


Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly known as non-alcoholic fatty liver disease (NAFLD), is defined as the presence of hepatocyte steatosis accompanied by at least one of five cardiometabolic risk factors, in the absence of other causes of steatosis including alcohol intake(Reference Rinella, Lazarus and Ratziu1,Reference Diehl and Day2) . MASLD prevalence is estimated to be 25–30 % worldwide, and amongst those diagnosed with MASLD, approximately 25 % progress to Metabolic-Associated Steatohepatitis (MASH), leading to end-stage liver disease and associated complications(Reference Rinella and Charlton3). Over the next decade, the burden of MASLD in the Canadian population will increase by 20 %, shifting the prevalence from 20·8 % to 22·9 %. Importantly, MASH cases are estimated to increase by 35 %, and complications of end-stage liver disease will double(Reference Swain, Ramji and Patel4).
The cornerstone of management for MASLD is focused on lifestyle interventions including energetic restriction and regular physical activity(5). An emerging body of work suggests that interventions to improve dietary quality aligned with a traditional Mediterranean diet are also fundamental for reducing severity of steatosis and improving insulin sensitivity(5). Importantly, these improvements are seen irrespective of weight loss and are strategies that independently support reduction in metabolic syndrome and cardiovascular risk(Reference Ryan, Itsiopoulos and Thodis6). A typical recommended Mediterranean diet is characterised by a high intake of vegetables, whole grains, legumes, seafood and olive oil, with low intake of red meat, refined sugars and processed foods(Reference Davis, Bryan and Hodgson7). Alongside dietary intervention, physical activity should be increased to > 150 min per week of moderate-intensity activity including a combination of aerobic and resistance training(5).
Despite clear recommendations for dietary and lifestyle changes < 10 % of patients manage to achieve 7–10 % weight-loss targets over 12 months, and many patients struggle to implement and sustain these interventions(Reference Centis, Moscatiello and Bugianesi8,Reference Vilar-Gomez, Martinez-Perez and Calzadilla-Bertot9) . It has been recently recognised that the association between MASLD, mental health and binge eating further highlights the complexity of the issue and has challenged the traditional lifestyle intervention model(Reference Funuyet-Salas, Martin-Rodriguez and Perez-San-Gregorio10). MASLD has been identified as an independent risk factor for the development of anxiety and depression(Reference Labenz, Huber and Michel11,Reference Shea, Lionis and Kite12) . Binge eating tendencies also occur frequently in patients with MASLD(Reference Zhang, Abbasi and Malevanchik13) and contribute to heightened risk of developing metabolic syndrome, independent of obesity(Reference Hudson, Lalonde and Coit14). Therefore, understanding the complex interactions between psychological health, binge eating behaviours, dietary quality and physical activity is necessary to provide more holistic, tailored and effective interventions for MASLD treatment.
Aim
The nutritional, physical and psychological needs of patients living with MASLD have not been previously assessed in the Canadian population. The aim of this study was to characterise the prevalence and patterns of lifestyle and psychological factors in patients with MASLD. This analysis focuses on cross-sectional data, with a single time point of assessment. Logistic regression was used to explore associations between participant characteristics and lifestyle or psychological outcomes.
Methods
We conducted a cross-sectional observational cohort study including consecutive MASLD patients attending the Toronto Centre for Liver Disease Clinic at the University Health Network Toronto between March and October 2023. The study was conducted according to the protocol and guidelines of the Good Clinical Practice/ICH, based on the principles of the Declaration of Helsinki 1964, as most recently revised by the 64th WMA General Assembly in Fortaleza, Brazil, October 2013, and the local national laws governing the conduct of clinical research studies. All procedures were approved by the University Health Network Research Ethics Board, with written informed consent obtained from all patients (CAPCR/UHN REB #: 22-6024.0.1).
Patient selection and recruitment
Eligible patients with MASLD were identified by the study investigator during their standard-of-care ambulatory clinic appointments between March and October 2023. All patients were recruited from an ambulatory clinic. Following their appointment, patients met with a co-investigator who explained the study in detail and obtained written informed consent. Inclusion criteria included patients > 18 years of age diagnosed with MASLD based on imaging or biopsy and cardio-metabolic criteria(Reference Rinella, Lazarus and Ratziu1). Patients were excluded if they had decompensated cirrhosis, coexisting viral hepatitis or any other co-morbid acute and/or chronic medical or severe and uncontrolled psychiatric disorder that could interfere with study participation. Eligible patients were identified by the study investigator during standard-of-care outpatient clinic appointments. Following their appointment, patients met with the co-investigator where the study was explained in detail and written consent was obtained.
Despite growing evidence for lifestyle interventions, adherence to nutritional and physical activity recommendations and psychological behaviours among patients with MASLD has not been previously characterised in Canada. Clinical Practice Guidelines recommend the Mediterranean diet for the management of MASLD(Reference Tacke, Horn and Wong15). In this clinic, all patients receive counselling from a specialist hepatologist, which includes dietary education and written information, emphasising adherence to a Mediterranean diet consistent with current guideline recommendations. Education occurs at the initial consultation and is reinforced at follow-up appointments.
Data collection
Patient demographics including age, sex, weight, height, BMI and ethnicity were collected. The four questionnaires were completed by patients immediately following their face-to-face standard-of-care clinic appointment. Each questionnaire was administered once per patient. All data, including questionnaires, clinical characteristics and laboratory measures, were collected at a single time point immediately following each patient’s face-to-face standard-of-care clinic appointment. For patients whose laboratory data were not available on the day of data collection, the most recent biochemical results from the previous 6 months were accessed.
Questionnaires
Three validated questionnaires were self-applied by the patient: (1) International Physical Activity Questionnaire Short Form (IPAQ-SF)(16) measures the intensity, frequency and duration of an individual’s physical activity in seven items that ask about the time spent during the past week doing vigorous-and moderate-intensity activities, as well as walking and time spent sitting. Individuals are categorised into low, moderate or high physical activity. High activity is equivalent to > 1 h of moderate-intensity activity above basal activity or > 30 min of vigorous-intensity activity above basal levels daily. Moderate activity is 30 min of at least moderate-intensity activity on most days of the week, and low activity is any individual not meeting high or moderate activity categories(Reference Craig, Marshall and Sjostrom17). (2) The Hospital Anxiety and Depression Scale (HADS)(Reference Zigmond and Snaith18) is a validated screening tool to identify the presence and severity of anxiety and depressive symptoms in medical patients. HADS comprises two seven-item subscales to measure anxiety (HADS-A) and depression (HADS-D) using a four-point Likert-type scale. For each subscale, a score of 8 or more indicates borderline abnormal, and a score of 11 or more indicates abnormal anxiety and depressive symptoms. (3) The Binge Eating Scale (BES)(Reference Gormally, Black and Daston19,Reference Celio, Wildley and Crow20) is a validated screening tool to assess the severity of certain behavioural, emotional and cognitive symptoms associated with Binge Eating Disorder in a sixteen-item screening questionnaire. A score of 18 or greater is positive for binge eating risk, and a score of 27 or greater is indicative of severe binge eating. The fourth questionnaire was completed with a Registered Dietitian; the energy-restricted Mediterranean Diet Adherence Screener (er-MEDAS)(Reference Schroder, Zomeno and Martinez-Gonzalez21) measures adherence to an energy-restricted Mediterranean diet describing both total and individual component adherence in seventeen questions. Compliance with each of the seventeen questions is scored with one point, with a total score of zero meaning null adherence and a maximum score of 17 meaning maximum adherence(Reference Alvarez-Alvarez, Martinez-Gonzalez and Sanchez-Tainta22). Poor adherence is defined as a score ≤ 7, moderate 8–10 and high for a score 11–17(Reference Martinez-Gonzalez, Buil-Cosiales and Corella23).
Clinical characteristics and laboratory data
Clinical characteristics and laboratory data were collected retrospectively from electronic medical records, including the presence of type 2 diabetes mellitus, hypertension, dyslipidaemia, obstructive sleep apnoea, polycystic ovarian syndrome, thyroid disease, anxiety or depression (+/− anti-anxiolytics or antidepressants). History of alcohol intake was obtained during medical review using structured questions from our electronic medical chart which included (1) how often do you drink alcohol, (2) how many drinks containing alcohol do you have on a typical day when drinking and (3) how often do you have six or more drinks on one occasion. Biochemical tests performed within the previous 6 months when available were collected including alanine transaminase, aspartate transaminase, prothrombin time, international normalised ratio, albumin, total bilirubin, Hb, platelet count, creatinine, ferritin, total cholesterol, LDL-cholesterol, HDL-cholesterol, TAG and glycated Hb (HbA1c).
Fibrosis stage was determined using liver stiffness measurement (LSM) assessed by Vibration Controlled Transient Elastography (VCTE) (Fibroscan) or liver biopsy when available. Non-advanced fibrosis was defined as F0–F2 on Fibroscan or biopsy and advanced fibrosis as F3–F4. Fibroscan cut-off value used for advanced fibrosis was ≥10 kPa(Reference Anstee, Lawitz and Alkhouri24). Serum non-invasive tests included the FIB-4, APRI and NAFLD fibrosis score. FIB-4 cut-off values for fibrosis categories were defined as < 1·3 for F0–2, > 2·67 for F3–4 and 1·3–2·67 as indeterminate(Reference Hagström, Talbäck and Andreasson25). APRI cut-off values were defined as < 0·5 for F0–1, > 1·0 for F2–4 and 0·5–1·0 as indeterminate(Reference Angulo, Bugianesi and Bjornsson26). NAFLD fibrosis score cut-off values were < –1·455 for F0–2, > 0·675 for F3–4 and –1·455–0·675 as indeterminate(5).
Data analysis
Demographic and clinical information of the patients was presented using the median with interquartile range (IQR) for continuous variables and frequency with percentage for categorical variables. Before conducting the analysis, any missing data were addressed through pairwise deletion, and continuous variables were normalised using log-scale transformation.
The study included 100 participants from a single centre. Given the sample size and observational design, this analysis is exploratory, aiming to generate hypotheses regarding lifestyle adherence in MASLD rather than to provide definitive estimates. We used the Wilcoxon rank-sum test for continuous variables and the χ 2 test (or Fisher’s exact test for small sample sizes) for categorical variables. For multivariate analysis, stepwise logistic regression was performed to examine the association between the proportion of patients with advanced fibrosis stage and their demographic and clinical variables. All tests were two-tailed, and statistical significance was established at a threshold of a P-value < 0·05. The statistical analysis was carried out using R version 4.3.0.
Results
Patient demographics
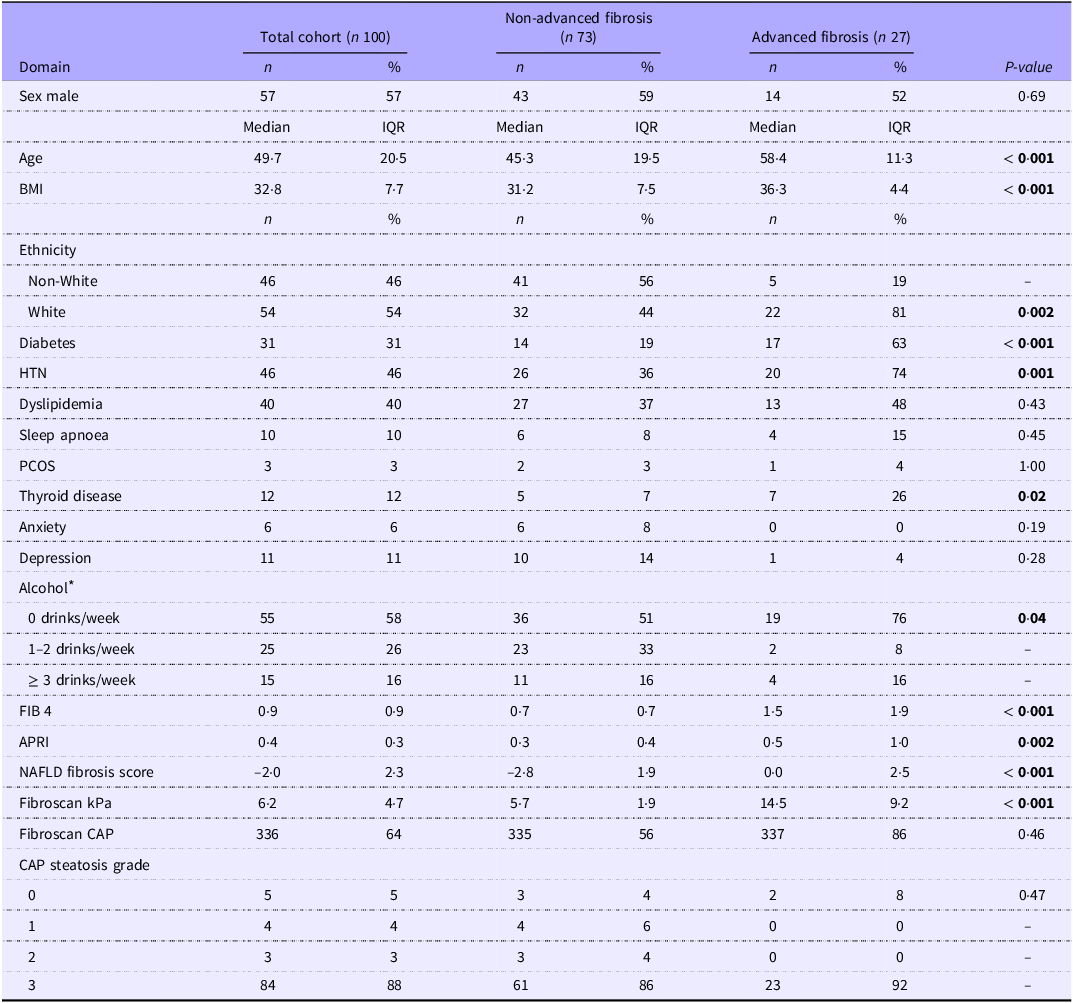
One-hundred adults with MASLD were included in the study. Our study cohort was 57 % male, with a median (IQR) age of 49·7 (20·5) years, BMI 32·8 (7·7) kg/m2 and weight 95·0 (27·2) kg. The prevalence of type 2 diabetes mellitus was 31 %, dyslipidaemia 40 % and hypertension 46 % (see Table 1 for Demographic and Clinical Data).
Comparison of demographics between patients with advanced fibrosis and non-advanced fibrosis

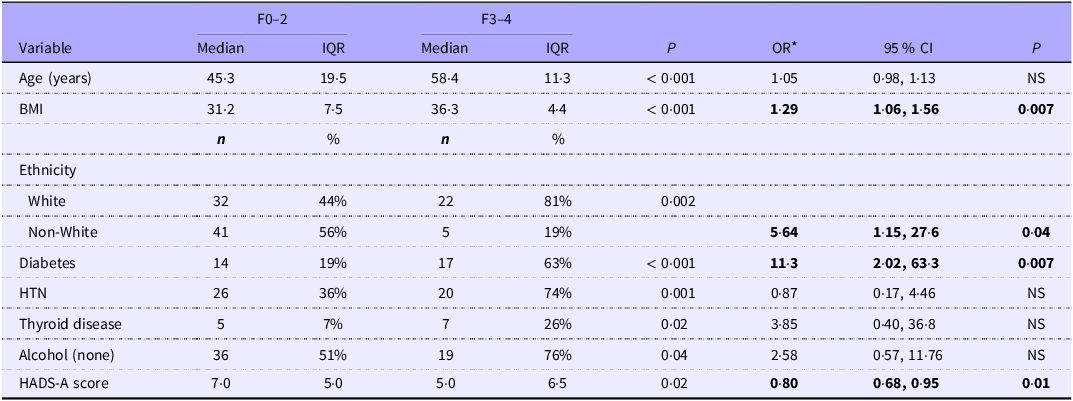
IQR, interquartile range; HTN, hypertension; PCOS, polycystic ovary syndrome; FIB 4, fibrosis-4 index; APRI, AST to platlet ratio index; NAFLD, non-alcoholic fatty liver disease; CAP, controlled attenuation parameter.
Bold signifies statistical significance e <0.05.
*Missing n 5.
Adults with MASLD with advanced fibrosis were older (median age 58·4 v. 45·3 years; P < 0·001), had a greater BMI (median 36·3 v. 31·2; P < 0·001) and a higher presence of metabolic risk factors including type 2 diabetes mellitus (P < 0·001), hypertension (P = 0·001), thyroid disease (P = 0·02) and were of White ethnicity (P = 0·002), in comparison to MASLD patients without advanced fibrosis. Using a two-sample test for proportions, post hoc assessment for the strong association between diabetes and advanced fibrosis provided > 95 % power at α = 0·05. However, for other subgroup-specific associations, the study had limited statistical power due to small subgroup sizes (Table 1).
Non-invasive tests showed higher scores in patients with advanced fibrosis: FIB-4 (median 1·5 v. 0·7, P < 0·001), APRI (median 0·5 v. 0·3, P = 0·002) and NAFLD fibrosis scores (median 0·0 v. −2·89, P < 0·001). There was no significant difference in the grade of steatosis (CAP score) measured by LSM Fibroscan between groups.
Anxiety, depressive and binge eating symptoms
The prevalence of clinically diagnosed anxiety was 6 % (n 6) and depression 11 % (n 11). Patients with normal/borderline anxiety (HADS-A ≤ 10) had lower BMI compared with those with moderate-severe anxiety (HADS-A > 10) (32·1 ± 6·2 v. 36·0 ± 4·4 kg/m2; P = 0·0077). There were no differences in BMI for patients with and without depression on HADS-D. There was a weak correlation between BMI and BES (Spearman’s rho 0·29; P = 0·003). Classification of patients according to BES (≤ 17 = none, 18–26 = mild-moderate, ≥ 27 = severe binge eating) indicated a higher BMI for mild-moderate BES compared with none (37·0 ± 7·6 v. 32·1 ± 5·4 kg/m2; P = 0·002). There were no significant differences in BMI between severe and none or mild-moderate BES.
There were no significant differences in rates of clinically diagnosed anxiety or depression between MASLD groups with advanced or non-advanced fibrosis.
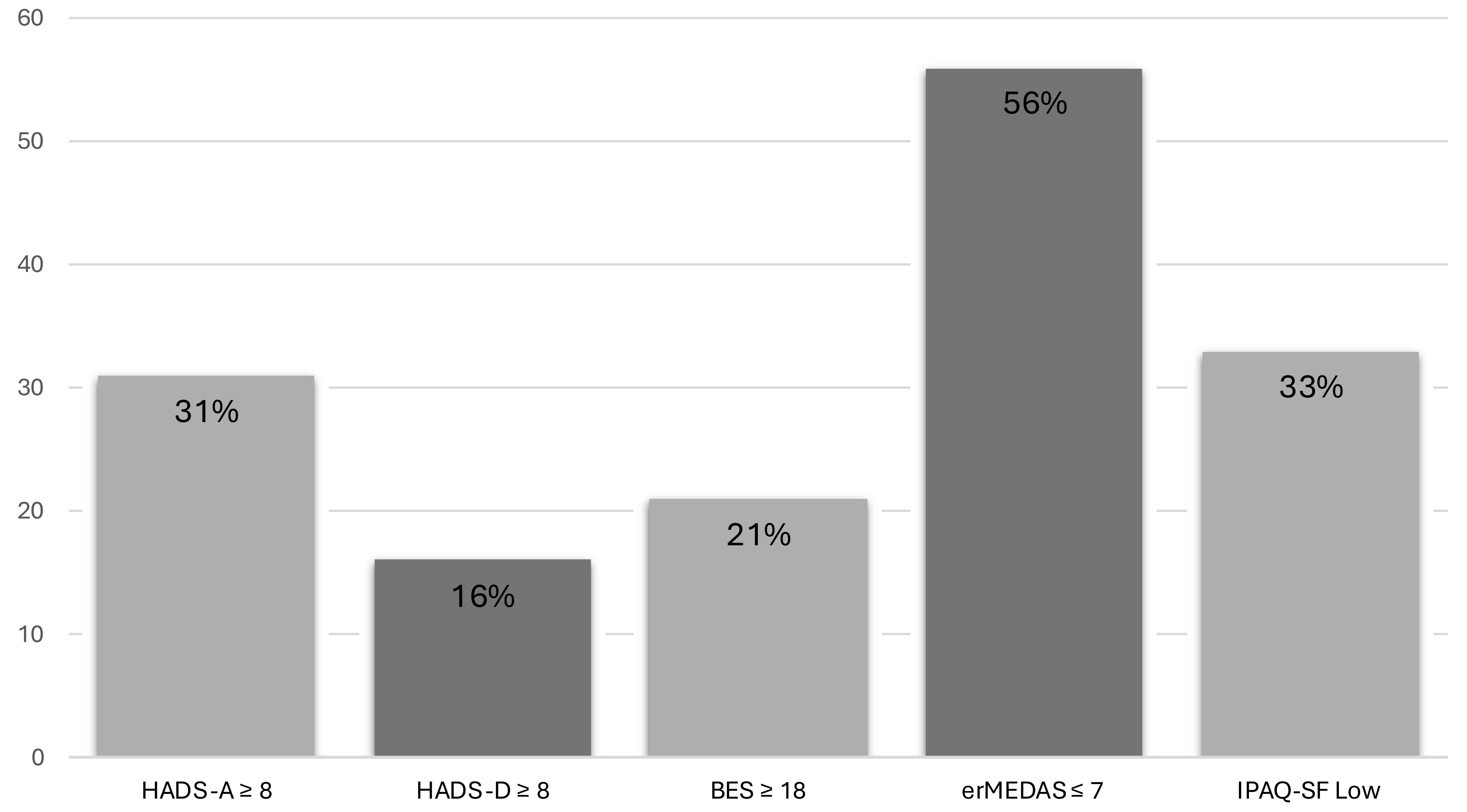
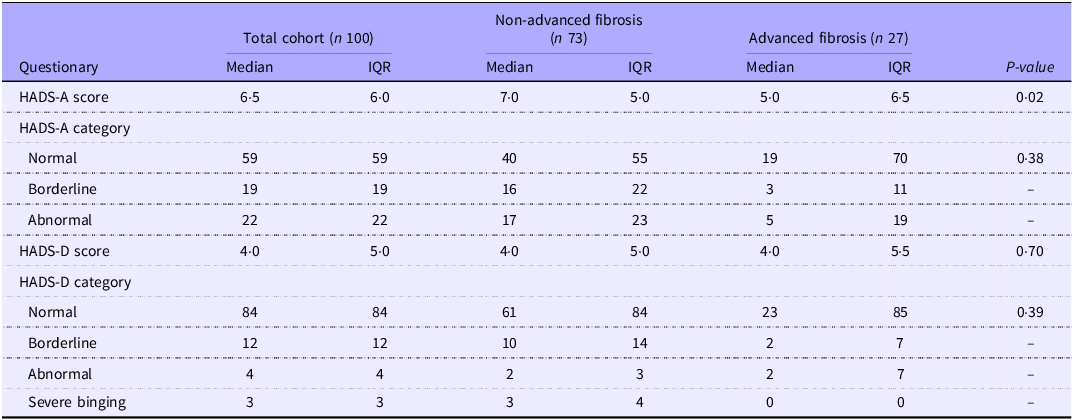
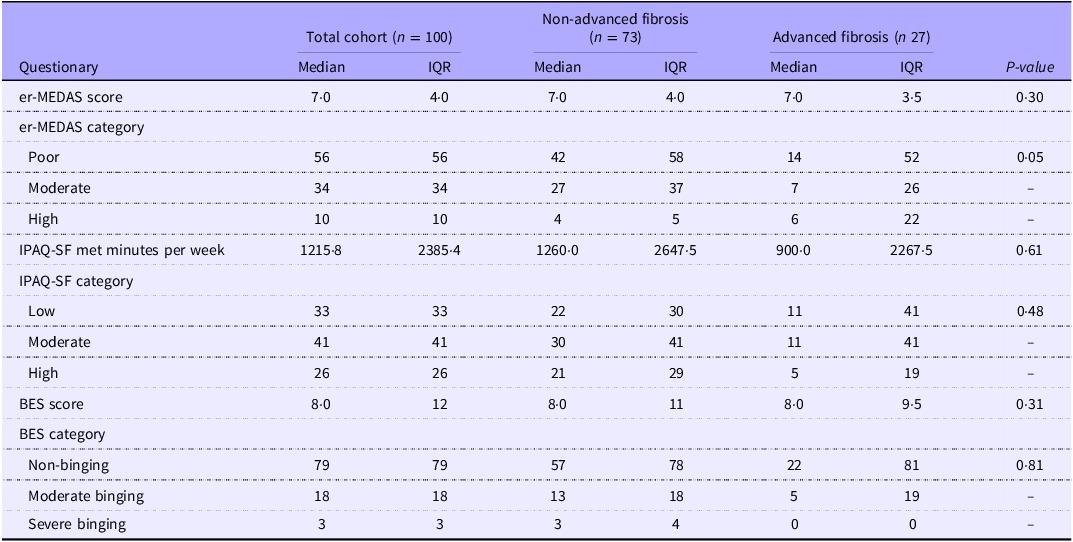
The median HADS-A score for the overall cohort was 6·5 (IQR 6·0), and 31 % had scores in borderline or abnormal range, higher than the 6 % with reported anxiety in their medical history (Figure 1). Five of these six patients with a known history of anxiety had HADS-A score ≥ 11 (abnormal). Overall, seven patients were on anxiolytics, including three with a history of anxiety (Table 2). Patients with non-advanced fibrosis had a significantly higher HADS-A score than patients with advanced fibrosis (median 7·0 v. 5·0, P = 0·02). The median HADS-D score for the overall cohort was 4·0 (IQR 5·0), with 16 % reporting borderline or abnormal scores, which was higher than 11 % with a medical history of depression. Three of the eleven patients with a known history of depression reported HADS-D ≥ 11 (abnormal). Seven of the sixteen patients with HADS-D score ≥ 8 (borderline/abnormal) were on antidepressants. There were no differences in HADS-D between groups with and without advanced fibrosis. Overall, 21 % of patients reported moderate-severe binge eating behaviour (Figure 1). The median BES score was 8·0 (IQR 12·0), and there were no significant differences between the advanced and non-advanced fibrosis groups (Table 3). Anxiety and depression were not associated with BES.
The prevalence of mood disorder in our cohort was 16–31 % based on HADS-A and HADS-D ≥ 8 indicating borderline/abnormal anxiety and depression, respectively. One-fifth of patients had BES score ≥18 indicating moderate/severe binge eating behaviour. Most patients in our cohort had poor adherence to a Mediterranean diet with er-MEDAS ≤ 7, and one-third had low quality of physical activity. HADS, the Hospital Anxiety and Depression Scale; BES, the Binge Eating Scale; er-MEDAS, the energy-restricted Mediterranean Diet Adherence Screener; IPAQ-SF, International Physical Activity Questionnaire Short Form.

Presence of anxiety and depression symptoms

HADS, the Hospital Anxiety and Depression Scale; IQR, interquartile range.
Lifestyle behaviours

Er-MEDAS, the energy-restricted Mediterranean Diet Adherence Screener; IQR, interquartile range; IPAQ-SF, International Physical Activity Questionnaire Short Form; BES, the Binge Eating Scale.
Mediterranean dietary quality and physical activity
The median er-MEDAS score for the entire MASLD group was 7·0 (IQR 4·0) and included 56 % of patients with poor dietary adherence, 34 % with moderate dietary adherence and only 10 % had high dietary adherence (Table 3). There were no significant differences in the er-MEDAS between advanced and non-advanced fibrosis groups (P = 0·30). The median IPAQ-SF total met minutes per week was 1215·8 (IQR 2385·4), with 33 % of patients reporting low physical activity (Figure 1), 41 % moderate physical activity and 26 % high physical activity. There was no significant difference between groups of patients with non-advanced fibrosis and advanced fibrosis (P = 0·61). There was no association between poor dietary adherence and activity, anxiety, depression or BES. Likewise, lower activity levels were not associated with anxiety, depression or BES.
Alcohol intake
Alcohol intake history was available in ninety-five patients, and forty (42 %) patients reported weekly alcohol consumption (Table 1). Of the patients consuming alcohol, 26 % had 1–2 drinks/week, and only 16 % had ≥ 3 drinks/week. None of our cohort met the alcohol consumption threshold for Metabolic and Alcohol Associated Liver Disease. There was a greater proportion of patients that reported any alcohol intake in the non-advanced fibrosis group compared with the advanced group 36 % v. 6 %; P = 0·03 (Table 1).
Ethnicity and advanced fibrosis
There was a statistically significant difference in ethnicity distribution between patients with non-advanced and advanced fibrosis (P = 0·033). This finding is mainly explained by the White group, which comprised over half of the cohort and had the highest proportion of advanced fibrosis (40·7 %). In contrast, most other ethnic groups had very few or no cases of advanced fibrosis, which contributed to the overall group difference but cannot be interpreted individually due to their small sample sizes (online Supplementary Table 2).
Risk factors for advanced fibrosis
We next assessed if there were any risk factors associated with the presence of advanced fibrosis. In multivariable analysis, advanced fibrosis stage was independently associated with type 2 diabetes (OR 11·3, 95 % CI 2·02, 63·3, P < 0·007), BMI (OR 1·29, 95 % CI 1·06, 1·56, P = 0·007), White ethnicity (OR 5·64, 95 % CI 1·15, 27·6, P = 0·04) and lower anxiety score, HADS-A (OR 0·80, 95 % CI 0·68, 0·95, P = 0·01, Table 4). There was no independent association with age or alcohol consumption. We further evaluated an independent association between ethnic subgroups and advanced fibrosis. Although ethnicity showed a significant overall difference between groups in univariate analysis, none of the individual ethnic categories remained independently associated with advanced fibrosis after adjustment, likely due to small subgroup sample sizes and wide CI. Other variables such as age, hypertension, thyroid disease and alcohol intake were not independently associated with advanced fibrosis in the adjusted model (online Supplementary Table 3).
Variables with significant differences between advanced and non-advanced fibrosis

IQR, interquartile range; HADS, the Hospital Anxiety and Depression Scale.
Bold signifies statistical significance e <0.05.
*Multivariate analysis OR and significant P-values are shown in bold.
Discussion
This is the first study in a Canadian MASLD cohort to assess lifestyle behaviour, including binge eating pattern, along with anxiety and depression, in relation to liver disease severity. Our findings indicate that patients with MASLD report anxiety and depression at a higher rate than recognised or documented during a routine clinical assessment. Most patients with MASLD had poor compliance with a Mediterranean diet, 20 % had moderate/severe binge eating behaviour and one-third of patients had low activity levels.
MASLD is a rapidly growing public health concern worldwide, currently affecting approximately 8 million Canadians. MASLD prevalence will increase by 20 % in less than a decade(Reference Swain, Ramji and Patel4). Despite these alarming trends, MASLD remains underdiagnosed, and patients often face systemic barriers that prevent effective disease management. This study highlights the importance of recognising mental health challenges that may preclude MASLD patients from engaging in recommended lifestyle strategies. Highlighting the need for multidisciplinary care for patients with MASLD, a standard tertiary liver clinic visit is mostly focused on assessment of disease severity and does not typically have the expertise to recognise important mental health concerns or binge eating patterns.
MASLD is often associated with cardiometabolic risk factors including high BMI, diabetes, dyslipidaemia and hypertension. A meta-analysis including eighty-six studies including 8 515 431 patients from twenty-two countries studied the prevalence of co-morbid conditions in patients with MASLD and reported a 51 % prevalence of obesity, 69 % of dyslipidaemia, 39 % of hypertension and 22 % of diabetes which is similar to the findings in our cohort(Reference Younossi, Koenig and Abdelatif27). Cardiometabolic dysfunction parameters, such as metabolic score for insulin resistance and lipid accumulation product, are also associated with MASLD in other chronic inflammatory diseases, but these were not available for our study(Reference Abenavoli, Scarlata and Borelli28). Several studies have shown that having co-morbid conditions confers a greater risk of histological progression(Reference Rinella, Neuschwander-Tetri and Siddiqui29). This is consistent with our data which show that the presence of diabetes and higher BMI, along with being White and lower anxiety scores, were associated with the presence of advanced fibrosis. We were unable to further assess the lower reported anxiety levels for advanced fibrosis within the scope of this study. This could partly relate to a greater period of time spent in consultation during the clinic visit, or perhaps more frequent primary care healthcare visits where mental health stressors are addressed.
The mainstay of treatment for MASLD relies on lifestyle interventions for targeted weight loss, as even modest amount of weight loss can improve steatosis. However, achieving sustained weight loss is challenging, and thus it is important to understand psychosocial components and specific lifestyle behaviours that may be a limitation for many patients. This allows an individualised management approach that enables patients to adopt a healthier lifestyle and achieve weight-loss targets. The study’s focus on lifestyle and psychological barriers highlights the need for holistic MASLD management. These findings suggest that future care models should adopt a multidisciplinary approach – integrating hepatology, nutrition, psychology and physical activity support – to address behavioural and emotional factors influencing adherence. Embedding behavioural counselling, mental health screening and ongoing patient education could improve engagement, outcomes and long-term disease self-management.
Dietary quality is one of the key modifiable factors of non-pharmacological MASLD management. Healthier eating patterns are associated with lower risk of cardiovascular morbidity and mortality(Reference Lichtenstein, Appel and Vadiveloo30). Based on er-MEDAS, 56 % of the patients in our study had poor adherence to Mediterranean dietary quality, with only 10 % displaying high adherence. Our study indicates that eating patterns should also be assessed in the clinic. Results from our BES assessment indicated that 21 % of patients had moderate-severe binge eating behaviour. A prior systematic review indicated that Western dietary patterns with high levels of processed food, red meat, dairy products and refined grains were associated with increased NAFLD, and Mediterranean dietary patterns reduced this risk by 23 %(Reference Hassani Zadeh, Mansoori and Hosseinzadeh31). Although adherence to a Mediterranean diet was not associated with lower risk of advanced fibrosis in our study, the relative percentage of patients adherent to this diet was low. Alongside the quality of the diet, physical activity is another key element in MASLD management. Sedentary behaviour was associated with MASLD in the US National Health and Nutrition Examination Survey, and low activity is associated with increased risk of disease progression(Reference Kim, Vazquez-Montesino and Li32). In our study, one-third of patients reported low activity levels, but there was no association with advanced fibrosis or mental health concerns.
There is limited information about the presence and association of depression and anxiety in patients with MASLD. A prior systematic review concluded that anxiety and depression were the most important emotional risk factors associated with NAFLD(Reference Macavei, Baban and Dumitrascu33). A cross-sectional study using data from the National Health and Nutrition Examination Survey from 2017 to 2020 in the USA, including 3327 patients, demonstrated that patients with depression were more likely to have MASLD (OR 1·77)(Reference Kim, Dennis and Cholankeril34). It is therefore necessary for healthcare providers caring for patients with MASLD to have increased awareness of the risk of depression. If untreated, depression could lead to functional impairment, limiting patients’ ability to engage with lifestyle interventions. A cross-sectional study from Brazil assessed the presence of depression and anxiety using the HADS scale. This study included 106 patients with MASLD and reported anxiety and depression in one-third of patients, with increased prevalence in females(Reference Botacin, Duarte and Stefano35). This was comparable to our cohort with 31 % of patients reporting HADS-A ≥8, although we did not find sex associations with depression or anxiety. We also found that patients with anxiety showed a reduced risk of having advanced fibrosis. This is consistent with another study from a community health promotion centre in Brazil that also included patients with both alcohol-and non-alcohol-associated fatty liver disease and showed an inverse association between MASLD and anxiety (OR = 0·75) and positive association with depression (OR = 1·17)(Reference Goulart, Bianchi and Bismarchi36).
In this study, we found that lower anxiety scores were independently associated with advanced fibrosis. There are several potential explanations for the observed association. First, patients with advanced disease may have undergone a process of psychological adaptation or acceptance over time. Having received a diagnosis and clinical follow-up, they might experience reduced uncertainty or fear compared with those earlier in the disease course, translating into lower reported anxiety. It is also possible that self-report questionnaires underestimate anxiety in patients with more advanced liver disease due to factors such as fatigue, apathy or reduced insight. Finally, measured confounders (e.g. medication use, social support or disease awareness) might have influenced both anxiety levels and fibrosis severity. Given the cross-sectional nature of this single-centre study, we are unable to provide further clarification as to the causative factors behind this association or the generalisability of these findings to other patient populations.
Several limitations should be considered. First, the study is single centre with a limited sample size, which may reduce statistical power and the ability to detect subtle associations. For example, only twelve participants in our cohort had thyroid disease. Using the observed proportions of advanced fibrosis, the post hoc power for detecting this association was approximately 67 %, and below the conventional 80 % threshold. Other non-significant findings may reflect insufficient power rather than the absence of a true association. Second, the cohort was relatively homogeneous, with over one-half being White, limiting the generalisability of our findings in more diverse populations. Further validation in larger cohorts accounting for racial and socio-economic diversity, including health literacy, is required. Another limitation is that the timing of data collection relative to disease diagnosis or referral was not standardised, which may influence the observed lifestyle and psychological measures. MASLD patients referred to our centre typically have highly variable duration and severity of disease, and as such, we were not able to control for these factors. Additionally, response rate data (i.e. the number of patients invited v. those who agreed to participate) were not collected. As a result, we are unable to comment on potential recruitment or non-response bias. Finally, the cross-sectional design precludes inference on longitudinal changes in lifestyle adherence.
Conclusion
Patients with MASLD may experience anxiety and depression at a higher rate than reported on routine Hepatology clinical assessment. Most patients with MASLD in our cohort had poor compliance with a Mediterranean diet, and one in five reported a binge eating pattern. Our findings require further validation but suggest that a combination of clinical, behavioural, psychosocial and social determinants remains important in the assessment of patients with MASLD. This will allow for a tailored approach to non-pharmacologic management, targeting specific mood disorder(s), dietary behaviour, binge eating and/or physical activity. Further studies to assess the impact of this individualised approach to management on liver disease progression and outcomes are required.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526107077
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
T. R. contributed to the study’s conceptualisation, methodology, investigation, data curation and writing of the original draft. K. P. was involved in the conceptualisation, methodology, supervision, formal analysis and both the writing of the original draft and review and editing of the manuscript. N. H. contributed to the investigation, data curation and writing of the original draft. C. B. and M. K. were involved in the investigation and data curation. R. P. contributed to the investigation and data curation as well. B. O. was responsible for formal analysis and validation. All authors participated in the review and editing of the manuscript and approved the final version.
K. P. is a consultant/advisory board member for Merck, Novo Nordisk and Resalis. Data safety monitoring board for Gilead Sciences. Research grants from Novo Nordisk. Other authors have no conflicts of interest to declare.



 Open access
Open access