
Introduction
Labour or parturition is a physiologic process culminating in expulsion of fetus, amniotic fluid, placenta and membranes from the gravid uterus of a pregnant woman, involving sequential and integrated changes in the myometrium, decidua and cervix. In a woman with a regular 28-day cycle, labour is said to take place 280 days after the onset of the last menstrual period. However, the length of human gestation varies considerably among healthy pregnancies, even when ovulation is accurately measured in naturally conceiving women [Reference Jukic, Baird, Weinberg, McConnaughey and Wilcox1]. Initiation of labour may be best regarded as a withdrawal of the inhibitory effects of pregnancy on the tissue of the uterus, rather than as an active process mediated by the release of uterine stimulants [Reference Norwitz2]. Successful labour passes through three stages: the shortening and dilatation of the cervix; descent and birth of the fetus; and the expulsion of the placenta and membranes. Efficient uterine contractions (power), an adequate roomy pelvis (passage) and an appropriate fetal size (passenger) are key factors in this process.
Anatomy of the Female Pelvis
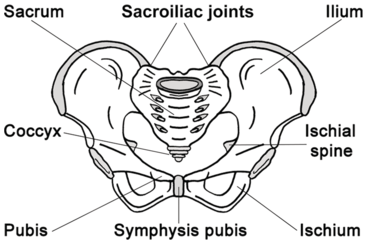
The bony pelvis consists of the two innominate bones, or hip bones, which are fused to the sacrum posteriorly and to each other anteriorly at the pubic symphysis. Each innominate bone is composed of the ilium, ischium and pubis, which are connected by cartilage in youth but fused in the adult (Figure 1.1).
Bony female pelvis.

The pelvis has two basins: the major (or greater) pelvis and the minor (or lesser) pelvis. The abdominal viscera occupy the major pelvis and the minor pelvis is the narrower continuation of the major pelvis. Inferiorly, the pelvic outlet is closed by the pelvic floor. The female pelvis has a wider diameter and a more circular shape than that of the male. The wider inlet facilitates engagement of the fetal head and labour. Numerous projections and contours provide attachment sites for ligaments, muscles and fascial layers. This distinctive shape of the human pelvis is probably not only the result of an adaptation to a bipedal gait but also a result of the need for a larger birth canal for a human fetus with a large brain [Reference Lovejoy3].
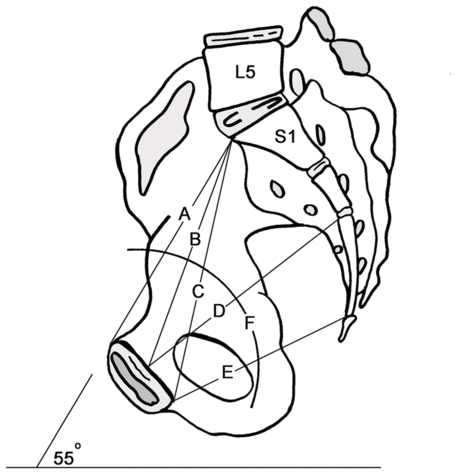
The female pelvis is tilted forwards relative to the spine and described as the deviation of the pelvic inlet from the horizontal in the sagittal plane. The pelvic ‘tilt’ or angle of inclination is measured as an angle between the line from the top of the sacrum to the top of the pubis and a horizontal line in a standing radiograph (Figure 1.2).
Female pelvis with the tilt at 55° to the horizontal plane. A) pelvic inlet (upper pubic to sacral promontory). B) mid-pubic to sacral. C) oblique inlet diameter (lower pubic to sacral promontory). D) mid-pelvic diameter (mid-symphysis to mid-sacrum). E) pelvic outlet lower symphysis to sacro-coccygeal. F) The line of descent of the fetus through the pelvis.
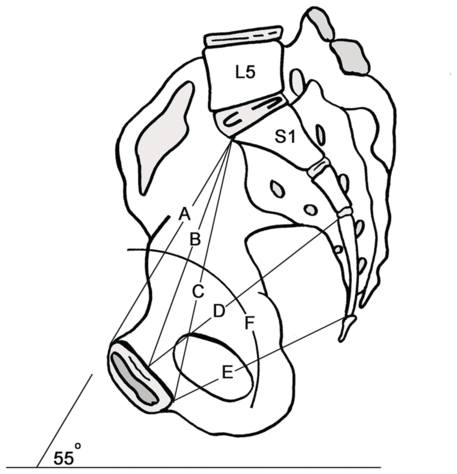
The pelvic tilt is variable between different individuals and between different races; in adult Caucasian females the pelvis is usually about 55° to the horizontal plane. It is also position-dependent and increases with growth into adulthood [Reference Mac-Thiong, Berthonnaud, Dimar, Betz and Labelle4].
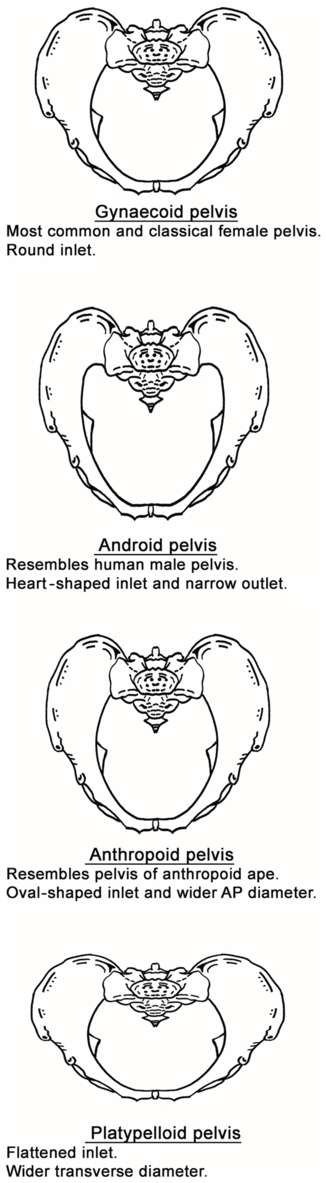
Based on the characteristic of the pelvic inlet, it is classified into four basic shapes: the round (gynaecoid), the wedge-shaped (android), the longitudinal oval (anthropoid) and the transverse oval (platypelloid) type of inlet (Figure 1.3).
The four basic types of pelvis: gynaecoid, android, anthropoid and platypelloid.
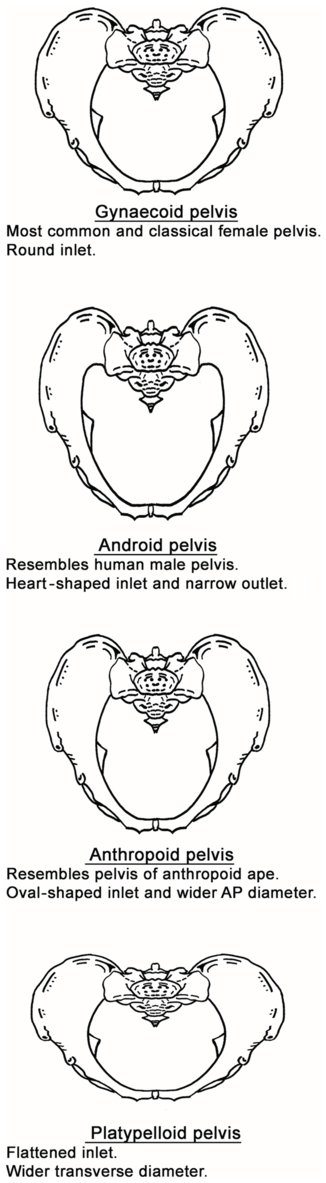
Figure 1.3 Long description
The text below for each type of pelvis is as follows. Gynecoid pelvis: Most common and classical female pelvis. Round inlet. Android pelvis: Resembles human male pelvis. Heart-shaped inlet and narrow outlet. Anthropoid pelvis: Resembles the pelvis of an arthropod ape. Oval-shaped inlet and wider A P diameter. Platypelloid pelvis: Flattened inlet. Wider transverse diameter.
However, a large number of pelvises appear to conform to intermediate shapes between these extreme types [Reference Caldwell and Moloy5]. The pelvic outlet is the lower circumference of the lesser pelvis. It is very irregular and bounded by the pubic arch anteriorly, ischial tuberosities laterally and sacrotuberous ligament and the tip of the coccyx posteriorly. In order to have a successful delivery the fetus has to pass through this bony canal, and the axis through which the fetus travels is an imaginary line joining the centre points of the planes of the inlet, cavity and outlet.
Anatomy of the Fetal Skull
The human fetal skull is considered to be the largest compared to the pelvic size of all other living primates and the most difficult part of the fetus to pass through the mother’s pelvic canal, due to its hard, bony nature [Reference Rosenberg and Trevathan6].
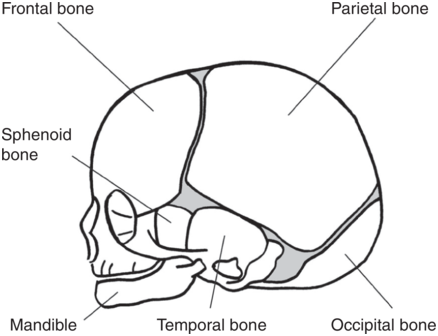
The skull bones encase and protect the brain, which is very delicate and is subjected to pressure when the fetal head passes down the birth canal. The fetal cranium is composed of nine bones (occipital, two parietal, two frontal, two temporal, sphenoid and ethmoid). Of these, the bones that compose the skull are of clinical importance during birth (Figure 1.4).
Fetal skull bones.
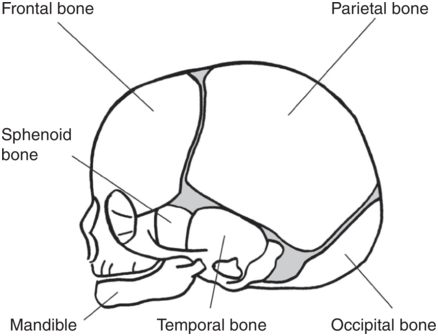
The fetal skull bones are as follows:
1. The frontal bone, which forms the forehead. In the fetus, the frontal bone is in two halves which fuse into a single bone after the age of 8 years.
2. The two parietal bones, which lie on either side of the skull and occupy most of the skull.
3. The occipital bone, which forms the back of the skull and part of its base. It joins with the cervical vertebrae.
4. The two temporal bones, one on each side of the head, are the closest to the ear.
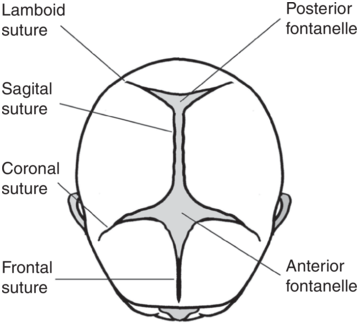
Sutures are joints between these bones of the skull. The lambdoid suture forms the junction between the occipital and the parietal bones; the sagittal suture joins the two parietal bones together; the coronal suture joins the frontal bones to the two parietal bones; and the frontal suture joins the two frontal bones together (Figure 1.5).
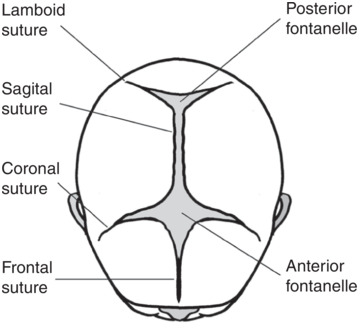
A fontanelle is the space created by the joining of two or more sutures. It is covered by thick membranes and the skin on the fetal head, protecting the brain underneath. The anterior fontanelle (also known as the bregma) is a diamond-shaped space towards the front of the fetal head, at the junction of the sagittal, coronal and frontal sutures. The posterior fontanelle (or lambda) has a triangular shape, and is found towards the back of the fetal skull. It is formed by the junction of the lambdoid and sagittal sutures. In the fetus the sutures between the bones permit their movement and overlap during labour under the pressure on the fetal head as it passes down the birth canal. This process, called moulding, can decrease the diameters of the fetal skull. The suboccipito-bregmatic diameter is more sensitive to the changes of labour force than other fetal skull diameters [Reference Pu, Xu and Li7]. Significant moulding with caput can be a sign of cephalo-pelvic disproportion, and this should be ruled out before attempting an instrumental vaginal delivery [8].
During early childhood, these sutures harden and the skull bones can no longer move relative to one another, as they can to a small extent in the fetus and newborn.
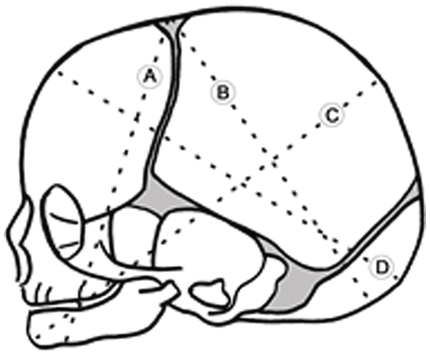
The widest transverse diameter of the fetal skull is the biparietal diameter, which is 9.5 cm. The anteroposterior (AP) diameter of the fetal head is determined by the degree of flexion of the fetal head. This also determines which region of the fetal skull is presenting during labour, and it is described as lines that correspond to the diameter of the presenting region of the head (Figure 1.6).
The fetal skull – showing possible engaging diameters. A) submento-bregmatic (face presentation. B) suboccipito-bregmatic (vertex –well flexed – occipito-anterior position). C) mento-vertical (brow presentation). D) occipito-frontal (vertex deflexed – occipito-posterior/occipito-transverse position).
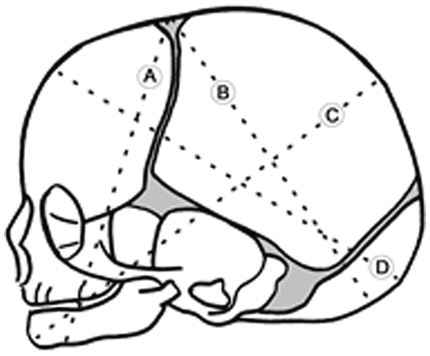
The suboccipito-bregmatic (fully flexed – vertex) and the submento-bregmatic (fully extended – face) are the narrowest AP diameters at 9.5 cm each. The widest AP diameter is 13.5 cm, and is with the extended head which is the mento-vertical of a brow presentation. The occipito-frontal (11.5 cm) diameter is seen with deflexed vertex presentation. Identification of these regions and landmarks on the top of the fetal skull has particular importance for obstetric care when vaginal assessments are made during labour.
The Uterus during Pregnancy
After conception, the uterus provides a nutritive and safe environment for the embryo to develop as a fetus until delivery. The uterus undergoes extensive adaptations mainly with regard to size, shape, position, vasculature and its ability to contract.
Uterine Size
In an uncomplicated pregnancy by term, approximately the weight of the uterus increases 10 to 20-fold (from 70 g to 1000 g) and the volume by 500-fold (10 cc to 5000 cc). This increase of capacity can be expected to accommodate the fetus, placenta and amniotic fluid. Myometrial hypertrophy (an increase in cell size) and accumulation of fibrous and elastic tissue play a major role. Though hyperplasia is limited in humans, the side population of myometrial cells (myoSP) are likely to contribute to the production of new myocytes [Reference Santamaria, Mas, Cervelló, Taylor and Simon9].
Early in gestation, uterine hypertrophy is probably stimulated by the action of mainly oestrogen and also by progesterone. Later in pregnancy hypertrophy of cells of the uterus is in response to the biological mechanical stretching of the uterine walls by the growing fetus and placenta [Reference Shynlova, Kwong and Lye10].
Uterine Shape and Position
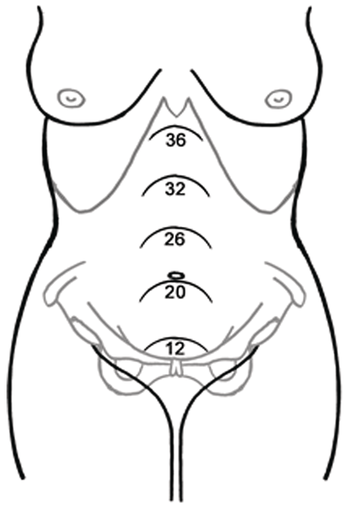
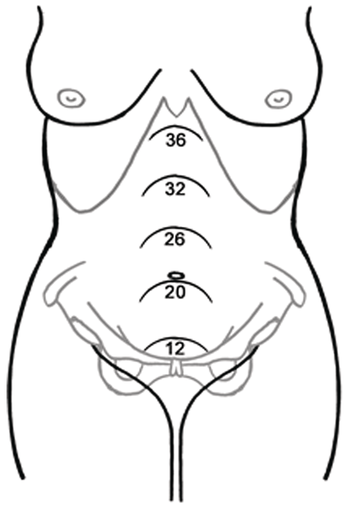
From its original pear shape, the uterus assumes a globular shape as the pregnancy advances. It becomes palpable abdominally by 12 weeks as it is too large to remain totally within the pelvis. From this point onwards it can be measured and palpated as it is in contact with the anterior abdominal wall (Figure 1.7). By term it almost reaches the liver, and this exponential enlargement of the uterus displaces the bowels laterally and superiorly. In supine position it rests on the vertebral column and the adjacent great vessels, especially the inferior vena cava and aorta. It also undergoes dextrorotation, which is likely caused by the recto-sigmoid colon on the left side of the pelvis. As the uterus rises, tension is exerted on the broad and round ligaments.
Height (in cms) of the uterus at various weeks of pregnancy.
Uterine Vascular Adaptations
Spiral artery remodelling, which is accomplished by endovascular trophoblasts during pregnancy, is part of the larger set of adaptive physiological processes required for a successful pregnancy outcome. They are brought about by high oxygen tension in the spiral artery, activation of maternal dNK cells and trapping of maternal platelets by the endovascular trophoblasts [Reference Sato11].
As a result, a multitude of physiological adaptations of the cardiovascular system takes place during pregnancy; the most notable changes are the increase in intravascular volume and cardiac output. Cardiac output increases from 3.5 to 6.0 l/min at rest, a rise of close to 40%. These changes begin as early as the first trimester of pregnancy.
The greatest changes, however, are those occurring in the uteroplacental circulation. Haemochorial placentation in humans results in decreased downstream resistance and secretion of molecular signals. The former results in increased upstream flow velocity and initiates nitric oxide secretion as well as other effects that lead to changes in cell and matrix properties. The combination of vasodilation, changes in matrix enzymes and cellular architecture leads to an increase in lumen diameter without any change in wall thickness, decreased resistance and increased uteroplacental flow [Reference Osol and Moore12]. As a result, an even greater fall in vascular resistance preferentially directs some 20% of total cardiac output to this vascular bed by term, amounting to a 10-fold or greater increase over levels present in the non-pregnant state, such that, by term, uteroplacental flow may approach 1 l/min [Reference Palmer, Zamudio, Coffin, Parker, Stamm and Moore13].
Uterine Contractility
Quiescence of myometrium contractile activity is important to accommodate the growing fetus and prevents preterm labor particularly during uterine stretch. Adaptations of human myometrium during pregnancy include cellular mechanisms that preclude the development of high levels of myosin light chain phosphorylation during contraction and an increase in the stress-generating capacity for any given level of myosin light chain phosphorylation. This process is said to be mediated through Ca2+ [Reference Word, Stull, Casey and Kamm14]. From the first trimester onwards, the uterus undergoes irregular painless contractions that become manually detectable during the mid-trimester. These contractions vary in intensity and timing and are called Braxton Hicks contractions [Reference Hicks15]. Gradually they increase in intensity and frequency during the last week or two and may cause some discomfort late in pregnancy.
Labour contractions are painful and regular. They progressively increase in frequency, duration and intensity, and present with a change in cervical dilation and/or effacement. The primary function of uterine contractions is to expel the fetus from the uterine cavity. Contractions also play an essential role in minimising postpartum haemorrhage.
Length of Pregnancy and Initiation of Labour
Length of Pregnancy
Length of pregnancy in humans averages 40 weeks. Little is known about the factors that determine the length of pregnancy. It is thought to be controlled by events occurring in late pregnancy that influence timing of parturition. Thus, preterm birth is a consequence of premature activation of parturition by a pathological process.
The fetus appears to control the timing of labour at term by coordinating the switch in myometrial activity via placental steroid hormone production and mechanical distension of the uterus, and by secretion of neuro-hypophyseal hormones and other stimulators of prostaglandin synthesis [Reference Norwitz2].
In humans, the timing of birth is associated with the expression of the gene responsible for corticotrophin-releasing hormone (CRH) by the placenta.
Under the influence of oxytocin there is a modification in the coupling mechanisms that leads to a decrease in the biological activity of the CRH receptor and in the generation of cyclic adenosine monophosphate which favours myometrial contractions. CRH, via distinct receptor subtypes, is then able to enhance the contractile response of the myometrium. This hypothesis places CRH in a central role in coordinating the smooth transition from a state of relaxation to one of contraction [Reference Grammatopoulos and Hillhouse16].
Initiation of Labour
During pregnancy, the uterus is maintained in a state of functional quiescence through the integrated action of one or more of a series of inhibitors. It is considered that interaction between maternal endocrine and genetic factors and fetal factors at term removes the mechanisms maintaining uterine quiescence and recruits factors promoting uterine activity.
These multifactorial physiologic events involve an integrated set of changes within the maternal tissues of the uterus (myometrium, decidua and uterine cervix) occurring gradually over a period of days to weeks prior to labour onset. Such changes include, but are not limited to, an increase in prostaglandin synthesis and release within the uterus, an increase in myometrial gap junction formation, and upregulation of myometrial oxytocin receptors [Reference Norwitz2].
Clinical Assessment during Pregnancy and Labour
Clinical assessment of a pregnant woman plays an important role to the obstetrician. It includes the general examination and some specific examinations that are done exclusively in obstetric patients. A systematic examination of the abdomen of a pregnant woman would be with the aim of establishing the symphysio-fundal height, presentation and engagement, lie, position and attitude. Pelvic examination during pregnancy is used to detect a number of clinical conditions such as anatomical abnormalities, to evaluate the size of a woman’s pelvis (pelvimetry) and to assess the uterine cervix. It is usually performed when the woman is thought to be in established labour unless indicated earlier for special reasons.
Abdominal Palpation
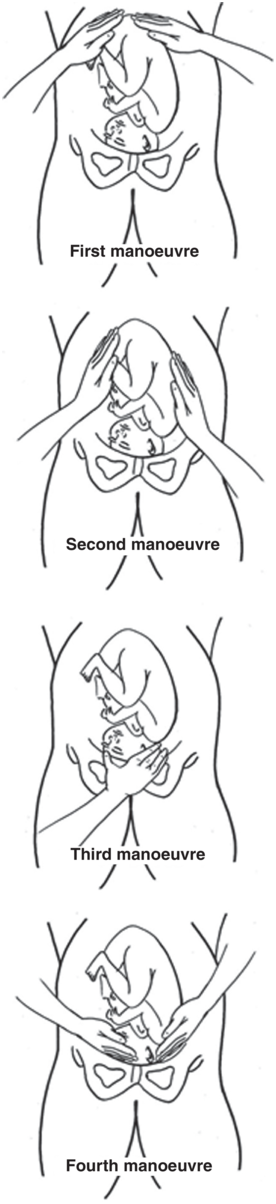
Abdominal examination can be conducted systematically with the aim of establishing the above-mentioned components; employing the four manoeuvres described by Leopold and Sporlinin in 1894 which are even of great value to current practice (Figure 1.8). The mother should be supine and comfortably positioned with her abdomen bared. These manoeuvres may be of limited value and difficult to interpret if the patient is obese, if there is excessive amnionic fluid or if the placenta is anteriorly positioned.
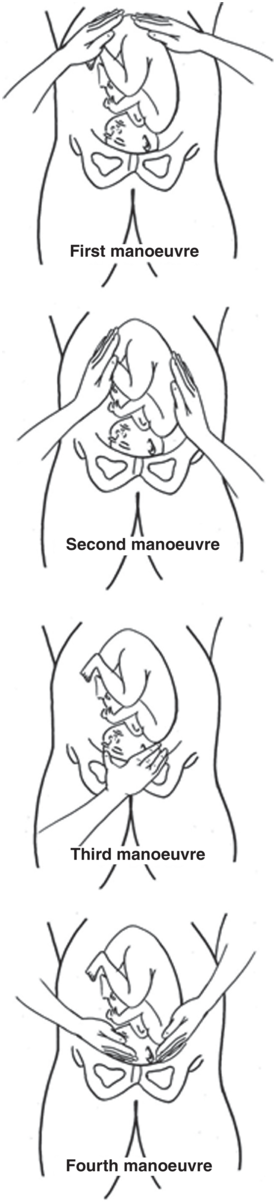
First Manoeuvre: The uterine fundal area is palpated with both hands in order to determine what part of the fetus is occupying the fundus. The breech gives the sensation of a large, nodular mass, whereas the head feels hard and round and is more mobile and ballotable.
Second Manoeuvre: Facing the woman, the abdomen is palpated gently using the palm of the hands placed on either side of the maternal abdomen. The fetal back will feel firm and smooth while fetal extremities feel like small irregularities and protrusions. By noting whether the back is directed anteriorly, transversely or posteriorly, the orientation of the fetus can be determined.
Third Manoeuvre: A gentle grip using the thumb and fingers of one hand are placed on the area over the symphysis pubis to determine what part of the fetus is lying over the pelvic inlet. The differentiation between head and breech is made as in the first manoeuvre and the amount of that presenting part that is palpable abdominally is determined. This manoeuvre may be uncomfortable for the pregnant woman and, if examination is performed in this way, it must be undertaken gently. Alternatively, and in preference, the necessary clinical information may be obtained through the fourth manoeuvre.
Fourth Manoeuvre: The examiner faces the mother’s feet and the fingers of both hands are moved gently down the sides of the uterus towards the pubis to confirm the presentation and on which side is the prominence of the presenting part. The side where the resistance to the descent of the fingers towards the pubis is greatest is where the brow is located. If the head of the fetus is well flexed, it should be on the opposite side from the fetal back. If the fetal head is extended, the occiput is instead felt and is located on the same side as the back.
Abdominal palpation using the above manoeuvres can be performed throughout the latter months of pregnancy and during and between the labour contractions. With experience, fetal malpresentations can be identified with high sensitivity and specificity.
Symphysio-fundal Height
Measurement of symphysio-fundal height is simple, inexpensive and is widely used during antenatal care. It can be achieved more objectively by using a tape measure in centimetres from 24 weeks onwards. When a tape measure is used, the measurement is made by identifying the variable point, the fundus, and then measuring to the fixed point of the top of the symphysis pubis, with the option of centimetre values being hidden by keeping the non-marked side of the tape facing the examiner [17]. This can be used as a screening method for identifying fetuses that are growth restricted, unusually large and for the detection of multiple pregnancies. High detection rates can be achieved if serial measurements are plotted on customised charts for recording with standardised training and protocols to manage the patient [Reference Muhunthan, Abarna, Peratheepa and Shampika18].
Presentation
Fetal presentation refers to the fetal part that directly overlies the pelvic inlet. Any presentation other than cephalic (vertex) is considered malpresentation and by term or 37 completed weeks 96% of pregnancies will have cephalic presentation. Commonest malpresentation at term is breech and its incidence reduces from approximately 20% at 28 weeks to 3–4% at term.
Engagement
Engagement of the fetal head is one of the most important signs for the obstetrician to decide on mode of delivery. Engagement occurs when the widest part of the fetal head passes through the pelvic inlet. Parity, ethnicity, cephalo-pelvic disproportion, malposition and placental location are some of the factors that determine engagement of the fetal head. In different groups of the pregnant population engagement of the fetal head for primigravida and multigravida has been shown to take place at different periods of gestation [Reference Weeks and Flynn19].
Engagement of the fetal head occurs in the majority of nulliparous women prior to labour, but not so for the majority of multiparous women. In nulliparous women, engagement usually takes place from the middle of the third trimester onwards, but in some of these women, and in most multiparous women, engagement may not take place until the onset of labour. Maternal height and birth weight of fetus also may play a significant role in determining the time at which the fetal head engages and need to be considered when assessing a patient [Reference Muhunthan, Abarna, Peratheepa and Shampika18].
Non-engagement at the onset of the active phase of labour is a predictor of the risk of caesarean section, which emphasises the importance of assessing a pregnant woman for engagement of the fetal head, especially when she is in labour [Reference Adeyemi, Adekanle and Afolabi20]. It is customary to describe the amount of the fetal head that is palpable outside the pelvis; when all of the fetal head is palpable above the pelvis it is described as 5/5 (five-fifths palpable). This is based on how many finger breadths are needed to cover the head above the pelvic brim. When the fetal head is engaged, it is usually two-fifths palpable, and when it is deeply engaged it is zero-fifths palpable.
Lie
Fetal lie refers to the long axis of the fetus relative to the longitudinal axis of the uterus. This can be longitudinal, transverse or oblique. Over 99% of singleton term babies have a longitudinal lie and factors such as prematurity, multiparity, multiple pregnancies, placenta praevia, polyhydramnios, uterine fibromatas, congenital uterine anomalies, intrauterine fetal death and extra uterine masses obstructing the birth canal predispose a pregnant woman to have persistent abnormal lie. Compared to those fetuses presenting with a longitudinal lie at the onset of labour, fetuses who are in transverse lie have been found to have a lower absolute pH, more frequent chance of developing severe acidosis, lower birth weight and are more likely to sustain birth trauma and long-term residual effects [Reference Hankins, Hammond, Snyder and Gilstrap21].
Position
Fetal position refers to the relationship of a nominated site of the fetal presenting part (most definable peripheral point in the presentation, e.g. occiput in vertex, sacrum in breech and mentum in face) to a denominating location of maternal pelvis (symphysis pubis anteriorly, sacral promontory posteriorly, sacro iliac joint postero-laterally). For example, in a vertex presentation, the fetal site used for reference is the occiput. In a breech presentation, the sacrum is used as the designated fetal site (e.g. right sacrum anterior). In the vertex presentation any fetal position that is not right occiput anterior, direct occiput anterior or left occiput anterior is referred to as a malposition and fetuses present with a deflexed head and larger engaging diameter and thus a slow labour.
Attitude
Fetal attitude describes the degree of flexion or extension of the fetal head in relation to the fetal spine. Adequate flexion (chin to chest) is necessary to achieve the smallest possible presenting diameter in a cephalic presentation. Deflexion in the early stages of labour corrects spontaneously in most cases by the architecture of the pelvic floor and uterine contractions.
Asynclitism
Asynclitism describes the relationship of the sagittal plane of the fetal head to that of the coronal planes of the symphysis pubis and the sacral promontory. Usually the planes are not parallel and a slight degree of asynclitism is the normal. Significant asynclitism occurs with relative cephalo-pelvic disproportion, as the fetal head rocks on entering the pelvis in an attempt to make progress. If the tilt of the sagittal plane is directed towards the symphysis pubis, then more of the posterior aspect of the fetus’ head is felt vaginally during examination; this is called posterior asynclitism. Anterior asynclitism occurs if more of the anterior part of the fetal head is felt on examination.
Abdominal palpation using the described manoeuvres can be performed throughout the latter months of pregnancy and during and between the labour contractions. On completion of a clinical examination it is usual to summarise the findings in the following order: the symphysio-fundal height; singleton or multiple pregnancy; fetal lie; presentation; and engagement. The fetal heart should be auscultated.
Pelvic Examination
Pelvic examination during pregnancy is used to detect a number of clinical conditions, such as anatomical abnormalities, to evaluate the size of a woman’s pelvis (pelvimetry) and to assess the uterine cervix, but it must be avoided when there is any suspicion of placenta praevia. A sterile speculum examination, allowing visual inspection, is indicated in cases of preterm labour, vaginal bleeding and suspected rupture of membranes. In addition, samples could be obtained for bacteriological tests when indicated.
Clinical Pelvimetry
Assessment of the size of a woman’s pelvis (pelvimetry) can be achieved by clinical examination where the bony pelvis is digitally examined to identify prominent structures that may cause obstructed labour. The aim of pelvimetry in women whose fetuses have a cephalic presentation is to detect the possibility of cephalopelvic disproportion and the need for caesarean section before or during labour. Other imaging techniques like X-rays, CT scanning or MRI are also used to assess the size of the pelvis. One should keep in mind that the dimensions of the pelvis and of the fetal head will change with the dynamics of labour.
During the clinical assessment, the diagonal conjugate is obtained by placing the tip of the middle finger at the sacral promontory and measuring to the point on the hand that contacts the lower border of the symphysis. This is the closest clinical estimate of the obstetric conjugate and is 1.5–2.0 cm longer than the obstetric conjugate. The bi-ischial diameter is the distance between the ischial tuberosities, with a distance greater than 8 cm considered adequate. Other qualitative pelvic characteristics include angulation of the pubic arch (more than 90° or accepts more than two fingers), prominence of the ischial spines, size of the sacrospinous notch (assessed by the sacrospinous ligament at more than three finger breadths) and curvature of the sacrum and coccyx (not being straight). Clinical pelvimetry is not routinely practised in all pregnant women with cephalic presentation, but it is considered a useful tool in certain circumstances.
Cervical Assessment
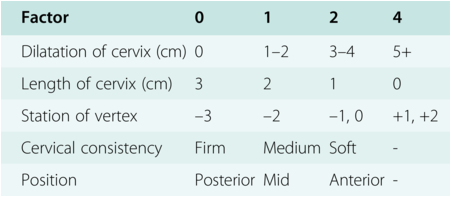
Cervical assessment with a sterile speculum and digital vaginal examination allows the examiner to visually inspect the cervix, obtain samples for bacteriological tests and to assess certain factors of the cervix called Bishop score (Table 1.1).

During the digital vaginal examination, it is customary to start with an assessment of the effacement or cervical length, dilatation, consistency, position and the presentation and station of the presenting part relative to the ischial spines. In the 1960s Edward Bishop developed a pelvic scoring system using these components, which remains the most commonly used system to assess for pre-induction readiness [Reference Baacke and Edwards22].
Expressing the cervical effacement in centimetres rather than percentage is a current modification to the assessment, which is described as ‘modified Bishop score’.
Cervical Effacement
The normal prelabour cervical length is 3–4 cm. The cervix is said to be 50% effaced when it shortens to approximately 2 cm, and fully effaced when there is no length and it is as thin as the adjacent lower segment of the uterus. Effacement is determined by assessing the length of the cervix from the external to the internal os and currently measured in centimetres to minimise the inter-examiner variability. Complete cervical effacement is associated with a characteristic and profound alteration in the gene expression profile of cervical cells. The majority of these genes encode cytokines, transcription factors and cellmatrix-associated proteins [Reference Huber, Hudelist, Czerwenka, Husslein, Kubista and Singer23]. The process of cervical effacement and dilatation differs between primigravida and multiparous patients. In the latter, effacement and dilatation occur simultaneously, while in the case of primigravidae, effacement precedes dilatation.
Cervical Dilatation
During labour the cervix dilates progressively and the primary factors leading to cervical dilatation are the traction forces of the myometrial contractions, and the pressure of the fetal head or the presenting part on the cervix. From full effacement and 4 cm dilatation to full dilatation or 10 cm, the cervix usually dilates at a rate of 1 cm per hour.
Cervical Position
Cervical position describes the location of the cervix in relation to the maternal pelvis. During labour, the position progresses from posterior to mid-position and then to anterior.
Cervical Consistency
Cervical consistency ranges from firm to soft. Cervical softening during pregnancy is a unique phase of the tissue remodelling process characterised by increased collagen solubility, maintenance of tissue strength and upregulation of genes involved in mucosal protection [Reference Read, Word, Ruscheinsky, Timmons and Mahendroo24]. During this process, the junction between the fetal membranes and the decidua breaks down, and an adhesive protein – fetal fibronectin – enters vaginal fluids. This is a clinically useful predictor of imminent labour [Reference Smith25].
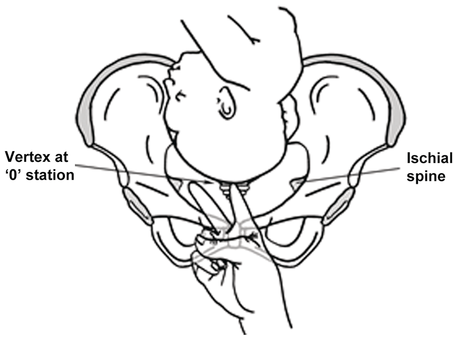
The Station
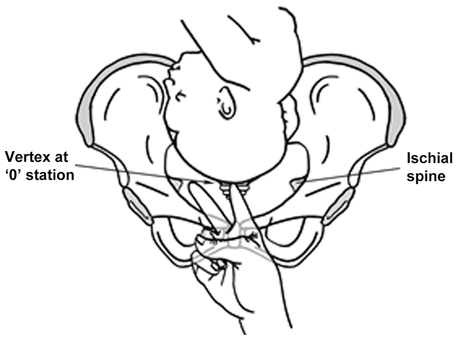
The station of the presenting part describes the distance of the leading bony part of the fetal head relative to the ischial spines. The usual method is to measure the distance above and below the spines in centimetres, with the areas above being given a minus sign and those below the spines being given a positive sign. For example, ‘0’ indicates that the lowest part of the fetal head is at the level of the ischial spines, while ‘+1’ indicates that the head is 1 cm below the level of the spines (Figure 1.9).
Clinical assessment of the station of the presenting part.
Identifying the position of the presenting part is accomplished by identifying the bony sutures of the fetal head, following the suture until it leads to a fontanelle and then identifying the sutures radiating from it. Provided the head is low and the patient has good pain relief, it may also be possible to locate the ear of the fetus and to assess to which side it faces. The nose and mouth can usually be identified in a face presentation, while the sacrum, genitalia and anus should be identifiable with a breech presentation.
At the end of the examination the following should be described and noted: inspection of vulva and vagina to ascertain/establish the presence or absence of any liquor, blood or discharge; and palpation of the cervix to establish its length, thickness and position (anterior, mid-position or posterior). In the active stage of labour, the clinician assesses the progress of cervical dilatation, and effacement, the station and position of the presenting part and whether there is any asynclitism, caput succedaneum and moulding.
Stages and Duration of Normal Labour
Although labour is a continuous process, it is divided into three stages to facilitate monitoring and to assist in clinical management.
First Stage
The first stage is said to begin with the onset of regular painful uterine contractions resulting in cervical changes, and ends when the cervix is fully dilated at 10 cm. It has been further subdivided into latent and active phases according to the rates of cervical dilatation [Reference Friedman26]. The latent phase is defined as the period of time, not necessarily continuous, when there may be painful contractions as well as cervical change, including cervical effacement and with cervical dilatation up to 4 cm. It is characterised by slow cervical dilatation and is of variable duration. The established, active phase of the first stage of labour begins when there are regular painful contractions and there is progressive cervical dilatation from full effacement and 4 cm dilatation onwards. The length of the labour duration or curve does not differ among ethnic or racial groups, but there are significant differences between nulliparous and multiparous women [Reference Duignan, Studd and Hughes27]. The length of the active first stage of labour in nulliparous women is on average 8 hours and is unlikely to be over 18 hours. Second and subsequent labours last on average 5 hours and are unlikely to last more than 12 hours [28].
By comparing a labouring woman’s rate of cervical dilatation with the normal profile described by Friedman, it is possible to detect abnormal labour patterns and identify pregnancies at risk for adverse events [Reference Friedman26]. This task can be facilitated by use of a partogram, which is a graphic representation of the labour progress curve against which a patient’s progress in labour is plotted. In this way, abnormal labour patterns can be identified easily and appropriate measures taken.
Second Stage
The second stage starts when the cervix is fully dilated at 10 cm and is characterised by descent of the presenting part through the maternal pelvis. It ends with the delivery of the fetus. It is characterised by an increase in bloody show, maternal desire to bear down with each contraction and a feeling of pressure on the rectum accompanied by the desire to defecate.
The safe duration desirable for the initial passive second stage of labour for a nulliparous may be up to 2 hours and an hour longer when a woman has an epidural in place. For a multiparous woman the duration is 1 hour and 2 hours, respectively. The onset of the active second stage of labour is when the baby is visible or there is involuntary or active pushing with full dilatation of the cervix [28].
Third Stage
The third stage of labour refers to the time from delivery of the fetus to separation and expulsion of the placenta and fetal membranes. It is characterised by signs of placental separation, namely lengthening of the umbilical cord, a gush of blood from the vagina, which signifies separation of the placenta from the uterine wall, and a change in the shape of the uterine fundus from discoid to globular, with elevation of the fundal height (and lengthening of the umbilical cord at the vaginal introitus). Though there are no uniform criteria for the normal length of the third stage of labour, it is diagnosed as prolonged if not completed within 30 minutes of the birth of the baby with active management, and 60 minutes with physiological management [28].
Mechanism of Labour
During the passages of the fetal head through the bony pelvis or birth canal, it adopts a series of changes which are traditionally described as cardinal movements which culminate with the delivery of the fetal head. Because of asymmetry in the shape of the fetal head and the maternal bony pelvis, such movements are required if the fetus is to negotiate the birth canal successfully. At least seven discrete movements are worth considering, which are engagement, descent, flexion, internal rotation, extension, external rotation or restitution, and expulsion.
This is followed by the delivery of the shoulders and the body of the fetus.
Engagement
Engagement occurs when the fetal head is engaged, that is, when its maximum diameters (suboccipito-bregmatic and biparietal, when the head is well flexed) have passed the pelvic inlet. On engagement, the biparietal diameter lies at the level of the true conjugate and the vertex is 1 cm above the ischial spines. In the breech presentation, the widest diameter is the bi-trochanteric diameter. Engagement can be confirmed clinically by palpation of the presenting part abdominally when only two-fifths of the head can be palpated, or vaginally, with confirmation of station at or below the ischial spines. Parity, maternal age, height and birth weight of fetus play a significant role in determining the time at which the fetal head engages, and need to be considered when assessing a patient [Reference Adeyemi, Adekanle and Afolabi20].
Descent
This is the downward movement of the fetal head or the presenting part in the pelvis. Descent with vertex presentation is described by the number of fifths of the head still palpable above the pelvis, and by the station (the relative position of the presenting part to the ischial spines).
Descent of the fetus is not a steady, continuous process and usually starts in the late first stage and continues through the second stage. Descent is usually brought about by uterine contractions and is aided in the second stage of labour by maternal bearing down effort.
Flexion
Flexion of the fetal head initially occurs passively as the head descends. This is facilitated by the shape of the bony pelvis and the resistance of the lower segment of the uterus, the pelvic side wall and downward medially sloping muscular levatores ani pelvic floor. Although some degree of flexion is present in most fetuses antepartum, complete flexion usually occurs during the course of labour as the uterus contracts and the pressure is conveyed via the vertebral column to the occipital part of the vertex that is on the downward and medially sloping pelvic floor. With the head completely flexed, the fetal chin coming into contact with the fetal chest, the fetus presents the smallest diameter of its head (suboccipito-bregmatic diameter 9.5 cm and biparietal 9.5 cm), which allows optimal passage through the birth canal.
Internal Rotation
Internal rotation is the rotation of the fetal head from its usual transverse position to the AP position as it passes through the pelvis. Typically in more than 95% of term labours this results in the fetal occiput rotating towards the symphysis pubis as it descends, which leads to the optimal diameter of the fetal head facing the widest axis of the pelvic passage. The fetal head initially descends in an asynclitic fashion, but it typically corrects itself as the head descends further (due to the curvature of the maternal sacrum). As with flexion, internal rotation is a passive movement that results from the shape of the pelvis and the resistance of the pelvic floor musculature.
Extension
As the fetal head descends to the level of the pelvic outlet, the base of the occiput will come into contact with the inferior margin of the symphysis pubis where the birth canal curves upward and forward. The head is delivered through the maternal vaginal introitus by extension from the flexed position. First to deliver is the occiput, then with further extension the vertex, bregma, forehead, nose, mouth and finally the chin. The forces responsible for this motion are the propulsive force exerted on the fetus by uterine contractions and maternal expulsive efforts, along with the upward forces exerted by the muscles of the pelvic floor.
External Rotation (Restitution)
Having delivered with the sagittal suture vertical (AP) and the occiput anterior, the delivered fetal head returns to the position it occupied in the vagina. For example, if the position was left occipito-anterior, the head will ‘restitute’ to the left. This is followed by complete rotation of the sagittal suture to the transverse position so that the shoulders align in the antero-posterior diameter of the pelvic outlet, so facilitating their passage (i.e. one shoulder will lie behind the symphysis pubis, the other will be posterior, in front of the sacral promontory). This is again a passive movement that results from a release of the forces exerted on the fetal head by the maternal bony pelvis and its musculature, and it is mediated by the basal tone of the fetal musculature.
Expulsion
Expulsion refers to delivery of the body of the fetus. After delivery of the head and external rotation (restitution), further descent brings the anterior shoulder to the level of the symphysis pubis. The anterior shoulder rotates under the symphysis pubis, after which the rest of the body usually delivers without difficulty.
Maternal Position and Pushing in Labour
As lying flat on the woman’s back can lead to a decrease in blood pressure due to compression of inferior vena cava and may reduce placental blood flow, women are encouraged to avoid this position.
Lying on the woman’s side increases the chance of a spontaneous vaginal birth, but she can use any other position she finds comfortable to give birth, including upright positions [28]. Though the cardinal movements are largely the result of uterine contractions, the passive action of the pelvic musculature and the descending fetal head, maternal pushing, especially during the second stage, assists in achieving vaginal delivery. Spontaneous pushing when a woman is labouring without epidural anaesthesia and directed pushing while on epidural anaesthesia are said to shorten the second stage of labour. These practices facilitate or speed delivery, though their contribution to increasing the intrauterine pressure is said to be small [Reference Buhimschi, Buhimschi, Malinow, Kopelman and Weiner29]. The clinical significance of shortening of the duration of the second stage of labour is uncertain with active pushing, but supporting spontaneous pushing and encouraging women to choose their own method of pushing should be accepted as best clinical practice [Reference Prins, Boxem, Lucas and Hutton30].