


Highlights
-
EP-QuIC is a nationally accessible, highly sensitive and specific antemortem test for CJD that outperforms existing surrogate biomarker tests.
-
A positive EP-QuIC test provides a reliable measure for monitoring CJD prevalence and can enhance prion disease surveillance.
-
CJD incidence across Canada is estimated at 1.51 cases per million using EP-QuIC.
Introduction
Human prion diseases are rare, fatal neurodegenerative conditions caused by the misfolding of cellular prion proteins (PrPC) into an infectious amyloid form (PrPSc) that accumulates in the brain of affected individuals. The most common phenotypic presentation of human prion disease is referred to as Creutzfeldt-Jakob disease (CJD). CJD usually occurs sporadically (sCJD) with an annual incidence of 1–2 cases per million, although heritable (familial CJD, Gerstmann–Sträussler–Scheinker syndrome, fatal familial insomnia, 5%–15% of cases) and acquired (iatrogenic CJD, <1% of cases) forms also exist. The clinical presentation of sCJD is heterogeneous but is typically characterized by a rapidly progressing neurological decline.
CJD’s heterogeneous presentation is partly attributed to the existence of prion strains, which are accepted to represent different structural conformations of PrPSc. CJD cases are classified using biochemical analysis of PrPSc in brain tissue, which is often described as type 1 or type 2 based on electrophoretic mobility of protease-resistant PrPSc. The presence of methionine or valine at position 129 of the PRNP gene (M/M, M/V or V/V) is also known to influence CJD susceptibility and presentation. Thus, sCJD is often categorized by integrating codon 129 genotype with PrPSc biochemical subtype into six canonical molecular sCJD subtypes: MM1, VV1, MM2, VV2, MV1 and MV2.Reference Parchi, Castellani and Capellari1,Reference Parchi, Giese and Capellari2
Historically, antemortem diagnosis of CJD has primarily relied on the detection of increased levels of surrogate protein biomarkers, including 14-3-3 and tau in patient CSF, along with clinical criteria and neuroimaging. However, the recent development of the real-time quaking-induced conversion assay (RT-QuIC) has altered the landscape of CJD testing by providing a sensitive and specific test able to detect prion seeds directly in CSF. This obviates the need to rely on the detection of nonspecific markers of neurodegeneration.Reference Atarashi, Satoh and Sano3 The Prion Diseases Section (PDS) at the National Microbiology Laboratory (NML) is funded by the Public Health Agency of Canada to support surveillance of human prion disease in the Canadian population. Since 2016, all CSF specimens submitted to the NML have been tested by the end-point quaking-induced conversion assay (EP-QuIC). Like RT-QuIC, EP-QuIC has been proven to be highly specific and sensitive for the detection of CJD prions.
Here, we report PDS’s data on CJD CSF testing conducted between 2016 and 2024, following EP-QuIC’s introduction. The Canada-wide average of annual positive EP-QuIC tests was 1.51 per million. We demonstrate consistent CSF test results over time and across Canadian Provinces, and we provide additional analysis on a cohort of confirmed sCJD cases. We further report on the demographics of individuals tested and provide comparative observations between EP-QuIC results and levels of the biomarker proteins 14-3-3 and hTau. Overall, our findings serve as an update on Canadian CJD surveillance and verify EP-QuIC’s specificity and sensitivity for antemortem sCJD diagnosis.
Results
Study cohort
Table 1 summarizes CSF test results and demographic information in the cohort used for this study. We assessed 2667 EP-QuIC tests, 2659 14-3-3 ELISA tests and 2655 hTau ELISA tests collected between 2016 and 2024. Clinicians may request CSF testing on any patient suspected of CJD. While there are no strict criteria for CSF testing, clinicians typically submit samples from patients presenting with rapid neurological decline. EP-QuIC has been implemented on all submitted CSF specimens beginning in 2016, in addition to measurement of 14-3-3 and hTau in most samples, unless the amount of CSF was insufficient. Among all 2677 CSF specimens, we identified 284 cases that were subsequently confirmed as CJD following autopsy and 35 confirmed non-CJD cases. Our group performed biochemical subtyping of PrPSc glycoforms via Western blotting of brain tissues from 280/284 confirmed CJD cases and ascribed 274 cases a subtype based on the combination of biochemical subtyping result (type 1, type 2 or mixed) and codon 129 genotype (M/M, M/V or V/V). Most brain tissues were assigned to the MM1 subtype, followed by VV2, MV1, MV2 and MM2. We also identified 25 individuals with CJD-causing mutations that underwent CSF testing over the study period, and these were excluded from this cohort.
Creutzfeldt-Jakob disease (CJD) cohort demographics and CSF positivity rates. EP-QuIC result, sporadic CJD (sCJD) diagnosis following autopsy and sCJD subtype categorize CSF samples. Rates are provided with 95% confidence intervals (CI). Mean age at testing is provided with standard errors (SE)

* Of the 282 CJD cases tested via EP-QuIC, 267/282 were positive, 5/282 were indeterminate and 10/282 were negative. Among the 15 EP-QuIC false negatives, 6/15 were from xanthochromic CSF specimens and were not reported to physicians. When these six xanthochromic CSF specimens were removed, EP-QuIC’s positivity rate was 0.967 (267/276).
Overview of Canadian CJD CSF testing
Of the 2667 CSF samples tested, 563 were EP-QuIC-positive, 2069 were negative and 35 were indeterminate. Among EP-QuIC-positive specimens, 77% were also positive for 14-3-3, and 88% were positive for hTau, while 10% and 12% of EP-QuIC-negative samples had positive 14-3-3 and hTau tests, respectively (Table 1). Among 284 confirmed CJD cases, 95% were positive via EP-QuIC, 91% were positive via hTau and 81% were positive via 14-3-3. Among the 35 confirmed non-CJD cases, we identified 1 EP-QuIC “false positive,” 4 hTau “false positives” and 8 14-3-3 “false positives.” Of the 15/282 false-negative QuIC tests from confirmed CJD patients (Table 1), 6/15 were xanthochromic CSF specimens and were not reported to clinicians (xanthochromia indicates blood contamination and inhibits QuIC reactions). EP-QuIC’s positivity rate was 96.7% (267/276) upon removing these six xanthochromic tests, which better reflects EP-QuIC’s performance in the context of test results reported to clinicians.
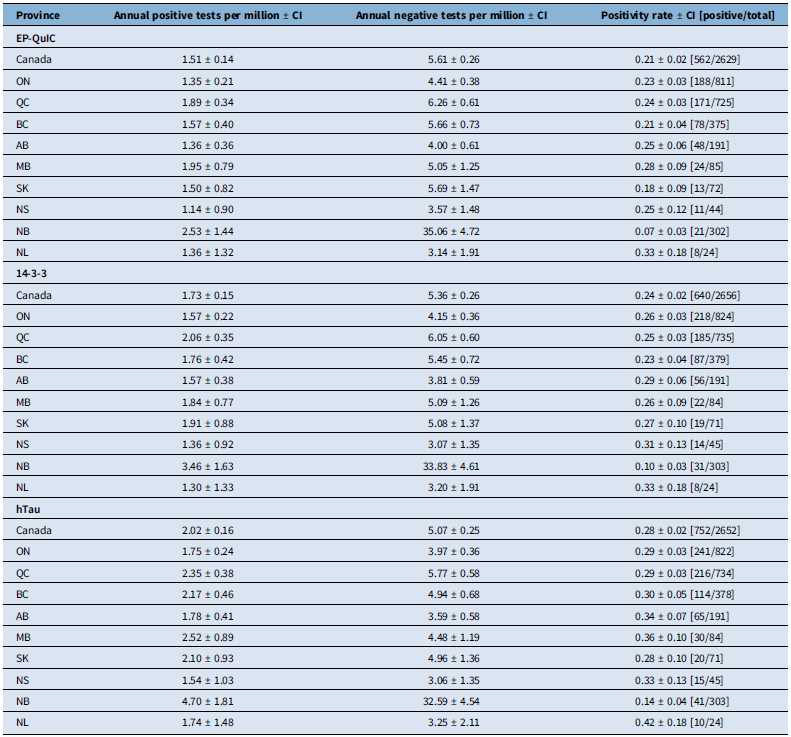
Table 2 provides an overview of annual age-adjusted CSF tests per million and test positivity rates for all of Canada and within individual provinces. Canada-wide means of age-adjusted positive CSF tests per million per year were 1.51, 1.73 and 2.02 for the EP-QuIC, 14-3-3 and hTau tests, respectively. These numbers align with the expected incidence of sCJD, commonly reported as between 1 and 2 per million per year. Test positivity rates were 0.21, 0.24 and 0.28 for the EP-QuIC, 14-3-3 and hTau tests, respectively. Poisson regression analysis revealed no difference between the Canada-wide incidence of positive EP-QuIC and 14-3-3 tests, while hTau had a significantly higher positive test incidence compared to both EP-QuIC (OR = 1.30, p = 8.7e-6) and 14-3-3 (OR = 1.16, p = 0.014).
Creutzfeldt-Jakob disease CSF testing across Canadian provinces. Annual tests per million were age-adjusted and are provided with 95% confidence intervals (CI)

ON = Ontario; QC = Quebec; BC = British Columbia; AB = Alberta, MB = Manitoba; SK = Saskatchewan; NS = Nova Scotia; NB = New Brunswick; NL = Newfoundland.
Temporal and geographic dynamics of CJD CSF tests in Canada
To assess CSF test performance over time, we examined temporal trends in the age-adjusted annual number of positive and negative EP-QuIC, 14-3-3 and hTau tests per million, smoothed by yearly rolling averages (Figure 1a). While the total number of CSF test submissions exhibited some fluctuations over time, the incidence of positive test results was stable, except for a decrease in positive testing from 2020 to 2022 that can be attributed to the COVID-19 pandemic. When examined longitudinally through yearly rolling averages, CSF positive rates were also stable, although the decline in positive CSF tests during the pandemic was again evident (Figure 1e).
Temporal and geographic trends of Creutzfeldt-Jakob disease CSF testing in Canada. (A) Canada-wide annual age-adjusted CSF tests per million (positive and negative) smoothed using 1-year rolling averages over time. (B) Canada-wide CSF test positivity rates smoothed using 1-year rolling averages over time. (C) Heatmaps illustrating geographic distributions of annual age-adjusted positive CSF tests per million. (D) Odds ratios from Poisson regression comparing annual age-adjusted positive CSF tests per million across provinces (error bars = 95% confidence interval). ON = Ontario; QC = Quebec; BC = British Columbia; AB = Alberta; MB = Manitoba; SK = Saskatchewan; NS = Nova Scotia; NB = New Brunswick; NL = Newfoundland.

Table 2 compares the geographic distribution of CSF testing across Canadian provinces through annual age-adjusted tests per million and CSF test positivity rates. Positive annual age-adjusted CSF tests in Canadian provinces are also provided as a map (Figure 1c), along with provincial odds ratios from Poisson regression analysis (Figure 1d). CSF positive test incidences and positivity rates were comparable across most Canadian provinces, apart from New Brunswick. New Brunswick submits higher total numbers of CSF samples per capita (Table 2), and this was reflected in lower CSF positivity rates (Figure 1d). Despite the enhanced CSF testing conducted in New Brunswick, the incidence of positive EP-QuIC tests is only slightly higher than the rest of the country, at 2.53 positive tests per million per year. New Brunswick’s positive EP-QuIC test incidence did not differ significantly via Poisson regression (Figure 1d), indicating that this difference reflects New Brunswick’s high numbers of test submissions. Indeed, we observed no significant differences in positive test incidence when comparing individual tests across provinces.
Comparison of CSF testing across sCJD subtypes
We also examined CJD CSF testing in the cohort of 274 autopsy-confirmed cases for which biochemical subtyping was performed. The CSF positivity rates for these cases were determined and are provided in Table 1. For each sCJD subtype, we also provide odds ratios from logistic regression analysis of CSF positivity rates (Figure 2a) and 14-3-3 and hTau abundances (Figure 2b). As expected, EP-QuIC’s reported sensitivity was reflected by positivity rates of 1 across most sCJD subtypes. Only 8/272 confirmed sCJD cases were associated with a negative EP-QuIC result, with another 5 cases producing an indeterminate EP-QuIC result. Most of these false negatives (8/13) originated from cases of sCJD MM1, the most common sCJD subtype.
Demographic breakdown of Creutzfeldt-Jakob disease (CJD) CSF test results. (A) Odds ratios from logistic regression comparing CSF test positivity rates by sporadic CJD (sCJD) subtype (dot plot, error bars = 95% confidence interval, n tests above points). (B) CSF 14-3-3 and hTau abundances stratified by sCJD subtype (violin plots, thresholds = dashed lines, n tests above violins). (C) Odds ratios from logistic regression comparing CSF test positivity rates by codon 129 genotype (dot plot, error bars = 95% confidence interval, n tests above points). (D) CSF 14-3-3 and hTau abundances in EP-QuIC-positive and EP-QuIC-negative samples, stratified by codon 129 genotype (violin plots, thresholds = dashed lines, n tests above violins). (E) Stacked bar plot showing codon 129 genotype distribution among positive and negative samples for each CSF test. (F) Odds ratios from logistic regression comparing CSF test positivity rates by age group (dot plot, error bars = 95% confidence interval, n tests above points). (G) CSF 14-3-3 and hTau abundances in EP-QuIC-positive and EP-QuIC-negative samples, stratified by age group (violin plots, thresholds = dashed lines, n tests above violins). (H) Odds ratios from logistic regression comparing CSF test positivity rates by sex (dot plot, error bars = 95% confidence interval, n tests above points). (I) CSF 14-3-3 and hTau abundances in EP-QuIC-positive and EP-QuIC-negative samples, stratified by sex (violin plots, thresholds = dashed lines, n tests above violins). Neg. = negative; Pos. = positive; F = female; M = male.

Although QuIC is the most accurate CSF test for CJD, it was interesting to explore any relationship between 14-3-3 and hTau biomarkers and sCJD subtypes. The following trends in 14-3-3 and hTau positivity rates and signal intensities were observed among sCJD subtypes: VV2 > MM1 > MV1 > MV2 ∼= MM2 (Table 1, Figure 2a and 2b). MM2 and MV2 were associated with significantly lower 14-3-3 positivity rates compared to VV2 (MM2/VV2: OR = 0.050, p = 0.013; MV2/VV2: OR = 0.072, p = 0.013) and MM1 (MM2/MM1: OR = 0.14, p = 0.039; MV2/MM1: OR = 0.20, p = 0.21). CSF abundances of 14-3-3 and hTau were also found to quantitatively differ based on CJD subtype. For instance, MM2 and MV2 were associated with significantly lower biomarker abundances compared to VV2 and MM1: 14-3-3 MV2/VV2: OR = 0.36, p = 3.2e-13; hTau MV2/VV2: OR = 0.26, p = 3.4e-13; 14-3-3 MM2/VV2: OR = 0.39, p = 1.0e-6; hTau MM2/VV2: OR = 0.26, p = 2.1e-7, 14-3-3 MV2/MM1: OR = 0.43, p = 8.0e-12; hTau MV2/MM1: OR = 0.31, p = 1.0e-12; 14-3-3 MM2/MM1: OR = 0.46, p = 4.1e-5; hTau MM2/MM1: OR = 0.32, p = 3.0e-6. Overall, these results indicate that the 14-3-3 and hTau tests do not perform equivalently across all CJD subtypes. Notably, the MV2 and MM2 subtypes were associated with lower levels of CSF biomarkers 14-3-3 and hTau.
CJD CSF test positivity rates differ across age groups
Sporadic CJD typically presents in individuals between 55 and 75 years of age (median age of onset = 67 years), and so we examined the age distribution at the time of CSF testing between samples that tested positive and negative via EP-QuIC (Table 1). EP-QuIC-positive CSF specimens were associated with a mean age at testing of 68.6 years, which was significantly higher than EP-QuIC-negative CSF specimens that had a mean age of 65.7 years (p = 0.0025). We next compared CSF test positivity rates across different age groups using odds ratios from logistic regression (Figure 2f). The highest positivity rates were evident in individuals between 60 and 85 years of age, with significantly lower EP-QuIC and hTau positivity rates in individuals < 50. For example, in all three tests, the greatest differences were observed between individuals 60–64 compared to those < 50 years of age, producing odds ratios of 6.6 (p = 4.6e-6) for EP-QuIC, 2.8 (p = 6.0e-4) for hTau and 2.2 (p = 0.039) for 14-3-3. We also examined 14-3-3 and hTau abundances in EP-QuIC-positive and EP-QuIC-negative CSF samples broken down by age group through GLM regression analysis (Figure 2g). As expected, EP-QuIC-positive samples were associated with significantly higher biomarker abundances within each individual age group. When only considering CSF samples that tested positive via EP-QuIC, 14-3-3 and hTau signal intensities were similar across age groups. A trend of elevated 14-3-3 and hTau signal intensities in EP-QuIC-negative CSF samples from older age groups was evident, although differences between individual age groups did not reach significance. This observation reinforces the fact that 14-3-3 and hTau are nonspecific biomarkers of neuronal degeneration and are elevated in association with age-related diseases.
CJD 14-3-3 and hTau CSF biomarker abundance is associated with codon 129 genotype
The presence of methionine or valine at codon 129 of the PRNP gene (M/M, M/V or V/V) is associated with CJD presentation and susceptibility, and so we next compared CSF testing in samples stratified by codon 129 genotype. Unlike EP-QuIC, 14-3-3 and hTau positivity rates differed between codon 129 genotypes (Figure 2c). Compared to M/M, CSF biomarker positivity rates were lower in M/V samples (14-3-3: OR = 0.40, p = 0.0013; hTau: OR = 0.48, p = 0.028) and higher in V/V samples (14-3-3: OR = 3.00, p = 0.018; hTau: OR = 2.85, p = 0.060). We also compared 14-3-3 and hTau abundances between codon 129 genotypes in EP-QuIC-negative and EP-QuIC-positive CSF samples (Figure 2d). As reflected by positivity rates, EP-QuIC-positive M/V samples were associated with significantly lower 14-3-3 and hTau CSF abundances compared to M/M (14-3-3: OR = 0.62, p = 1.6e-4; hTau: OR = 0.52, p = 8.0e-5) and V/V (14-3-3: OR = 0.48, p = 3.9e-7; hTau: OR = 0.40, p = 1.4e-6). Interestingly, EP-QuIC-negative V/V samples were associated with higher 14-3-3 (OR = 2.06, p = 0.11) and hTau (OR = 3.44, p = 0.018) CSF abundances compared to M/V. The distribution of codon 129 genotypes was also compared between CSF samples that tested positive and negative via each test (Figure 2i). In all three tests, positive CSF samples were enriched with M/M and V/V genotypes and depleted with the M/V genotype relative to CSF samples that tested negative. Overall, these results support the theory that heterozygosity at codon 129 is protective against CJD.
CJD CSF testing is comparable between males and females
CSF test positivity rates were also compared between males and females (Figure 2h). As expected, EP-QuIC positivity rates were identical between males and females. We found that males exhibited a slight trend toward lower positivity rates for the 14-3-3 (OR = 0.82, p = 0.053) and hTau (OR = 0.82, p = 0.040) biomarkers. We also compared 14-3-3 and hTau abundances across EP-QuIC-positive and EP-QuIC-negative CSF samples collected from males and females and did not identify any biological sex-associated differences (Figure 2i).
Discussion
We estimated the Canadian annual CJD incidence to be 1.51 cases per million based on 563/2667 EP-QuIC-positive CSF samples collected between 2016 and 2024. While we did not apply case definitions to our cohort in this study, our laboratory previously reported comparable EP-QuIC sensitivity and specificity in a smaller cohort.Reference Simon, Peterson and Phillipson4 The general trend of increasing CJD incidenceReference Gao, Tian and Xiao5 is supported by comparing our estimate of 1.51 positive EP-QuIC tests per million with the crude sCJD mortality rate of 1.18 per million per year reported by the Canadian CJD Surveillance System between 1998 and 2013.Reference Coulthart, Jansen and Connolly6 This increase in CJD incidence has been attributed to an aging population, increased disease awareness and improved antemortem tests for CJD.Reference Watson, Brandel and Green7
Estimated CJD incidences were similar across Canadian provinces, although New Brunswick exhibited a slightly higher incidence that we attribute to a higher sampling rate. Over the study period, New Brunswick averaged 37.5 CSF test submissions per million compared to 7.1 test submissions per million from the rest of Canada. Indeed, this New Brunswick cohort represents the highest density of CJD testing performed in a focused Canadian population to date.Reference Klug, Wand and Boyd8,Reference Klug, Wand and Simpson9 This localized increase in sample submissions was driven by concerns of individuals who exhibited neurological syndromes of an unknown cause.10 Of 303 samples submitted by the Province of New Brunswick, 21 were EP-QuIC positive. Although this translates to an annual CJD incidence of 2.5 per million, slightly higher than the national average, we attribute this to a general increase in vigilance and heightened awareness of CJD testing in local healthcare communities. Similar instances of enhanced surveillance in a geographically restricted area have been linked with elevated detection of CJD cases.Reference Klug, Wand and Boyd8
Our findings support the use of QuIC for routine CJD diagnosis and surveillance. EP-QuIC’s positivity rate was 95% among postmortem confirmed sCJD cases that underwent CSF testing, surpassing both 14-3-3 and hTau biomarker tests and corroborating previous data.Reference Simon, Peterson and Phillipson4,Reference Watson, Brandel and Green7,Reference Budhram, Taylor, Fuller, Burneo, Knox and Pasternak11,Reference Watson, Hermann and Ladogana12 Notably, EP-QuIC’s exceptional specificity was further evidenced by the lack of false-positive tests reported for the province of New Brunswick, despite higher numbers of test submissions per population. We confirmed a single false-positive case in our cohort overall, in an individual who was diagnosed with immune-mediated encephalopathy, a class of neurological disease that has been reported to occasionally result in positive QuIC tests.Reference Hermann, Schmitz and Cramm13 EP-QuIC positivity was also uninfluenced by sCJD subtype, codon 129 genotype and biological sex – factors that we demonstrated to be associated with the measurement of the nonspecific biomarkers 14-3-3 and hTau.
We also report 15/282 confirmed CJD cases that either tested negative or inconclusive by EP-QuIC in our cohort. Six of 15 EP-QuIC false negatives were from xanthochromic CSF specimens, which we do not report as negative to clinicians because blood contamination inhibits QuIC reactions. False-negative QuIC tests can also occur in early stages of disease, and repeat testing is encouraged if there is a strong suspicion of CJD. Additionally, some inherited prion diseases, particularly fatal familial insomnia and cases of dominantly inherited prion amyloidosis such as Gerstmann–Straussler–Scheinker disease, as well as other atypical subtypes with slow disease progression, can also test negative in QuIC assays. Therefore, while a QuIC-negative result means CJD is unlikely, it does not exclude the possibility of a prion disease, and test results should be interpreted alongside clinical findings, neuroimaging and family history.
We determined that EP-QuIC, 14-3-3 and hTau positivity rates were highest in Canadian individuals between 60 and 85 years old, consistent with international data reporting sCJD’s median age of symptom onset at 67 years of age.Reference Watson, Hermann and Ladogana12,Reference Uttley, Carroll, Wong, Hilton and Stevenson14–Reference Nishimura, Harada, Koyama, Hagiya and Otsuka16 We also observed an age-dependent increase in 14-3-3 and hTau signal intensities in EP-QuIC-negative samples that further highlights the limited specificity of these surrogate biomarkers. Indeed, elevated CSF 14-3-3 and hTau levels are detected in other age-associated neurodegenerative conditions, including Alzheimer’s disease, frontotemporal dementia, dementia with Lewy bodies and vascular dementia.Reference Burkhard, Sanchez, Landis and Hochstrasser17–Reference Muayqil, Gronseth and Camicioli19 High 14-3-3 levels have also been observed in carcinomatous meningitis and anoxic encephalopathy,Reference Foote and Zhou18 which are also associated with aging.
Furthermore, we detected trends in 14-3-3 and hTau CSF abundances across sCJD subtypes, reflecting sCJD’s considerable phenotypic heterogeneity. Cases of sCJD VV2 were associated with the highest levels of CSF 14-3-3 and hTau, whereas in sCJD MM2 and MV2, the levels were conspicuously lower. Previous studies also reported higher 14-3-3 levels in classical MM1, VV2 and MV1 molecular sCJD subtypes compared to nonclassical subtypes,Reference Gmitterová, Heinemann and Bodemer20 with tau levels following similar trends.Reference Gmitterová, Heinemann, Krasnianski, Gawinecka and Zerr21–Reference Bentivenga, Gonzalez-Ortiz and Baiardi23 CSF 14-3-3 and hTau levels show some correlation with codon 129 genotype, since we observed low biomarker levels in M/V individuals and high biomarker levels in V/V individuals. We were also surprised to observe high biomarker levels in EP-QuIC-negative V/V individuals, which seems to suggest that PRNP genotype influences 14-3-3 and hTau levels independently of prion disease. Many biological functions have been attributed to PrPC, and so an indirect relationship between PRNP genotype and CSF protein levels is plausible.
Collectively, this study serves as an update on Canadian CJD surveillance and supports the use of EP-QuIC for antemortem CJD diagnosis. Our analyses focused solely on laboratory testing without cross-referencing clinical or pathological case information. For this reason, while the distribution of sCJD subtypes in our cohort was consistent with those reported from other countries’ national surveillance systems, we could not distinguish nonclassical sCJD subtypes like MM2C, MM2T, MV2K, MV2C or the recently characterized VM1 subtype.Reference Parchi, Castellani and Capellari1,Reference Gelpi, Baiardi and Nos24 Nevertheless, our thorough analyses of CJD CSF testing in a comparatively large cohort of Canadian CJD cases verified the utility of EP-QuIC as a specific and sensitive test. Continued CJD surveillance remains especially important in light of ongoing concerns of zoonotic transmission from chronic wasting disease. This prion disease is prevalent among cervids in the western Canadian provinces of Alberta and Saskatchewan and has recently spread east to Manitoba and further west into British Columbia.
Methods
Study population
We retrospectively analyzed data from 2677 patient CSF samples submitted for diagnostic testing to the Prion Diseases Section, National Microbiology Laboratory, between 2016 and 2024. This unit serves as Canada’s national reference laboratory for diagnostic testing and surveillance. Samples are tested on demand and are not prescreened with respect to any clinical criteria.
Laboratory testing
Samples were processed through three testing streams. CSF samples were tested using EP-QuIC, 14-3-3 and hTau tests, as described in our service guide: https://cnphi.canada.ca/gts/reference-diagnostic-test/4462?labId=1025. EP-QuIC was performed using an in-house assay, as previously described.Reference Cheng, Vendramelli and Sloan25 Briefly, 15 µL of CSF is added in triplicate to a reaction containing 100 µg/mL filtered recombinant hamster PrP(23-231), 160 mM NaCl, 10 µM EDTA and 10 µM Thioflavin T in PBS in a final volume of 100 µL. Before shaking, fluorescence readings are taken at t = 0 h on a FLUOstar Omega plate reader (λEx = 450 nm; λEm = 480 nm). Reactions are incubated on an Eppendorf Thermomixer C at 42°C, 900 r.p.m. (90 s on, 30 s rest) for 66 h, and end-point fluorescence values are recorded. Samples where all three replicates have a ≥4-fold increase in fluorescence over t = 0 h are considered positive, where those with three wells with <4-fold increase are considered negative. Samples with one or two positive replicates are re-run using 7.5, 15 and 30 µL CSF. Indeterminate results are reported when tests repeated with multiple CSF dilutions fail to produce a positive or negative test result. Commercial kits were used for 14-3-3 (Circulex 14-3-3 Gamma ELISA kit) and hTau (Innotest hTAU ELISA kit) biomarker testing, following the manufacturer’s instructions. Biomarker tests were classified as positive or negative based on thresholds of 20,000 absorbance units for 14-3-3 and 976 pg/mL for hTau. A plot comparing 14-3-3 and hTau abundances between EP-QuIC-positive and EP-QuIC-negative samples is provided in Supplementary Figure 1a.
Genetic sequencing of the PRNP gene was conducted on blood or brain tissue specimens to determine the codon 129 genotype and identify CJD-associated mutations. PrPSc glycotypes were confirmed via Western blot analysis of proteinase K-digested brain homogenates using methods previously described elsewhere, with slight modifications.Reference Parchi, Giese and Capellari2 PrPSc glycotypes were classified as type 1, type 2 or mixed based on the Parchi classification system.Reference Parchi, Castellani and Capellari1,Reference Parchi, Giese and Capellari2
Case definitions
Cases with a positive or negative EP-QuIC test were used to compare biomarker abundances (14-3-3 and hTau). Cases with a positive biochemical subtyping test were classified as definitive CJD cases and used to compare test sensitivities for all three CSF tests (EP-QuIC, 14-3-3 and hTau). Sporadic CJD cases were defined by a positive subtyping test with no identified PRNP mutation. Sporadic CJD cases were subtyped based on the combination of PrPSc glycotype (type 1, type 2 or mixed) and PRNP genotype (M/M, M/V and V/V). Familial CJD cases were defined by the presence of a known CJD-associated PRNP mutation, and these cases were not included in the study cohort.
Data analysis and statistics
Data analyses were conducted in R using the dplyr, emmeans, ggplot2 and complexHeatmap packages for data manipulation, statistics and visualization. Diagnostic data were cleaned by associating all test results with individual patients. When multiple tests were conducted (e.g., CSF testing), the most recent result was used for analysis. Patient age at testing was calculated using their birthdate and the date of their most recent test result. Sex and province were included as reported on test requisition forms. Prior to analysis, the dataset was filtered based on the most recent test result (> 2016-01-01 and < 2025-01-01), familial CJD cases were removed, and patients with at least one CSF test result (EP-QuIC, 14-3-3 and hTau) were retained.
The age-adjusted incidences of positive and negative CSF tests were calculated using the following age strata, associated with province-level population data from Statistics Canada: 0–17 years, 18–24 years, 25–44 years, 45–64 years, 65 years and older. Incidences were calculated separately for each stratum using the number of positive and negative tests and person-years for each group from 2016 to 2024 (EP-QuIC was implemented on all CSF samples beginning in 2016). Canada’s 2011 population was used as the reference for weighting age strata. Age-adjusted incidences were calculated as the weighted sum of age-stratified incidences, with standard errors calculated as sqrt(n/person-years).Reference Parchi, Giese and Capellari2 To examine CSF testing incidences longitudinally, annual age-adjusted incidences were smoothed using 1-year rolling averages, calculated daily and averaged over 1-year windows.
To compare age-adjusted incidences between tests and provinces, the number of positive CSF tests was fitted to a Poisson regression model (log link), with province, age group and sampling rate as covariates and log(person-years) as an offset. Pairwise comparisons between tests and provinces were performed using estimated marginal means to determine odds ratios, with p-values adjusted using the Tukey method.
Positivity rates were calculated as positive tests/total tests, with 95% confidence intervals calculated using the Wilson score interval method. Positivity rates were compared using logistic regression, with test result (positive or negative) fitted to a binary model (logit link) against province, age group, gender and codon 129 genotype as covariates. Pairwise comparisons were performed using estimated marginal means to calculate odds ratios, with p-values adjusted using the Tukey method.
CSF biomarker abundances (14-3-3 and hTau) were analyzed using a gamma generalized linear model (log link) against EP-QuIC status, codon 129 genotype, gender, age group and province as covariates. Pairwise comparisons between EP-QuIC-positive and EP-QuIC-negative CSF samples, stratified by other variables, were conducted using estimated marginal means to calculate odds ratios, with p-values adjusted using the Tukey method. Age distributions were analyzed similarly, but using a Gaussian generalized linear model.
Statistical results (pairwise comparisons) are provided in Statistical Source Data 1.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cjn.2025.10088
Acknowledgments
We would like to especially thank healthcare institutions, physicians, affected patients and families, without whose generous collaboration, this work would not have been possible. We also extend thanks to the staff of the Creutzfeldt-Jakob Disease Surveillance System, Centre for Foodborne, Environmental and Zoonotic Infectious Diseases, for assistance.
Author contributions
J.A.S., B.A.B.E and S.A.B. designed the study. A.P., K.A., C.P., D.M.S.K., R.F., L.L. and M.L. performed diagnostic testing and collated data. G.H.J. performed pathological analyses and case review. J.A.S. analyzed data and prepared figures. J.A.S., J.M., B.A.B.E. and S.A.B. drafted the manuscript and contributed to writing, review and editing.
Funding statement
This work was funded by the Public Health Agency of Canada.
Competing interests
The authors declare that there are no competing interests.






 Open access
Open access
Target article
Diagnosis of Creutzfeldt-Jakob Disease in Canada: An Update on Cerebrospinal Fluid Testing from 2016 to 2024
Related commentaries (2)
Reviewer Comment on Slota et al. “Diagnosis of Creutzfeldt-Jakob Disease in Canada: An Update on Cerebrospinal Fluid Testing from 2016–2024”
Reviewer Comment on Slota et al. “Diagnosis of Creutzfeldt-Jakob Disease in Canada: An Update on Cerebrospinal Fluid Testing from 2016–2024”