Previous research has implicated herpes simplex virus 1 (HSV1) and cytomegalovirus (CMV) in severe mental illness (SMI) with conflicting results. Both pathogens have high universal seroprevalence, are neurotropic and after the primary infection typically establish a persistent latent infection with periodic reactivations. Increased immunoglobin G (IgG) concentrations are considered to be attributable to an increased infection severity with more frequent reactivations or host immune system alterations.
We assessed the HSV1 and CMV IgG concentrations in previously infected (seropositive) patients with SMI and healthy controls (HC). We hypothesized that seropositive patients would show higher IgG concentrations than seropositive HC.
We included 765 patients, 515 with schizophrenia (SZ) and 250 with bipolar disorder (BP), and 541 HC. HSV1 and CMV IgG seropositivity and concentrations were measured with immunoassays. 355 patients, mean age 33 years, 45% females, and 238 HC, mean age 35 years, 44% females, were HSV1 seropositive (HSV1+) while 447 patients, mean age 33 years, 50% females, and 296 HC, mean age 34 years, 47% females, were CMV seropositive (CMV+). In our main analysis among seropositive participants, we investigated the main effect of patient/control status on HSV1 and CMV IgG concentrations.
There were no significant differences in CMV or HSV1 seropositivity frequencies between patients with SZ, patients with BP and HC. Among seropositive participants, patients had higher HSV1 (p<0.001) and CMV (p=0.018) IgG concentrations than HC; stratifying by diagnosis, both patients with SZ (p=0.001) and patients with BP (p=0.001) had higher HSV1 IgG concentrations than HC, while patients with SZ, but not BP, had higher CMV (p=0.045) IgG concentrations than HC (Image). For HSV1, higher IgG concentrations were associated with higher general (p=0.017), negative (p=0.041) and positive (p=0.028) psychotic symptom scores.
Image:
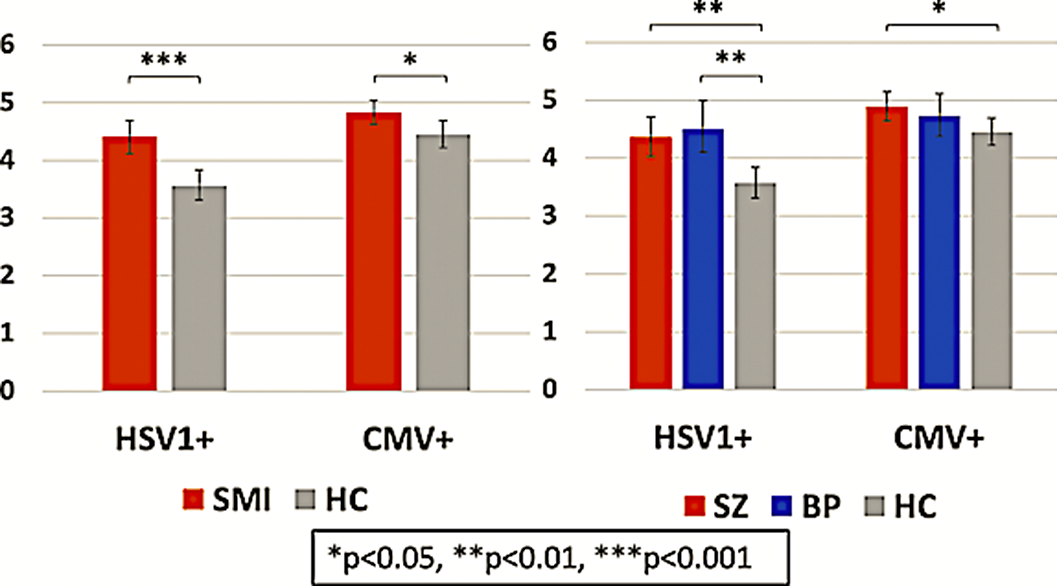
Seropositive patients with SMI showed higher HSV1 and CMV IgG concentrations than seropositive HC suggesting that patients suffer a more severe infection or exhibit an altered immune response when contracting the pathogens. For HSV1, higher IgG concentrations were linked to more psychotic symptoms.
D. Andreou: None Declared, N. E. Steen: None Declared, K. N. Jørgensen: None Declared, T. Ueland: None Declared, L. Wortinger: None Declared, L. Mørch-Johnsen: None Declared, R. Yolken: None Declared, O. Andreassen Consultant of: Consultant to HealthLytix, Speakers bureau of: Received speaker’s honorarium from Lundbeck and Sunovion, I. Agartz Speakers bureau of: Received speaker’s honorarium from Lundbeck
Postnatal cytomegalovirus (CMV) infection of immunocompetent hosts is usually inapparent but typically results in lifelong latency. Congenital CMV infections as well as CMV infections in patients with immunodeficiencies have been linked to major cerebellar pathology. Patients with severe mental illness have been repeatedly found to have smaller cerebellum, and they may be particularly susceptible to CMV infections. Finally, both animal and human studies have shown a differential male and female immune response to CMV.
We evaluated whole cerebellar grey matter volumes (CGMV) in CMV immunoglobulin G (IgG) seropositive (CMV+) and seronegative (CMV-) patients with severe mental illness and healthy controls (HC). We hypothesized that CMV seropositivity, reflecting previous infection and current latency, is associated with smaller CGMV in patients but not in HC, and that such a putative association may be sex-dependent.
We included 529 adult patients with severe mental illness (CMV+ 57%, women 48%), i.e., 324 patients with schizophrenia spectrum disorders and 205 patients with bipolar spectrum disorders, and 494 HC (CMV+ 56%, women 45%). MRI scans were obtained with a 1.5T Siemens scanner (n=596) and two 3.0T General Electric scanners (n=427), and processed with FreeSurfer v6.0. Circulating CMV IgG concentrations were measured with immunoassays. In age-, scanner- and estimated total intracranial volume-adjusted analyses of covariance (ANCOVAs), we investigated main and interaction effects of CMV status and sex on CGMV in patients and HC.
CMV+ patients had smaller CGMV than CMV- patients (p=0.042). There was no CGMV difference between CMV+ and CMV- HC (p=0.858). The adjusted CGMV means in CMV+ patients and CMV- patients were 115078 mm3 and 116725 mm3, respectively (p=0.042); the adjusted CGMV means in CMV+ and CMV- HC were 117980 mm3 and 117840 mm3, respectively (p=0.858) (Image). Among patients, a trend towards CMV-by-sex interaction (p=0.073) was found. Post-hoc analyses showed a significant CMV-CGMV association in the female patient group (p=0.005), with no association among male patients (p=0.840).
Image:

CMV IgG seropositivity is associated with smaller cerebellum in severe mental illness, an effect driven by the female patients, but not among HC. This may indicate a CMV-related deleterious impact on cerebellum restricted to patients.
None Declared