011). It is for these reasons that psychogenic dysphonia is assessed and treated by speech and language therapists among other voice professionals.
Little is known about the prevalence and incidence of psychogenic dysphonia. Kollbrunner et al. (Reference Kollbrunner, Menet and Seifert2010) reported that psychogenic aphonia, a so-called conversion disorder, is a rare condition which has a point prevalence of 0.4%. The category of functional voice disorders, to which psychogenic dysphonia belongs, is altogether more prevalent, and accounts for the majority of cases of dysphonia in many clinical samples. In a study of 882 patients attending the ENT Department at the University Hospital in Ghent, Belgium between 2004 and 2008, Van Houtte et al. (Reference Van Houtte, Van Lierde, D'haeseleer and Claeys2010) found functional voice disorders in 30% of their clinical sample. Psychogenic dysphonia is considerably more common in women than in men. Martins et al. (Reference Martins, Tavares, Ranalli, Branco and Pessin2014) examined 28 adult patients with psychogenic dysphonia, 26 of whom were women. Between February 2000 and May 2006, Kollbrunner et al. (Reference Kollbrunner, Menet and Seifert2010) identified 22 patients with psychogenic aphonia in the Department of Otorhinolaryngology, Head and Neck Surgery at Bern University Hospital. Of these patients, 19 were female. The mean ages of clients in Martins et al.'s study and Kollbrunner et al.'s investigations were 47.3 years and 40.3 years, respectively. Voice disorders are more common in certain occupational groups including teachers and professional voice users such as singers (Cantor Cutiva et al., Reference Cantor Cutiva, Vogel and Burdorf2013; Fortes et al., Reference Fortes, Imamura, Tsuji and Sennes2007). Psychogenic dysphonia is no exception in this regard, with teachers and sales clerks accounting for nine of 11 adults with psychogenic dysphonia who were in employment in Martins et al.'s study.
The onset of psychogenic dysphonia in clients is often preceded by upper respiratory tract infections and/or asthma or allergy-like symptoms. Schalén and Andersson (Reference Schalén and Andersson1992) examined 40 consecutive patients with psychogenic voice disorder. An upper respiratory tract infection prior to the onset of dysphonia was identified in 25% of patients, with as many as 40% of clients treated with antibiotics on one or more occasions. Asthma and allergy-like symptoms were reported in 37.5% of patients, a level which exceeded the incidence of asthma/allergy in the Swedish adult population. Combined with the fact that a perceptual analysis of voice profiles in psychogenic dysphonia and acute laryngitis has been shown to reveal similar aberrations (Schalén et al., Reference Schalén and Andersson1992), the presence of these other conditions can complicate a differential diagnosis of psychogenic dysphonia and lead to misdiagnosis of the voice disorder.
Unit 38.1 Primer on psychogenic dysphonia
(1) Which of the following is a true statement about psychogenic dysphonia?
Psychogenic dysphonia is a hyperfunctional voice disorder.
Psychogenic dysphonia can manifest in some cases as complete aphonia.
The vegetative functions of the larynx are compromised in psychogenic dysphonia.
Psychogenic dysphonia can arise following a stressful or traumatic event.
Vocal nodules are a common pathological finding in psychogenic dysphonia.
(2) Name three medical and health professionals who are involved in the assessment and treatment of clients with psychogenic dysphonia.
(3) In the nosology of voice disorders, psychogenic dysphonia is a functional voice disorder. Which of the following voice disorders is a functional dysphonia?
(4) Give two reasons why psychogenic dysphonia is frequently misdiagnosed.
(5) Which of the following is a true statement about the epidemiology of psychogenic dysphonia?
Psychogenic dysphonia has a similar prevalence in children and adults.
Psychogenic dysphonia is more common in women than in men.
Psychogenic dysphonia is more common in certain ethnic groups.
Psychogenic dysphonia has a peak incidence in adolescence.
Psychogenic dysphonia is a common voice disorder in the elderly population.
Client history
Ms S reported to the authors’ hospital with complaints of a hoarse voice and intermittent aphonia which had lasted 5 months. Ms S's vocal symptoms had started abruptly with fluctuations in voice quality. She reported that while she was visiting her cousins on holiday in her home country of Asian origin, there had been complete restoration of her voice. She did not experience throat pain. Her complaints included low mood, feelings of anxiety and sleeping problems. Ms S had been employed as a teaching assistant at a local school for over 10 years. Her occupational functioning had been affected by her voice problems, as she was unable to take classes. Also, much of her work had to be delegated to colleagues, as she was only able to undertake tasks that did not require her to talk for long periods of time.
Ms S is married to a business man and is a university graduate. She left her home country and migrated to a European country following her marriage. Her husband is also from her country of origin, but migrated with his family when he was an adolescent. At the time of her referral, Ms S was living with her spouse, two daughters and a son. She reported significant difficulties in her marriage to her spouse. There were frequent disagreements and anger over the children's futures and the relationship between Ms S and her mother-in-law. This was not Ms S's first attempt to seek help. She had attended several centres previously with little reported success.
Unit 38.2 Client history
(1) Which of the following statements characterise the onset of Ms S's voice disorder?
(2) Which two features of Ms S's self-report suggest that she is at risk of psychogenic dysphonia?
(3) Which aspect of Ms S's functioning is most compromised by her voice disorder?
(4) Why should an organic disorder not be rejected as a cause of Ms S's voice disorder at this stage?
Voice assessment
Ms S underwent a laryngeal examination by an otolaryngologist which revealed no organic abnormality. She reported that she used her voice for singing hymns as an amateur and for formal teaching as well as for everyday speech. Perceptual and acoustic analyses of Ms S's voice were undertaken. The GRBAS scale (Hirano, Reference Hirano1981) was used to perform a perceptual assessment. This scale assigns ratings of 0 (normal) to 3 (extreme degree of impairment) to a number of parameters: grade (G), roughness (R), breathy (B), asthenia (A) and strained (S). Ms S obtained scores of G1, R1, B0, A1, S1 during sustained phonation. On a speech task, her scores were G3, R1, B3, A3, S3. Ms S's volitional cough was good. An acoustic analysis was conducted using a speech software system. Sustained phonation of the vowel [a] had a mean habitual frequency of 220 Hz. Ms S's speaking range was from a minimum of 197.53 Hz to a maximum of 266.66 Hz. The maximum phonation duration at the mean habitual frequency was only 4 seconds. However, this was well sustained. At other frequencies – 212 Hz, 241 Hz, 271.03 Hz and 328 Hz – phonation was also well sustained, and the transition between frequencies as Ms S went up the modal register was smooth. At 359.75 Hz, the quality of the voice became strained-hoarse and Ms S was advised not to go higher in the pitch scale.
Unit 38.3 Voice assessment
(1) Which of the following procedures might an otolaryngologist use to exclude the presence of an organic laryngeal abnormality in Ms S's case?
(2) Ms S had a good volitional cough. What does this indicate?
(3) The GRBAS scale indicates that Ms S has more pronounced vocal abnormalities during a speech task than during sustained phonation. What does this suggest about the aetiology of Ms S's voice disorder?
(4) The fundamental frequency of Ms S's speaking voice ranged from 197.53 Hz to 266.66 Hz, while her mean frequency for sustained phonation of [a] was 220 Hz. Are these values within the normal range?
Psychological assessment
Ms S was assessed by a clinical psychologist. The assessment revealed that there were significant interpersonal difficulties between Ms S and her spouse and mother-in-law. Issues concerning communication patterns, decision-making in the marriage, child rearing and Ms S's ability to express her feelings and thoughts about the marriage tended to dominate. Ms S experienced feelings of alienation and distance from her spouse's family whom she perceived to be demanding. The early years of the marriage were described as difficult. Ms S felt she was criticised by her spouse over trivial matters. This caused her anxiety which led her to be somewhat disorganised in her daily activities. Her spouse was characterised as a perfectionist who was critical and demeaning about Ms S's style of functioning. In a separate interview, the spouse was found to be domineering in the relationship and particular about being on time and organised. Ms S had steadily decreased her contribution to family discussions as she had felt her ideas were criticised and dismissed as being worthless. She described how she felt ‘silenced’ by her spouse and stated that she was never ‘heard’. Both Ms S and her spouse expressed anger by not talking to each other for days. The couple did not have a healthy sexual relationship. During joint sessions with her spouse, Ms S was noted to have considerable variation in her voice. This ranged from hoarseness to aphonia, which corresponded with Ms S and her spouse having an argument.
Alongside these difficulties with her spouse Ms S had additional problems in the relationship with her mother-in-law. As the eldest son, Ms S's spouse had a duty to look after his mother. This required Ms S to spend considerable time with her spouse's family, including many family gatherings which she did not enjoy. As the eldest and only daughter-in-law of domiciliary origin, Ms S was expected to conform to family expectations and tradition, even though she and her husband now lived in a foreign culture. Ms S exhibited further anxieties about her three children growing up in western culture. Her son had failed to establish a career and had not yet moved out of the parental home. Ms S and her spouse had had several discussions about their son's career. Her daughters were both young adults. They felt restricted by their mother's expectations and value system. One of the daughters had moved to a nearby university. The other daughter had looked for a part-time job to fund herself. Ms S's children, and especially her daughters, had initially expressed concerns about her voice problems.
Three assessments of Ms S were conducted: Beck's Depression Inventory (BDI; Beck et al., Reference Beck, Ward, Mendelson, Mock and Erbaugh1961); Dysfunctional Attitudes Scale (DAS; Weissman and Beck, Reference Weissman and Beck1978); and Sentence Completion Test (SCT; Sacks and Levy, Reference Sacks, Levy, Abt and Bellak1959). The BDI is a 21-item, self-report measure of clinically derived categories of depression. Ms S obtained a score of 15 on this assessment, indicating the presence of depression of mild severity. The DAS is a 40-item, self-report measure which assesses an individual's attitudes across several domains. Ms S displayed problems in the approval–rejection domain of DAS and imperative assumptions. She had difficulty endorsing items on autonomy. She endorsed views that others did not like her if they disagreed with her, and that she was worthless if someone she loved did not reciprocate. Ms S's responses on the SCT indicated significant difficulties in the area of marriage and heterosexual relations. However, she recalled a happy childhood.
Unit 38.4 Psychological assessment
(1) Issues around speaking out and having one's voice heard are often revealed in a psychological assessment of the client with psychogenic dysphonia. Is that true of the present case?
(2) Communication is a dominant theme in Ms S's personal psychology. But there is another way in which communication issues manifest themselves in the present case. What is that way?
(3) Are fluctuations in Ms S's vocal symptoms reflective of her emotional state? Provide support for your answer.
(4) Primary and secondary gains are thought to play an important role in maintaining and reinforcing certain psychogenic voice disorders (Roy, Reference Roy and Kent2004: 28). A primary gain describes the avoidance of anxiety that is made possible when a psychological conflict does not enter one's conscious awareness. A secondary gain is the avoidance of an undesirable responsibility or activity and the extra attention that is conferred on the patient who has a voice disorder. Is there any secondary gain for Ms S in having a voice disorder?
(5) Clearly, a psychological assessment of the voice client is only of clinical value to the extent that its findings can be successfully addressed in therapy. Is there any evidence that a combined treatment involving speech therapy and psychotherapy is more effective than speech therapy alone?
Therapeutic programme
Ms S received a programme of therapy which was jointly delivered by a clinical psychologist and speech pathologist. During a three-week period, Ms S received a total of 15 sessions of cognitive behavioural therapy. These sessions attempted to restore voice and improve the client's ability to cope with emotional problems. The possible meaning of Ms S's symptoms was addressed in the sessions. To assist Ms S in reducing the physiological arousal that was related to her anger and anxiety, and associated sleep problems, training in deep muscle relaxation was adopted. Dysfunctional assumptions were identified and clarified through Socratic questioning with the aim of cognitively restructuring them. Negative cognitions in the domains of Ms S's children's future and her relationship to her spouse and his family were the focus of sessions. Ms S was encouraged to adopt more neutral alternative interpretations during interactions. Sessions also aimed to increase Ms S's problem-solving skills, decision-making and organisation of tasks. During sessions with the couple, tasks and goals were identified which were intended to help improve communication and resolve conflicts about child rearing and sexual interactions. The critical attitudes and expectations of Ms S's spouse were addressed in these sessions, although he appeared reluctant to modify them.
In each session of voice therapy, Ms S received direct voice therapy and counselling. Direct therapy began with the non-phonatory task of cough which was immediately followed by sustained production of [a]. From cough and phonation, Ms S progressed to phonation with soft contact. Gradually, phonation was extended to other speech sounds (e.g. [u] and [i]). Reassurance and encouragement was provided to maintain a good quality of voice production. Other tasks included sustained humming and the matching of pitch patterns. During counselling the abuse of Ms S's voice in the context of her family problems were subjected to psychotherapeutic examination. Efforts were made to reduce her psychosocial stress. Vocal hygiene and the effects of voice misuse were also addressed. When Ms S could sustain voice for a longer duration in the clinic, she was encouraged to generate words from lexical categories in a prolonged manner. She was eventually able to engage in sustained conversation for a period of 15 minutes. After approximately six 1-hour sessions Ms S was able to sustain voicing even in the presence of her spouse. Although Ms S experienced intermittent dysphonia during this period, she was able to regain her voice with humming and she was encouraged to sing hymns as she had done previously. After sustained voice was achieved over several days, voice therapy was terminated. By this stage, Ms S had a mean habitual frequency for [a] of 207.79 Hz. Her GRBAS scale scores were zero across all parameters.
Unit 38.5 Therapeutic programme
(1) Ms S received cognitive behavioural therapy (CBT). Which of the following are true statements about CBT as applied to clients with dysphonia?
CBT is the only psychological intervention used by voice therapists.
Stress management is a part of CBT for clients with dysphonia.
CBT is most effective in the absence of voice therapy.
CBT is only used when dysphonia has persisted for six months.
Assertiveness training is a part of CBT for clients with dysphonia.
(2) During direct voice therapy Ms S progressed to using phonation with soft contact. Explain what ‘soft contact’ means in this context.
(3) Vocal hygiene was addressed during Ms S's treatment. Describe some of the issues which are brought to the client's awareness during a discussion of vocal hygiene.
(4) Ms S was also educated about voice misuse. Why are clients with psychogenic dysphonia at risk of voice misuse?
Introduction
The following exercise is a case study of a man (‘MT’) who was studied by Burkart et al. (Reference Burkart, Senchenkov, Wilson and Pensak2010). MT presented with a late-stage supraglottic carcinoma. He was treated with open supraglottic laryngectomy and postoperative radiation therapy. The case study is presented in five sections: primer on laryngeal carcinoma; client history; medical evaluation and diagnosis; medical and surgical management; focus on post-laryngectomy communication.
Primer on laryngeal carcinoma
Laryngeal cancer is a life-threatening disease which also causes significant disability in the individuals who develop it. The epidemiology of laryngeal cancer is monitored through the Surveillance, Epidemiology, and End Results (SEER) Program of the National Cancer Institute in the United States. According to SEER statistics, there were an estimated 88,852 people living with laryngeal cancer in the US in 2012. There were 13,560 estimated new cases in 2015 and 3,640 deaths in the same year. Between 2008 and 2012, most new laryngeal cancers (31.2%) occurred in the age group 55 to 64 years (National Cancer Institute, 2015). Historically, more men than women have developed laryngeal cancer. This is still the case today. However, there is evidence that women are representing an increasing proportion of cases over time (Brandstorp-Boesen et al., Reference Brandstorp-Boesen, Falk, Boysen and Brøndbo2014). MacNeil et al. (Reference MacNeil, Liu, Shariff, Thind, Winquist, Yoo, Nichols, Fung, Hall and Garg2015) reported a five-year survival rate of 57.4% in a study of 4,298 patients who were diagnosed with laryngeal cancer in Ontario between 1995 and 2007. This was lower still (45.4%) for laryngectomy-free survival. This study also showed that overall and laryngectomy-free survival had remained unchanged since the mid-1990s.
Laryngeal carcinoma has a multifactorial aetiology. Among the factors linked to the development of the disease are smoking and alcohol consumption, gastroesophageal reflux disease (GERD), immunosuppression (in HIV/AIDS and transplant recipients), infection with human papillomavirus and helicobacter pylori, and a history of head and neck cancer in first-degree relatives. Laskaris et al. (Reference Laskaris, Sengas, Maragoudakis, Tsimplaki, Argyri, Manolopoulos and Panotopoulou2014) examined HPV infection in 54 patients with squamous cell carcinoma of the larynx. HPV DNA was present in 18.5% (10/54) laryngeal squamous cell carcinomas. HPV 16, which was the most common type, was detected in 7.5% of patients. Zhang et al. (Reference Zhang, Zhou, Chen, Zhou and Tao2014) conducted a systematic review of studies published up to November 2013 that examined the prevalence of GERD in laryngeal or pharyngeal cancer. In a meta-analysis of 10 studies, GERD was found to be significantly associated with laryngeal cancer, but not pharyngeal carcinoma. Piselli et al. (Reference Piselli, Burra, Lauro, Baccarani, Ettorre, Vizzini, Rendina, Rossi, Tisone, Zamboni, Bortoluzzi, Pinna, Risaliti, Galatioto, Vennarecci, Di Leo, Nudo, Sforza, Fantola, Cimaglia, Verdirosi, Virdone and Serraino2015) reported a particularly elevated standardised incidence ratio for cancer of the larynx in liver transplant recipients with alcoholic liver disease.
Treatment for laryngeal cancer involves surgery, radiotherapy and chemotherapy. Today, protocols emphasise organ- and function-preserving interventions as a primary treatment method. When a laryngectomy is performed, it is often undertaken as a salvage procedure when radiation or chemoradiation has failed. The result has been a decrease in the number of laryngectomies that are performed (Grau et al., Reference Grau, Johansen, Hansen, Andersen, Godballe, Andersen, Hald, Møller, Overgaard, Bastholt, Greisen, Harbo, Hansen and Overgaard2003). When surgery is adopted as the primary modality, conservative procedures (partial laryngectomy) are pursued whenever possible. The choice of total versus partial laryngectomy as well as type of partial laryngectomy is determined by a range of factors including the location of a tumour. For example, a supraglottic laryngectomy is performed if there is a tumour of the false vocal fold. However, if a supraglottic lesion extends to the glottis, a supracricoid laryngectomy is performed. These procedures have different implications for voice and swallowing function. A supraglottic laryngectomy can leave an individual with relatively good voice quality but often causes serious swallowing difficulties. When a carcinoma of the tongue or oesophagus invades laryngeal tissues, the larynx may also need to be removed. In this case, laryngectomy is performed alongside glossectomy or oesophagectomy.
Unit 39.1 Primer on laryngeal carcinoma
(1) The epidemiology of laryngeal cancer has revealed that women are representing an increasing proportion of cases over time. Why do you think this is the case?
(2) The subjects studied by Piselli et al. (Reference Piselli, Burra, Lauro, Baccarani, Ettorre, Vizzini, Rendina, Rossi, Tisone, Zamboni, Bortoluzzi, Pinna, Risaliti, Galatioto, Vennarecci, Di Leo, Nudo, Sforza, Fantola, Cimaglia, Verdirosi, Virdone and Serraino2015) had a particularly elevated standardised incidence ratio for cancer of the larynx. Which two risk factors for laryngeal cancer do these subjects exhibit?
(3) Gastroesophageal reflux disease (GERD) is now recognised as a significant risk factor for laryngeal cancer. Explain how GERD is associated with the development of laryngeal cancer.
(4) Which of the following procedures may be used to treat a tumour of the epiglottis and false vocal folds?
(5) Respond with true or false to each of the following statements about swallowing after laryngectomy:
Aspiration is a significant risk after total laryngectomy.
There is a high incidence of dysphagia after supracricoid laryngectomy.
Videofluoroscopy can be used to evaluate swallowing after laryngectomy.
Dysphagia normally resolves within 6 months after laryngectomy.
Manometry can be used to evaluate swallowing after laryngectomy.
Client history
MT is a 62-year-old man who is a construction worker. He presented for assessment because of hoarseness which had lasted for three months. He reported mild dysphagia and odynophagia. He exhibited no weight loss or otalgia and is otherwise healthy. MT has smoked one pack of cigarettes per day for 40 years and has consumed alcohol socially.
Unit 39.2 Client history
(1) MT conforms to the demographic profile of individuals who are most likely to develop laryngeal cancer. In what two respects is this the case?
(2) Which two lifestyle risk factors for laryngeal cancer does MT have?
(3) MT presented for assessment on account of persistent hoarseness. Depending on the location of a laryngeal tumour, hoarseness can be an early symptom of disease or a sign of a more advanced tumour. Explain.
(4) Among the symptoms that MT exhibited were odynophagia and otalgia. Describe these symptoms.
(5) Apart from the symptoms described above, list three other symptoms associated with laryngeal cancer.
Medical evaluation and diagnosis
MT underwent an extensive medical evaluation. His larynx was mobile on physical examination. Flexible fibreoptic laryngoscopy was performed. It revealed a friable, ulcerated mass on the laryngeal surface of the infrahyoid epiglottis and the left false vocal fold. The true vocal folds were crisp and appeared to be clear of tumour. There was no involvement of the anterior and posterior commissures and the arytenoids. The right vocal fold was fully mobile and was effectively compensating for mildly impaired mobility of the left vocal fold. MT had a left, firm, palpable, enlarged, upper jugular node which was less than 3 cm in diameter. There were no other signs of adenopathy or other masses in the head and neck region on examination. MT had poor dentition.
Other medical investigations were performed. MT had a CT scan of the head and neck. This revealed a 2.5 × 2.3 × 1.9 cm left supraglottic tumour that involved the epiglottis and left false vocal fold but not the laryngeal cartilages. The scan also showed a single 2.5 cm ipsilateral level 2 lymph node with central necrosis but no other adenopathy. Panendoscopy was performed and revealed no second primary tumour. The base of the tongue had normal consistency during bimanual palpation. There was fullness in the pre-epiglottic space. The laryngeal tumour biopsy that was performed during direct laryngoscopy revealed a moderately differentiated keratinising squamous cell carcinoma. Squamous cell carcinoma clusters were obtained from a fine-needle aspiration of the cervical lymph node. A chest radiograph was negative for metastatic foci. On the basis of these investigations, a diagnosis was made: MT had a stage III (T2N1M0) squamous cell carcinoma of the supraglottic larynx.
Unit 39.3 Medical evaluation and diagnosis
(1) During a visual examination of the larynx, MT's tumour was found to involve certain laryngeal structures while other structures appeared to be free of disease. The diagram below is a coronal section of the larynx viewed from the back. Place an X on the structures that are compromised by MT's tumour.

(2) What type of laryngectomy is warranted in MT's case? Provide support for your answer. Is any additional surgical procedure necessary?
(3) What significance does the poor condition of MT's dentition have for any post-surgical rehabilitation?
(4) One of the medical investigations that were undertaken was a panendoscopy. What is panendoscopy? Give two reasons why this procedure is performed.
Medical and surgical management
MT was treated with open supraglottic laryngectomy. He also underwent left modified radical neck dissection and right selective neck dissection. The neck specimen revealed extracapsular spread, for which MT received postoperative radiation therapy.
Unit 39.4 Medical and surgical management
(1) MT was treated with open supraglottic laryngectomy. Which aspect of this client's post-surgical rehabilitation will be of most concern to the speech-language pathologist?
(2) Which of the following stages of swallowing is most compromised in clients with supraglottic laryngectomy? oral preparatory; oral propulsive; pharyngeal; oesophageal. Explain why the stage you have selected is most compromised.
(3) Which other aspect of MT's management is likely to contribute to any swallowing problems?
(4) MT was treated with an open supraglottic laryngectomy. What other type of supraglottic laryngectomy can be performed? Do these different procedures have the same voice and swallowing outcomes?
(5) Which histological finding is a poor prognostic indicator for MT?
Focus on post-laryngectomy communication
MT underwent an open supraglottic laryngectomy in which his vocal function was preserved. Such a procedure can establish safe short-term swallow function. However, clients who have a partial laryngectomy may subsequently require completion laryngectomy because of late dysphagia and chronic aspiration (Bagwell et al., Reference Bagwell, Leder and Sasaki2015). After completion laryngectomy, clients face a new challenge of alaryngeal communication. In this unit, different methods of post-laryngectomy voice production will be examined. These methods are as relevant to clients who require completion laryngectomy as they are to clients who have total laryngectomy as a primary treatment modality.
The three methods of communication that are available to clients after total laryngectomy are (i) the use of an artificial or electronic larynx, (ii) the use of oesophageal voice and (iii) the use of a tracheoesophageal voice prosthesis. There are different types of commercially available artificial or electronic larynxes. The electronic neck-type and electronic mouth-type artificial larynxes are the most common of these devices (Benninger et al., Reference Benninger, Grywalski, Phyland, Johnson and Jacobson2007). In the neck-type device, a battery-produced sound is conducted through the neck into the oral cavity where the articulators proceed to produce speech sounds as normal. The head of the device is placed against the neck. For effective sound conduction to occur, neck tissue must be supple. Post-operative swelling of the neck tissue and changes to neck tissue related to radiotherapy may make this device difficult to use initially. In the electronic mouth-type device, battery produced sound is carried via a mouth tube into the oral cavity. Because these devices produce continuous sound at the push of a button, clients must be taught strategies for normal phrasing and dealing with the inability to produce contrasts between voiced and voiceless sounds (Benninger et al., Reference Benninger, Grywalski, Phyland, Johnson and Jacobson2007). An electronic neck-type device is shown in Figure 39.1.
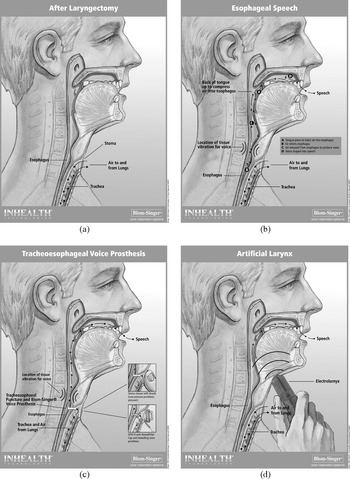
Figure 39.1(a)–(d) Diagrams showing: (a) anatomical structures after laryngectomy and various methods of alaryngeal communication; (b) oesophageal voice; (c) tracheoesophageal voice prosthesis; (d) artificial larynx.
In the second method of alaryngeal communication after laryngectomy – oesophageal voice production – air is either inhaled or injected into the hypopharynx. The inhaled or injected air is then quickly expelled through the pharyngoesophageal (PE) segment, a narrow sphincter of muscle fibres at the juncture of the hypopharynx and the oesophagus (Benninger et al., Reference Benninger, Grywalski, Phyland, Johnson and Jacobson2007). Because this method only has access to air in the hypopharynx, there are reduced air volumes for speech. Accordingly, oesophageal voice users need to frequently insufflate the PE segment during continuous speech. In rehabilitation, clients can be taught different methods of optimal air intake and how to achieve appropriate phrase lengths during speech. They can also be advised on how to avoid stoma and air injection noise (Benninger et al., Reference Benninger, Grywalski, Phyland, Johnson and Jacobson2007). The quality of oesophageal voice is associated with the vibratory function of the PE segment. Van Weissenbruch et al. (Reference Van Lierde, Van Borsel and Van Cauwenberge2000) found that hypertonicity, spasm, strictures, and hypotonicity of the PE segment were correlated significantly with poor or moderate alaryngeal speech in 60 post-laryngectomy patients. The use of oesophageal voice is also illustrated in Figure 39.1.
The third method of alaryngeal communication is the use of a tracheoesophageal voice prosthesis (TEVP). TEVP has become the gold standard in the management of clients who undergo total laryngectomy (Kapila et al., Reference Kapila, Deore, Palav, Kazi, Shah and Jagade2011). A fistula is surgically created in the common wall of the posterior trachea and the anterior oesophagus. A voice prosthesis is fitted into this fistula, with the proximal end in the stoma and the distal end in the lumen of the oesophagus (Benninger et al., Reference Benninger, Grywalski, Phyland, Johnson and Jacobson2007). The prosthesis is a one-way valve. As such, it permits air to enter the oesophagus but prevents food and secretions in the oesophagus from entering the trachea. When the stoma is manually occluded, pulmonary air is directed through the valve into the oesophagus where it travels superiorly to vibrate the PE segment. An adjustable tracheostoma valve obviates the need to manually block the stoma. A TEVP may be fitted at the time that a total laryngectomy is performed (primary TE puncture). Alternatively, it may be fitted some weeks after total laryngectomy (secondary TE puncture). Because a pulmonary airstream is used to vibrate the PE segment in this form of alaryngeal communication, it is easier for clients to produce continuous speech using a TEVP than standard oesophageal voice. The use of a TEVP is also illustrated in Figure 39.1.
Unit 39.5 Focus on post-laryngectomy communication
(1) Respond with true or false to each of the following statements about alaryngeal communication:
Blom-Singer is one type of voice prosthesis.
Clients can use more than one method of alaryngeal communication.
There are four different methods of oesophageal insufflation.
Voice prostheses cannot prevent aspiration into the airway.
Irradiated tissue presents challenges for alaryngeal communication.
(2) Effective alaryngeal communication is integral to the quality of life of clients who have a laryngectomy. Describe three ways in which alaryngeal communication can contribute to quality of life in laryngectomy clients.
(3) All three methods of alaryngeal communication have drawbacks as well as advantages. Five of these drawbacks are listed below. Identify the form of alaryngeal communication to which each of these drawbacks relates:
Volume and pitch alterations can be achieved but are compromised.
Regular equipment maintenance is required.
A limited air source results in reduced continuous speech.
Management of secretions is required.
Enlargement of the tracheoesophageal puncture can occur along with periprosthetic leakage.
(4) The use of external beam radiation therapy and chemotherapy to treat upper aerodigestive tract malignancy can result in radiation-induced pharyngoesophageal stenosis (Urben et al., Reference Urben, Jacobson and Lazarus2012). Which method(s) of alaryngeal communication are compromised by PE stenosis? What other function is compromised by PE stenosis?
Introduction
The following exercise is a case study of a male-to-female transgender adolescent (‘LA’) aged 15 years who was studied by Hancock and Helenius (Reference Hancock and Helenius2012). LA was diagnosed at 14 years of age with gender dysphoria by a neuropsychologist. The case study is presented in five sections: primer on gender dysphoria and transsexual voice; client history; voice evaluation; voice and communication therapy; and communication outcomes.
Primer on gender dysphoria and transsexual voice
The Royal College of Psychiatrists (2013) states that ‘[g]ender dysphoria is the distress associated with the experience of one's personal gender identity being inconsistent with the phenotype or the gender role typically associated with that phenotype’ (12). Several recent epidemiological studies have estimated the prevalence of gender dysphoria in a number of European countries. Judge et al. (Reference Judge, O'Donovan, Callaghan, Gaoatswe and O'Shea2014) estimated the prevalence of gender dysphoria in the Irish population to be 1:10,154 (male:female) and 1:27,668 (female:male). Kuyper and Wijsen (Reference Kuyper and Wijsen2014) used three measures to estimate the prevalence of gender dysphoria in the Dutch population. The measures were gender identity, dislike of the natal female/male body, and wish to obtain hormones/sex reassignment surgery. These measures combined resulted in figures of 0.6% and 0.2% for the prevalence of gender dysphoria in males and females, respectively. De Cuypere et al. (Reference De Cuypere, Van Hemelrijck, Michel, Carael, Heylens, Rubens, Hoebeke and Monstney2007) reported an overall prevalence of 1:12,900 for male-to-female transsexuals and 1:33,800 for female-to-male transsexuals in Belgium. These investigators calculated the male:female sex ratio in the total Belgian population to be 2.43:1.
Management of the transsexual client by speech-language pathologists has focused for the most part on the assessment and treatment of voice. The pitch of the speaking voice is the main area of concern, particularly for male-to-female transsexuals. However, there is increasing recognition that areas such as resonance and articulation also make an important contribution to the perception of the speaker as female (Dacakis et al., Reference Dacakis, Oates and Douglas2012). In male-to-female transsexuals, voice therapy is the primary means of achieving pitch elevation, with a range of surgical procedures offered if the client's desired voice quality is not achieved. These procedures work by altering one of the physiological parameters that are known to control pitch: vocal fold tension, length and mass (Anderson, Reference Anderson2014). The vocal attributes of female-to-male transsexuals is still a relatively under-investigated area (Azul, Reference Azul2015). This is despite the fact that pitch-lowering difficulties have been identified in approximately 10% of female-to-male transsexuals (Cosyns et al., Reference Cosyns, Van Borsel, Wierckx, Dedecker, Van de Peer, Daelman, Laenen and T'Sjoen2014). One reason for this neglect is the mistaken assumption that testosterone-induced voice changes are sufficient in themselves to achieve the type of vocal result that female-to-male transsexuals desire.
Unit 40.1 Primer on gender dysphoria and transsexual voice
(1) It is difficult for epidemiological studies to obtain accurate estimates of the prevalence of gender dysphoria. Some of these studies have based their findings on the number of individuals attending gender clinics (e.g. Judge et al., Reference Judge, O'Donovan, Callaghan, Gaoatswe and O'Shea2014). Are these studies likely to be overestimating or underestimating the true prevalence of gender dysphoria in the general population? Provide support for your answer.
(2) Respond with true or false to each of the following statements about gender dysphoria:
‘Gender dysphoria’ is a diagnostic term in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
A diagnosis of gender dysphoria is made by speech-language pathologists.
The individual with gender dysphoria must experience clinically significant distress.
Speech-language pathologists are an integral part of the multidisciplinary team which assesses and treats clients with gender dysphoria.
Typically, there is no impairment in social, occupational or other areas of functioning in clients with gender dysphoria.
(3) Pitch elevation is the primary aim of voice therapy in male-to-female transsexuals. Which physical attribute of the speaking voice must be modified in order to make pitch elevation possible?
(5) For a number of female-to-male transsexuals, pitch-lowering poses significant difficulties. Which of the following factors best explains these difficulties?
Pitch-lowering difficulties are the result of poor compliance on the part of clients with voice therapy techniques.
Pitch-lowering difficulties are the result of diminished androgen sensitivity on the part of some female-to-male transsexual clients.
Pitch-lowering difficulties are the result of low frequency voice therapy.
Pitch-lowering difficulties are related to structural anomalies of the larynx.
Pitch-lowering difficulties are related to the use of inappropriate behavioural techniques in voice therapy.
Client history
LA is a healthy teenager with an unremarkable medical history. She is 5 feet 9 inches tall and weighs 140 lbs. English is her first language and she speaks Standard American English dialect. LA has had no prior contact with speech-language pathology.
A neuropsychologist diagnosed LA with gender dysphoria at 14 years of age. LA first told her friends that she was a girl followed by her family. She then began a month-long transition from living as a male to living as a female. At first, she presented as gender-neutral at school and as female at home. After one month, when school had ended, she presented as female 100% of the time. Two months after beginning to live as female, LA started hormone therapy (1mg oestradiol and 15mg spironolactone, each twice daily). At this stage, she was post-puberty, Tanner Stage 4.
At 15;3 years of age, LA started voice and communication therapy. LA's clinical social worker referred her for voice assessment and voice feminisation therapy to the Speech and Hearing Center at George Washington University. According to LA, her voice embarrassed her, made her feel less feminine, and got in the way of her living as a female. At her initial voice evaluation, LA estimated that she used her male birth voice approximately 85% of the time even though she was living as female 100% of the time. The remaining 15% of the time, LA used what she described as a ‘higher-pitched female voice’. LA's ability to pass as female on the phone was assessed by clinicians to be approximately 50%, while the ability to pass as female in face-to-face interaction was approximately 70%. LA reported no significant abusive vocal behaviours, and did not have a history of acid reflux or alcohol and tobacco use.
LA was well supported by family members and friends. A member of her family always accompanied her to weekly voice therapy sessions. LA also received the full support of her high school. Despite this, she chose to be home schooled for the autumn semester in her tenth grade year, and also for half of her courses in the spring semester of the same year.
Unit 40.2 Client history
(1) LA's hormone therapy included oestradiol (an oestrogen) and spironolactone (an anti-androgen). Respond with true or false to each of the following statements about the effect of hormone therapies on the voice in transsexual clients:
Oestrogen and anti-androgen therapy cannot reverse pubertal changes in the voice in the male-to-female transsexuals.
Laryngeal tissues are largely insensitive to androgen therapy.
Androgen therapy in female-to-male transsexuals causes the vocal folds to become thicker and heavier.
Laryngeal tissues are more sensitive to oestrogen therapy than other tissues in the body.
Androgen therapy can achieve acceptable pitch-lowering in most female-to-male transsexuals.
(2) LA is at Tanner Stage 4 in pubertal maturation. What is the significance of this stage for the characteristics of the voice?
(3) How would you characterise LA's voice-related quality of life at the point of referral to a university voice clinic?
(4) What evidence is there that the auditory–perceptual characteristics of LA's voice resulted in listener misidentification of her gender?
(5) LA reported no significant abusive vocal behaviours, and did not have a history of acid reflux or alcohol and tobacco use. Why is it important for LA's voice clinicians to know about abusive vocal behaviours on the one hand, and acid reflux and alcohol and tobacco use on the other hand?
Voice evaluation
LA's voice was evaluated on a weekly basis prior to a therapy session. Visi-PitchTM software was used to analyse her voice during three speech tasks – reading, picture description and monologue. She received instructions to speak at a comfortable volume and pitch into a microphone that was placed approximately 4 inches in front of her mouth. Several acoustic measures were recorded for each speech task in order to chart LA's progress in therapy. These measures included: total frequency range; mean speaking fundamental frequency; minimum and maximum speaking frequencies with range in Hertz and semitones; and loudness in decibels. LA's speaking rate, calculated as the number of words produced per minute, was also recorded on a weekly basis.
Unit 40.3 Voice evaluation
(1) Visi-Pitch software was used to analyse LA's voice. Which of the following are true statements about this software?
Voice parameters are displayed in real-time to help clients achieve therapy goals with visual feedback.
Visi-Pitch is only suitable for use with clients who have voice disorders.
Split screens allow a client's attempts to be compared to a target vocalisation along a number of parameters.
Visi-Pitch can be used to display fundamental frequency, amplitude and spectral characteristics.
Visi-Pitch can provide clients with auditory feedback.
(2) LA's voice was assessed during three different speech tasks: reading, picture description and monologue. Why is it important to include different speech tasks in a voice assessment?
(3) Mean speaking fundamental frequency was one of the acoustic measures recorded during LA's voice assessment. Why is fundamental frequency an important measure to record in LA's case?
(4) The mean fundamental frequency of the male speaking voice is 125 Hz (range 107–146 Hz), while the mean fundamental frequency of the female speaking voice is 212 Hz (range 197–227 Hz).Footnote 1 For the male-to-female transsexual to be perceived as female, the fundamental frequency of the speaking voice must approximate that of natal females. Which of the following figures reflects the minimum speaking fundamental frequency that must be achieved by the male-to-female transsexual in order to be perceived as female?
Voice and communication therapy
Over a period of seven months, LA received a total of 15 sessions of voice therapy. Therapy was conducted by a certified speech-language pathologist with expertise in transgender communication and a master's-level speech-language pathology student clinician. There were a number of elements to LA's therapy. These included education, posture, relaxation and breathing; oral resonance; intonation; pitch; voice quality; and rate. Generalisation and stabilisation were also addressed in therapy. These various components are addressed below.
Education, posture, relaxation and breathing: During education and counselling, LA was informed about abusive vocal behaviours. Anatomy and physiology of voice production were also described and the goals and objectives of therapy were discussed. LA was instructed in how to achieve aligned and relaxed posture. Mind and body meditation were used during relaxation and were followed by neck stretches and shoulder rolls. A weekly massage of the suprahyoid space and laryngeal musculature was performed by the clinician. The clinician also modelled and explained diaphragmatic–abdominal breathing.
Oral resonance: Feminine oral resonance was modelled by the clinician. LA was encouraged to feel the ‘buzz’ that was created by resonance in her oral cavity and to project her voice to the back of the room using a smooth, full sound. A resonant sound was attempted first at a single-sound utterance level (i.e. sustained /ah/, gradual increase in volume on /ah/, gradual increase in pitch on /ah/). This same technique was then implemented on single words, and longer and more complex utterances until resonance could be achieved in connected speech.
Intonation: Female and male intonation patterns were compared. The clinician modelled female intonation. Female intonation was first used by LA in single words, then longer and more complex utterances and eventually in connected speech.
Pitch: When more efficient breathing, resonance, relaxation and intonation had been achieved by LA, attention turned to the fundamental frequency of her voice. A speech sample which had been recorded at the beginning of the session was played to LA. The Visi-Pitch program display was used to show LA the acoustic measure of fundamental frequency. LA was then encouraged to read brief sentences at a pitch which was slightly higher than the one she had just heard. Acoustic measures were again shown to LA. Through the use of auditory and visual feedback, LA was able to gauge whether her vocal adjustments were successful.
Voice quality: LA's female voice had a breathy quality that was ‘wispy’ or weak especially as pitch increased. She was instructed in how to produce a ‘soft, gentle’ voice that was strong rather than weak. A feminine vocal quality was achieved after one treatment session.
Rate: At the beginning of therapy, LA's speaking rate when reading the Rainbow Passage was approximately 260–80 words per minute (wpm). LA was able to gradually decrease her speaking rate to 190–200 wpm by means of her clinician giving her a verbal cue to ‘slow’ and using a gesture of slow arm movement as in conducting an orchestra.
Generalisation and stabilisation: LA was encouraged to use her new voice in more challenging situations such as asking strangers for directions and ordering quickly in a fast food line. When speaking to her parents and brother, some aspects of LA's new voice lapsed. For example, she spoke with a lower pitch and increased rate to her brother than when she was with the clinician. Around the university campus she simulated more challenging situations with the clinician. Follow-up at two months revealed that LA was pleased with her voice and communication. Her new voice no longer required her conscious attention in order to be used.
Unit 40.4 Voice and communication therapy
(1) During therapy the use of diaphragmatic–abdominal breathing was encouraged. This type of breathing provides optimal respiratory support for voice production. Which respiratory pattern will LA's clinician be aiming to avoid?
(2) Oral resonance was targeted during LA's voice therapy. Can modifications of oral resonance in male-to-female transsexuals increase perception of the speaker as female? Provide evidence to support your answer.
(3) Intonation was also considered to be an important aspect of LA's voice feminisation. Respond with true or false to each of the following statements about intonation in male-to-female transsexuals:
Male-to-female transsexuals who are not perceived as female use less upward and more downward intonations than those who pass as female.
Intonation does not influence gender perception in male-to-female transsexuals.
Male-to-female transsexuals who are not perceived as female use more upward and less downward intonations than those who pass as female.
Intonation in male-to-female transsexuals is resistant to therapeutic intervention.
Intonation makes a less significant contribution to gender perception in male-to-female transsexuals than speaking fundamental frequency and resonance.
(4) In a retrospective chart review of 25 male-to-female transsexuals, Hancock and Garabedian (Reference Hancock and Garabedian2013) reported that 28% presented with a voice disorder that was separate from gender presentation concerns. Why are these clients at an increased risk of voice disorder? Which aspect of LA's intervention is intended to reduce this risk?
(5) Palmer et al. (Reference Palmer, Dietsch and Searl2012) found that male-to-female transsexuals who reported passing as females had incomplete glottal closure (a posterior glottal gap) and phase closure ratios which were skewed towards more open time. Which aspect of LA's voice quality might be explained by these endoscopic and stroboscopic findings?
Communication outcomes
LA reported a positive change in attitude and self-perception following therapy. She completed the Transgender Self-Evaluation Questionnaire (TSEQ; Dacakis, Reference Dacakis, Adler, Hirsch and Mordaunt2006) at three points in time. At her initial evaluation, LA scored 106/120 on the TSEQ, which indicated that her voice negatively affected her life to a severe degree. Six months later, her score had dropped to 79/120 (moderate degree). Four months later – two months after therapy had been terminated – LA scored 53/120.
The Consensus Auditory–Perceptual Evaluation of Voice (CAPE-V; American Speech-Language-Hearing Association, 2002) was used to describe the auditory–perceptual attributes of LA's voice before and after therapy. At initial evaluation, roughness, strain and loudness were judged to be within normal limits. Breathiness was mild and pitch was assessed to be mildly low. It was also observed at initial evaluation that LA used imprecise articulation, had a voice tone that resonated in the laryngeal area rather than forward in the oral cavity, displayed limited intonation and had an excessive speech rate (282 wpm). LA's posture was mildly slouched and she used thoracic breathing. There was also mild suprahyoid and laryngeal tension. After eight therapy sessions, LA's mild breathiness and low pitch had improved. Also, LA had forward-focused resonance in the oral cavity, demonstrated relaxed and aligned posture, and used diaphragmatic–abdominal breathing at follow-up two months after the termination of treatment.
At the initial evaluation, LA's male voice during monologue had a mean speaking fundamental frequency of 136 Hz. During production of a sustained vowel, perturbation measures for her male voice were within normal limits. The speaking fundamental frequency of LA's female voice was 151 Hz during conversation, 141 Hz during picture description and 158 Hz when reading. LA's female voice was excessively breathy and sounded unnatural. Shimmer (%) values were high, but noise-to-harmonic ratio values were not excessive. At discharge, LA's mean fundamental frequency was near 200 Hz when reading or describing a picture and was 172 Hz during monologue. Stable pitch levels near 200 Hz for sustained /a/, reading and picture description were maintained at two-month follow-up. Pitch during monologue was slightly lower at 169 Hz. Jitter was above normal limits at follow-up. The total range of frequency had reduced from discharge but was still within normal limits at 30 semitones.
LA's resonance was assessed during treatment. The first formants (F1) and second formants (F2) of the four corner vowels in /hVd/ context were measured. These formants correspond to tongue height and tongue fronting, respectively. F1 and F2 values are higher in females because of the different sizes of the male and female vocal tracts, and the more open oral cavity and anterior oral resonance in females. With the exception of the back vowel /u/, LA's formant frequencies moved towards average female values during treatment. LA's speaking rate gradually decreased to near 200 wpm. Listener perceptions of LA's voice were also recorded. For picture description and monologue, ratings of femininity increased from 27 to 79 (a 192% increase) and from 31 to 72 (a 132% increase), respectively. Ratings of the softness of LA's voice displayed similar increases. These ratings were stable two months after discharge.
Unit 40.5 Communication outcomes
(1) Voice therapy in male-to-female transsexuals is judged to be effective if it achieves an improvement in the voice-related quality of life of these clients. How would you characterise the effectiveness of the therapy that LA has received?
(2) Before therapy, LA displayed mild suprahyoid and laryngeal tension which improved after treatment. What type of voice disorder might LA have been at risk of developing if this tension had been allowed to persist?
(3) At initial evaluation, LA's female voice was perceived to be mildly breathy. However, after eight therapy sessions, her breathiness had improved. Which acoustic measure confirms the impression of breathiness?
(4) At discharge, LA's mean fundamental frequency was near 200 Hz when reading or describing a picture. How would you characterise LA's mean fundamental frequency upon completion of treatment?

