

Highlights
-
• Canadian FTD caregivers face long diagnostic journeys, with frequent misdiagnoses and major barriers related to low awareness and limited access to specialized care.
-
• Caregivers report substantial burden and high distress, strongly driven by neuropsychiatric symptom.
-
• Young-onset cases, absence of family history and misdiagnosis significantly delay diagnosis.
Introduction
Frontotemporal dementia (FTD) and related disorders are the second most common neurodegenerative causes of young-onset dementia (YOD) after Alzheimer’s disease (AD) and the third most common neurodegenerative causes of dementia overall, after AD and Lewy body dementia (LBD). Reference Olney, Spina and Miller1–Reference Sivasathiaseelan, Marshall and Agustus3 Although the prevalence of FTD in Canada is not precisely known, it is estimated to account for 1.7–7% of all dementia cases. Reference Leroy, Bertoux and Skrobala4,Reference Hogan, Jetté and Fiest5 With the number of Canadians living with dementia projected to reach one million by 2030, the impact of FTD is likely to grow. This burden is particularly substantial as FTD typically affects people under the age of 65, striking during prime working years and placing added strain on families, the workforce, and the healthcare system. 6,Reference Novek and Menec7 Clinically, FTD encompasses behavioural variant FTD (bvFTD), primary progressive aphasia (PPA), corticobasal syndrome (CBS), progressive supranuclear palsy (PSP) and FTD associated with amyotrophic lateral sclerosis (FTD-ALS). Reference Desmarais, Rohrer and Nguyen8,Reference Tartaglia and Mackenzie9 Their various manifestations – ranging from profound behavioural and neuropsychiatric symptoms (NPS) to language and motor impairments – often overlap with those of psychiatric disorders and other more common dementias. Reference Olney, Spina and Miller1,Reference Ducharme, Price, Larvie, Dougherty and Dickerson10,Reference Erkkinen, Kim and Geschwind11 The absence of widely available biomarkers, along with substantial clinical and pathological heterogeneity, makes accurate diagnosis challenging. Misdiagnosis is common, with 33% to up to 50% of patients initially given another diagnosis, such as psychiatric disorders and AD. Reference Ducharme, Price, Larvie, Dougherty and Dickerson10,Reference Beber and Chaves12–Reference Barker, Dodge and Niehoff14
For individuals living with FTD, the disease invariably leads to progressive loss of independence over time, with rate of decline depending on subtype. Reference Galvin, Howard, Denny, Dickinson and Tatton15 Families and caregivers shoulder most of the care burden. Compared with caregivers of individuals with AD or LBD, those supporting people with FTD consistently report higher levels of distress, Reference Cheng16,Reference Lima-Silva, Bahia and Carvalho17 potentially driven by delays in obtaining an accurate diagnosis, high rates of behavioural disturbances such as agitation and disinhibition, limited access to specialized care and community resources, and the lack of effective pharmacologic treatments. Reference Desmarais, Rohrer and Nguyen8,Reference Cheng16–Reference Desmarais, Lanctôt and Masellis20 These challenges make delivering optimal care for FTD particularly complex. Reference Boxer, Gold and Feldman21 Despite the recognized difficulties, little is known about the specific journey of Canadian caregivers navigating the healthcare system for an individual with FTD. Understanding barriers to diagnosis and care is critical to improve health system responsiveness, reduce caregiver distress, and support equitable, high-quality dementia care. The primary objectives of this study were to describe the profiles and experiences of caregivers of individuals with FTD, and to characterize their journey to obtaining a diagnosis and accessing care within the Canadian healthcare system, including factors associated with delayed diagnosis and higher burden. The secondary objective was to examine the influence of sex and gender on the caregiving and disease experience, recognizing that differences in caregiving roles, expectations, perceptions, and health system interactions may shape both the journey to diagnosis, needs, and access to care.
Methods
Study design
We conducted a cross-sectional online survey to characterize the experiences of individuals providing informal care to people living with FTD and related disorders across Canada. The survey aimed to depict caregivers’ and care recipients’ sociodemographic profiles, their experiences seeking a diagnosis and accessing health and community care. The study also included a parallel arm for healthcare providers; however, the present paper reports only on responses from caregivers. The study followed the Checklist for Reporting Results of Internet E-Surveys Reference Eysenbach22 and the STROBE statement for cross-sectional studies. Reference von Elm, Altman and Egger23
Participant eligibility and recruitment
Eligible participants were self-identified informal caregivers – defined as adults (≥18 years) who were currently providing, or had provided recently (i.e., within the past year), unpaid care for a person diagnosed with FTD or a related disorder. Care recipients of participants were required to have received a diagnosis of bvFTD, PPA, PSP, CBS, or FTD-ALS, and to have undergone assessment and care within the Canadian healthcare system. Informal caregivers could include spouses, family members, or friends.
Participants were recruited through multiple channels: (1) an open survey link posted on the Find a Research Study page of the Alzheimer Society of Canada website and on the Studies Seeking Participants page of the Association for Frontotemporal Degeneration website; (2) invitations and reminders sent to memory clinics across Canada, who distributed the survey link to their patients and families; and (3) targeted advertisements via newsletters, provincial and national associations, social media, and flyers provided to healthcare providers for distribution to caregivers. Participation was voluntary, informed consent was required and obtained by having respondents providing online consent prior to beginning the survey, and no incentives were offered.
Survey development and data collection
The survey was developed by a multidisciplinary team of clinicians and researchers with expertise in dementia diagnosis and care, in consultation with individuals with lived caregiving experience. It was pilot tested with diverse stakeholders, notably older adults and caregivers, to ensure clarity, readability, accessibility, and content validity. The final version was hosted on the SurveyMonkey© platform and was available in English and French between June 1, 2023, and May 31, 2024.
The survey included five fixed sections with both closed- and open-ended questions (See Supplementary Material): 1. Caregiver characteristics (e.g., age, sex [i.e., assigned sex at birth – biological variable], gender [i.e., self-reported gender – psychosocial variable], relationship to care recipient, region of residence); 2. Care recipient characteristics (e.g., age, sex, gender, specific diagnosis, disease duration [estimated in years], level of functional independence); 3. Diagnostic journey and access to care (e.g., initial manifestations, time to diagnosis [TTD – estimated in months], number of clinical visits, prior diagnoses received, perceived barriers, current and needed community services); 4. Caregiver burden and associated factors, assessed using the 12-item Zarit Burden Interview (ZBI-12 – which quantifies subjective burden experienced by caregivers of individuals with chronic health conditions) Reference Gratão, Brigola and Ottaviani24 and supplemented by the Neuropsychiatric Inventory (NPI) Reference Cummings, Mega, Gray, Rosenberg-Thompson, Carusi and Gornbein25 to evaluate the frequency ([F]; from 0 to 4) and severity ([S]; from 1 to 3) of 12 common NPS in care recipients, as well as their repercussion on the caregiver (i.e., distress [D]; from 0 to 5); and 5. Research participation and opportunities. Functional status of care recipients was assessed using the Katz Index of Activities of Daily Living Reference Katz, Downs, Cash and Grotz26 and Instrumental Activities of Daily Living scales. Reference Katz27 Respondents were not obliged to answer every question; sensitive questions were clearly identified, and definitions and examples accompanied technical terms to improve comprehension and minimize missing data. All responses were collected anonymously. IP addresses, time stamps, and session identifiers were used only to ensure data integrity and prevent duplicate submissions.
Data analysis
Three investigators (AM, MC and PD) independently reviewed, cleaned and verified the dataset. Duplicate entries and implausible aberrant values were removed; extreme outliers were winsorized where possible. Respondents were excluded if they (1) did not provide consent, (2) did not identify themselves as caregivers or (3) reported providing care to someone with a diagnosis other than a FTD or related disorder. Partially completed surveys were retained in the analyses if core eligibility criteria were met and core outcome data were available. To portray the profiles and experiences of caregivers and care recipients, including level of burden and presence of NPS, descriptive statistics were calculated, using means and standard deviations (SD) for continuous variables and counts and percentages for categorical variables. For NPS, we reported the prevalence of clinically significant symptoms, defined a priori as those with a frequency and severity [F × S] product of ≥4 points. Reference Eikelboom, van den Berg and Singleton28
To identify factors associated with delayed diagnosis, we conducted univariate analyses examining caregiver and care recipient characteristics in relation to TTD (i.e., interval of time from first initial manifestations to final FTD diagnosis). Mean differences, in months, with 95% confidence intervals (CI) were calculated according to the presence or absence of specific biopsychosocial characteristics. To assess the contribution of NPS in FTD to caregiver burden, we first conducted bivariate analyses to explore associations between the ZBI score and explanatory variables. We then conducted multivariable linear regression models with the ZBI as the dependent variable. Independent variables included the NPI total score, NPI-D total score and the individual symptom domain scores [F × S], while adjusting for caregiver’s age and gender, and disease duration.
To highlight noteworthy differences according to caregiver and care recipient’s sex and gender, we repeated descriptive statistics and analyses accordingly and reported disaggregated results (see Supplementary Data). For uniformity, as all the respondents identified themselves as cisgender and that caregiving is predominantly a psychosocial experience, we reported our findings according to gender, but highlighted in the interpretation of findings when sex, gender or both were believed to be at play. Statistical significance was set at two-tailed p < 0.05. All analyses were performed using IBM SPSS Statistics, version 31.0. Reference Corp29
Engagement of people with lived experience
Meaningful engagement of people with lived experience was embedded throughout the study in alignment with the Canadian Institutes of Health Research Strategy for Patient-Oriented Research principles, which emphasize inclusiveness, support, mutual respect and co-building in health research. Our research team collaborated with the Canadian Consortium on Neurodegeneration in Aging (CCNA)’s Engagement of People with Lived Experience of Dementia (EPLED) Advisory Group and Program. EPLED provides structured mechanisms for involving individuals living with dementia, caregivers and healthcare system users in all stages of research. Following data collection, preliminary survey findings were presented in three dedicated virtual meetings to the EPLED Advisory Group members, including those with a diagnosis of dementia and caregivers. Their input contextualized and enriched interpretation of both quantitative and qualitative results, ensuring analyses and findings reflected the lived realities of caregiving (e.g., healthcare navigation, daily tasks). This iterative process allowed to refine analysis, highlight priorities for caregivers and identify implications for policy and practice most relevant to improving quality of care and health system responsiveness.
Ethics approval
The study was approved by CHUM Research Ethics Board (Approval 22.271, 23.05.2023).
Results
Survey caregivers and care recipients
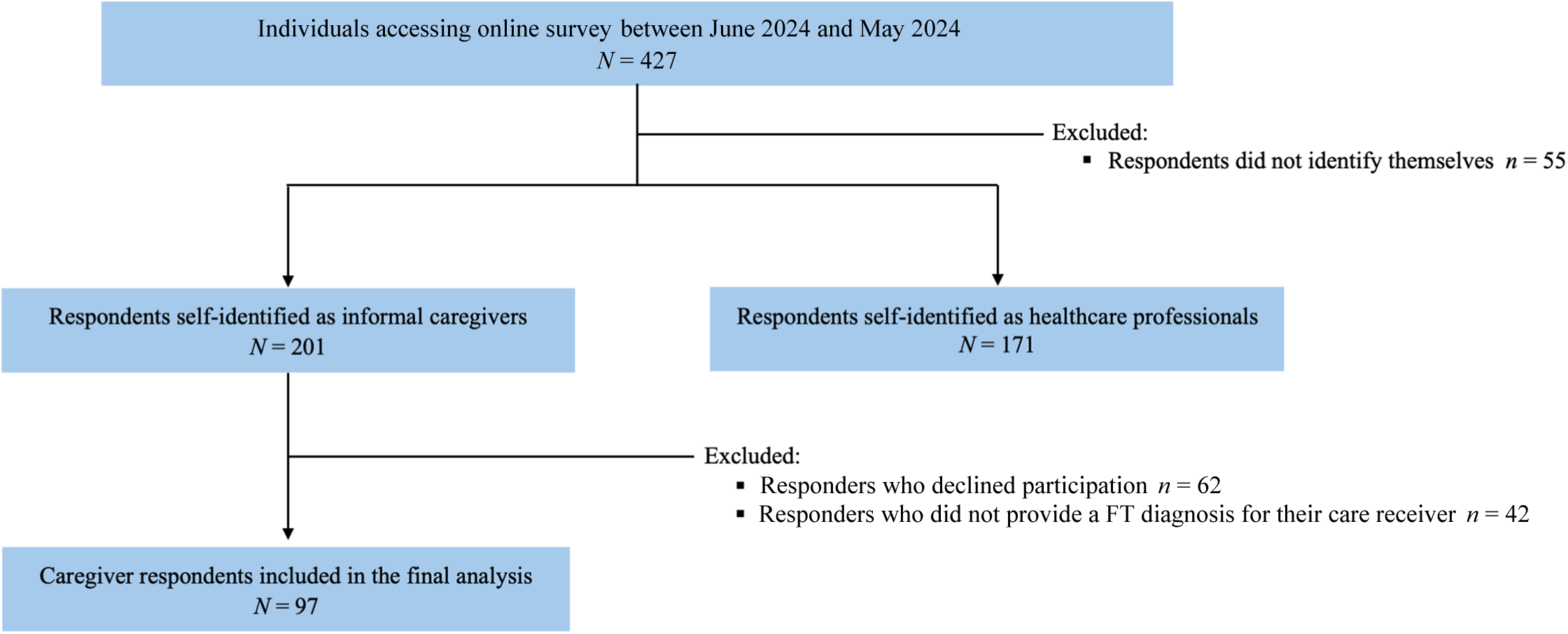
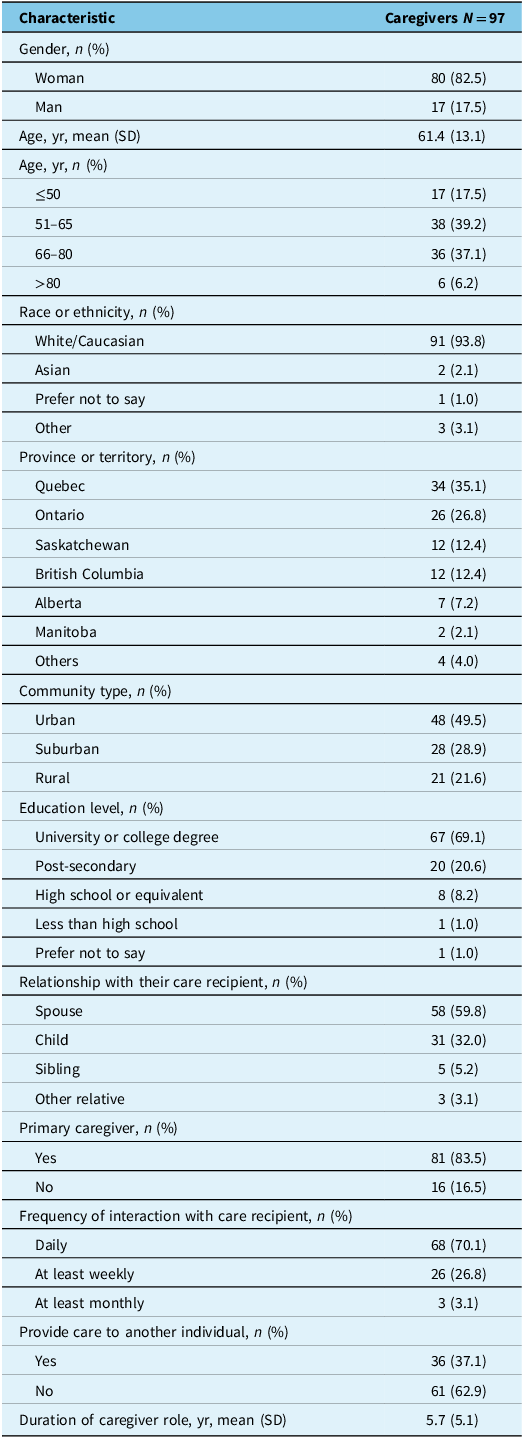
Between June 1st, 2023, and May 31st, 2024, the online survey was accessed 427 times. A total of 97 responders self-identified as a caregiver to an individual with FTD and were included in the analysis (Figure 1). Responses were obtained across all Canadian provinces, with most respondents from Quebec (35.1%) and Ontario (26.8%) (Table 1). Most respondents identified themselves as the primary caregiver of the individual with FTD (83.5%), were white/Caucasian (93.8%), women (82.5%) and in a spousal relationship (59.8%). Caregivers were on average 61.4 years old (SD = 13.1), mostly university or college educated (69.1%), and from urban communities (49.5%). On average, they were in a caregiving role for the past 5.7 years (SD = 5.1) and maintained daily contact (70.1%) with their care recipient. More than a third of caregivers (37.1%) reported providing care to another individual in addition to the individual with FTD (Table 1); most often a parent (34.2%) or a child (34.2%). Men respondents were predominantly the spouse of the care recipients (70.6%) comparatively to women respondents (57.5%) (Supplementary Data).
Selection of study population. FTD = Frontotemporal dementia.

Characteristics of caregiver respondents of the Canadian FTD Survey

FTD = frontotemporal dementia.
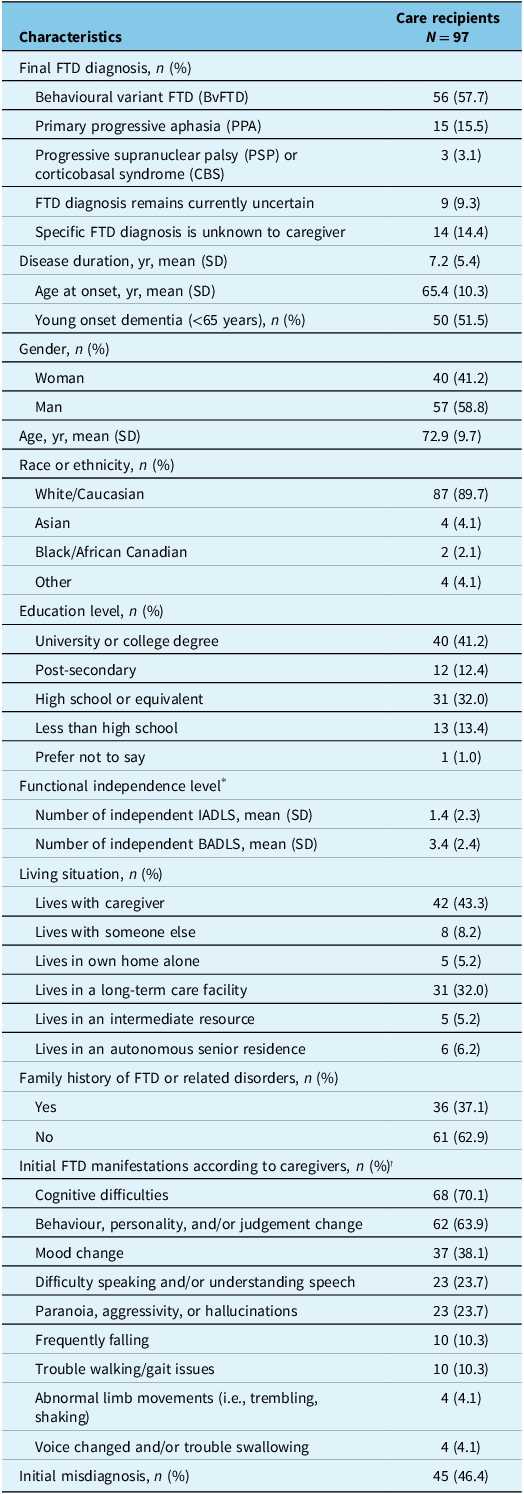
Care recipients were mainly white/Caucasian (89.7%), men (58.8%), with an average age of 72.9 years old (SD = 9.7) (Table 2). Most had a university/college (41.2%) education and lived either with their caregiver at home (43.3%) or in a long-term care (LTC) facility (32.0%). Among care recipients, 61.4% of men lived at home with their caregiver, compared to 17.5% of women (p < 0.001). The most common specific diagnoses of FTD were bvFTD (57.7%) and PPA (15.5%). A significant proportion of caregivers did not know the specific FTD subtype diagnosis of their loved one (14.4%) or reported that the specific clinical diagnosis was still uncertain (9.3%).
Characteristics of care recipients of the Canadian FTD Survey

BADLS = basic instrumental activities of daily living; FTD = frontotemporal dementia; IADLS = instrumental activities of daily living.
* Only 94 respondents answered all the items for the functional independence scales.
† Respondents could check all that applied.
Journey to diagnosis
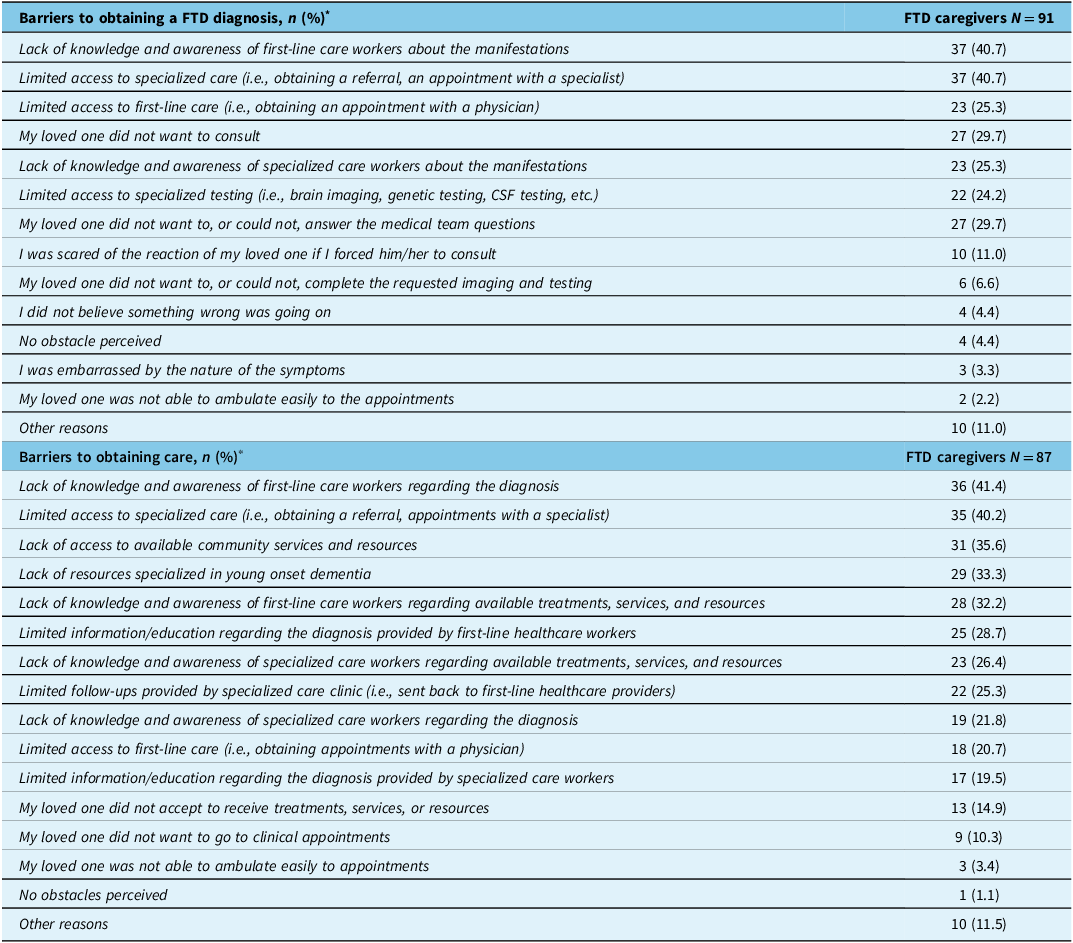
Respondents identified cognitive difficulties (70.1%), behaviour, personality and/or judgement change (63.9%), and mood change (38.1%) as the most common initial manifestations of their care recipients with FTD (Table 2). Mood as a common initial manifestation was more frequently reported for women than men care recipients (50% vs. 29.8%, p = 0.049), while language difficulties were more frequently reported for men than women recipients (31.6% vs. 12.5%, p = 0.022) (Supplementary Data). Caregivers reported that their care recipients had been symptomatic on average for 7.2 years (SD = 5.4), with a mean age at onset of 65.4 years (SD = 10.3), ranging from 44 years to 87 years (5 cases [5.3%] ≤50 years; 27 cases [28.7%] 51 to 60 years; 33 cases [35.1%] 61 to 70 years; 21 cases [22.3%] 71 to 80 years; 8 cases [8.5%] >80 years). About half of care recipients (51.5%) had YOD. Mean TTD was 3.1 years (SD = 4.5), with a mean number of clinical visits of 6.9 (SD = 8.6), and a mean number of 2.9 (SD = 1.6) different physicians consulted prior to receiving a diagnosis of FTD. A different diagnosis prior to FTD was reported by 46.4% of respondents; most often a psychiatric disorder (35.6%) or AD (22.2%). Among initially received diagnoses, respondents specified bipolar disorder, personality disorder, gambling addiction, attention and hyperactive disorder, post-traumatic stress disorder and obsessive-control disorder. Most respondents reported that their care recipient’s diagnosis changed at least once during follow-ups (53.6%). Before care recipients obtained a final FTD diagnosis, 64 cases (65.9%) underwent brain MRI, 46 cases (47.4%) brain FDG-PET-scan or SPECT-scan, 9 cases (9.3%) lumbar puncture and 15 cases (15.5%) EMG testing. In total, 83 cases (85.5%) received their final FTD diagnosis from a specialist, while 14 cases (14.4%) were diagnosed by their primary care physician. Care recipient’s diagnosis was supported by genetic testing in 36 cases (37.1%). Most frequently reported barriers to diagnosis by respondents included lack of knowledge and awareness of first-line workers about the disorder (41.8%), limited access to specialized care (40.7%), and their care recipient not wanting to consult (29.7%) (Table 3).
Identified barriers by caregivers in their healthcare journey

* Respondents could check all that applied.
FTD = frontotemporal dementia.
Journey to receiving care
Most frequently reported barriers to obtaining care for their care recipients included lack of knowledge and awareness of first-line care workers regarding the diagnosis (41.4%), limited access to specialized care (40.2%), lack of access to available community services and resources (35.6%) and lack of resources specialized in YOD (33.3%) (Table 3). A third of caregivers identified that their care recipient was receiving more than one care service (32.6%); with the most common services being adult day programme services (18.9%), home support from companionship services (17.9%) and occupational therapy (12.6%). Additionally, 43.2% of caregivers mentioned having required private (i.e., paid) services to complete available community services and that 63.9% of caregivers reported that the medical and psychological resources did not meet or only partly met the needs for their care recipient. Over the past year, among respondents, 21.6% reported their care recipient visited the hospital emergency room (ER), and 16.7% were hospitalized because of FTD manifestations. Furthermore, 22.5% of care recipients were relocated, while 31.8% were prescribed new medications to prevent an ER visit.
Factors associated with delayed diagnosis
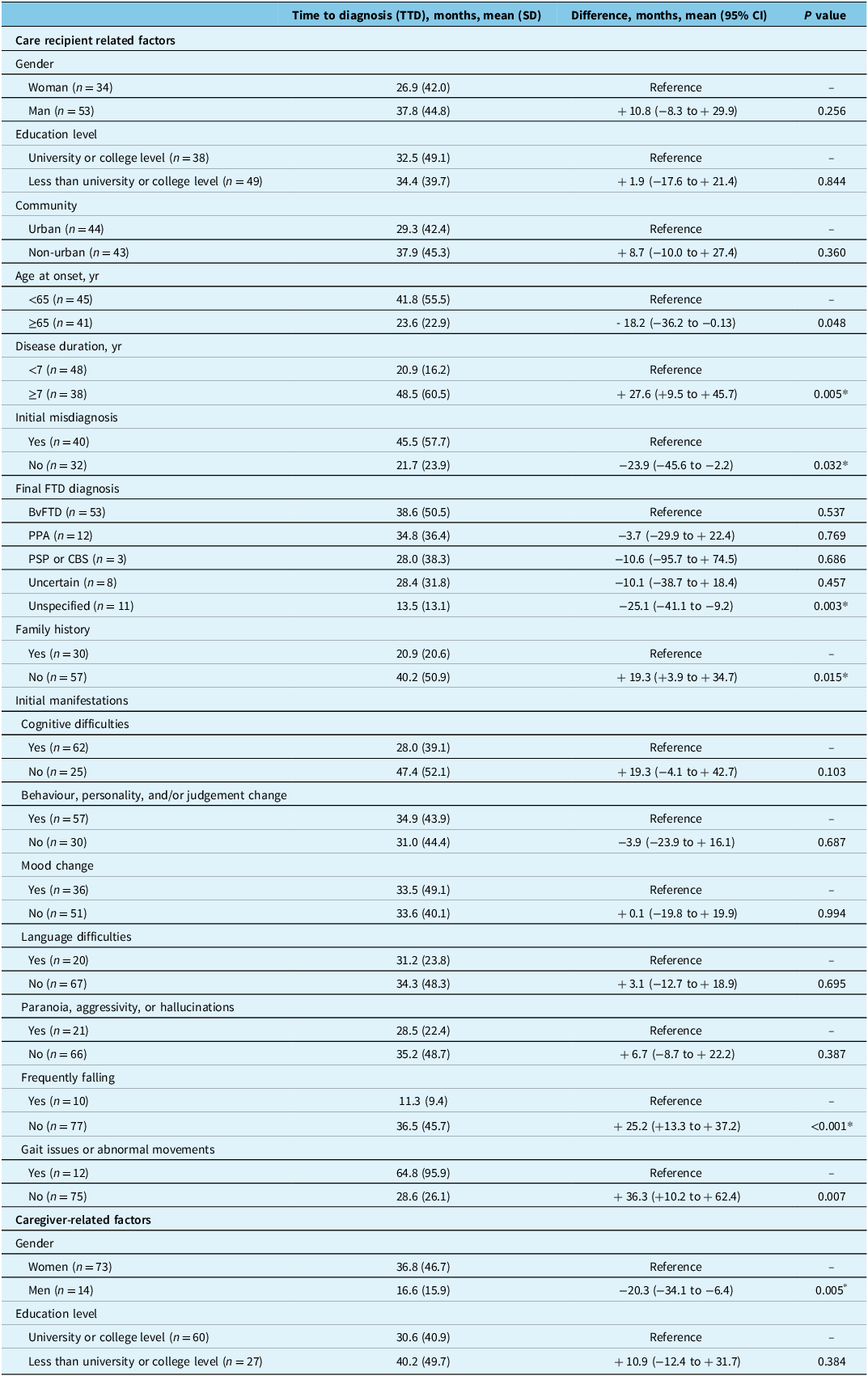
Table 4 reports analyses on average time to final FTD diagnosis from onset of initial manifestations according to caregiver and care recipient characteristics. Individuals with YOD were on average diagnosed 18.2 months later than individuals with an age at onset of ≥65 years (p = 0.048) and individuals with no family history of FTD were on average diagnosed 19.3 months later than those with a positive family history (p = 0.015). More recent cases of FTD (i.e., disease duration <7 years) obtained a diagnosis on average 27.6 months sooner than those that have been progressing longer (p = 0.005). Initially misdiagnosed cases received a final FTD diagnosis on average 23.9 months later (p = 0.032). While the differences were not statistically significant, average TTD was longer for men than women (37.8 months [SD = 44.8] vs. 26.9 months [SD = 42.0], respectively, p = 0.256) and longer for non-urban care recipients than urban care recipients (37.9 months [SD = 45.3] vs. 29.3 months [SD = 42.4], respectively, p = 0.360). Care recipients who presented initially with frequent falls or with gait/abnormal movements at onset of dementia were on average diagnosed 25.2 months and 36.3 months sooner than those without these early manifestations (p < 0.001 and p = 0.007, respectively). Women caregivers reported on average significantly longer TTD than men caregivers (+20.3 months, p = 0.005). In the sensitivity analysis where extreme values and PSP/CBS cases were removed, differences remained statistically significant for disease duration, initial misdiagnosis, family history, falls and caregiver’s gender (see Supplementary Data).
Care recipient and caregiver characteristics association with time to diagnosis

* In sensitivity analysis, these differences remained statistically significant after removing extreme values (see Supplementary Data).
BvFTD = behavioural variant frontotemporal dementia; CBS = corticobasal syndrome; FTD = frontotemporal dementia; PPA = primary progressive aphasia; PSP = progressive supranuclear palsy.
Caregiver burden and neuropsychiatric symptoms
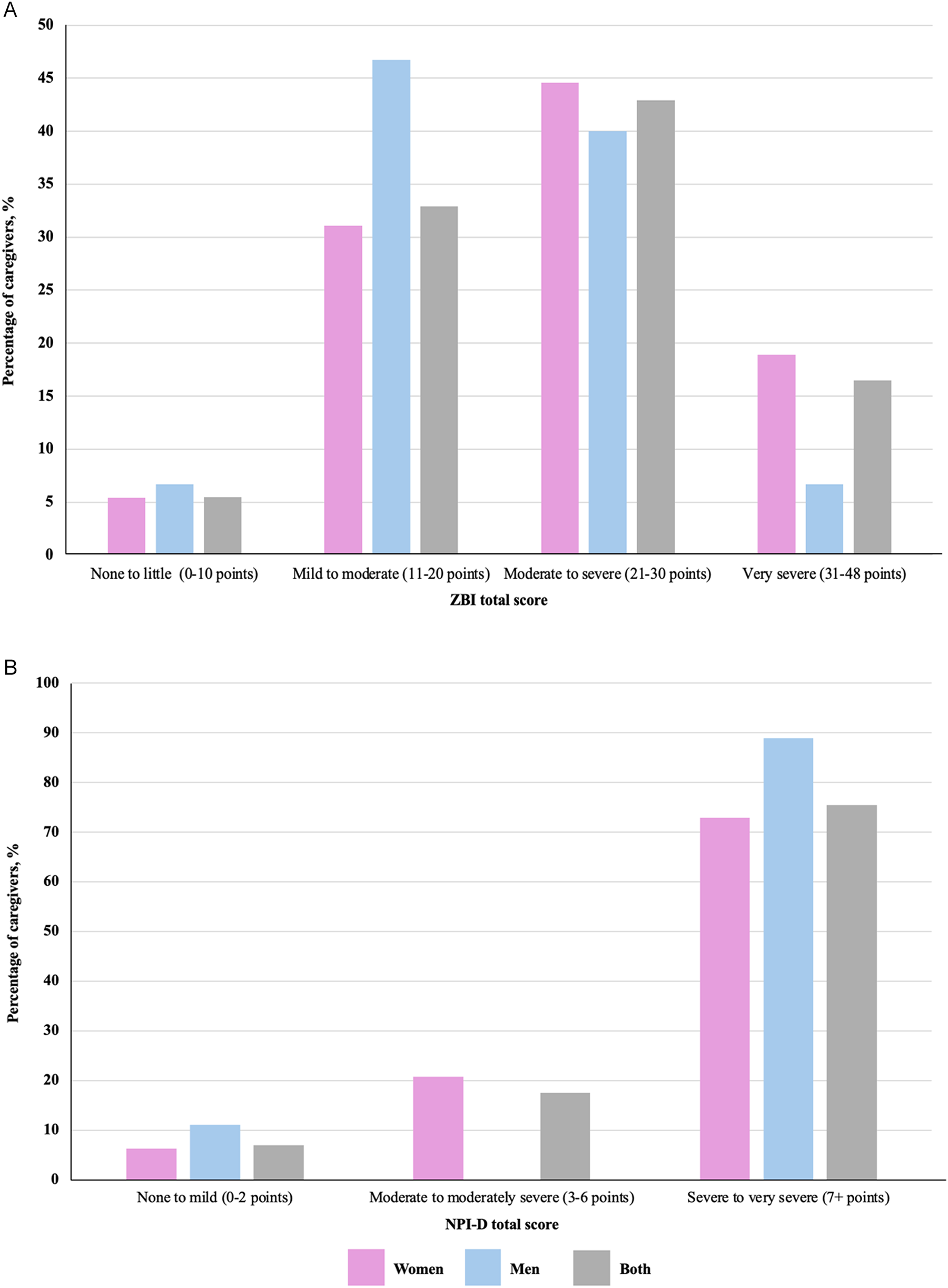
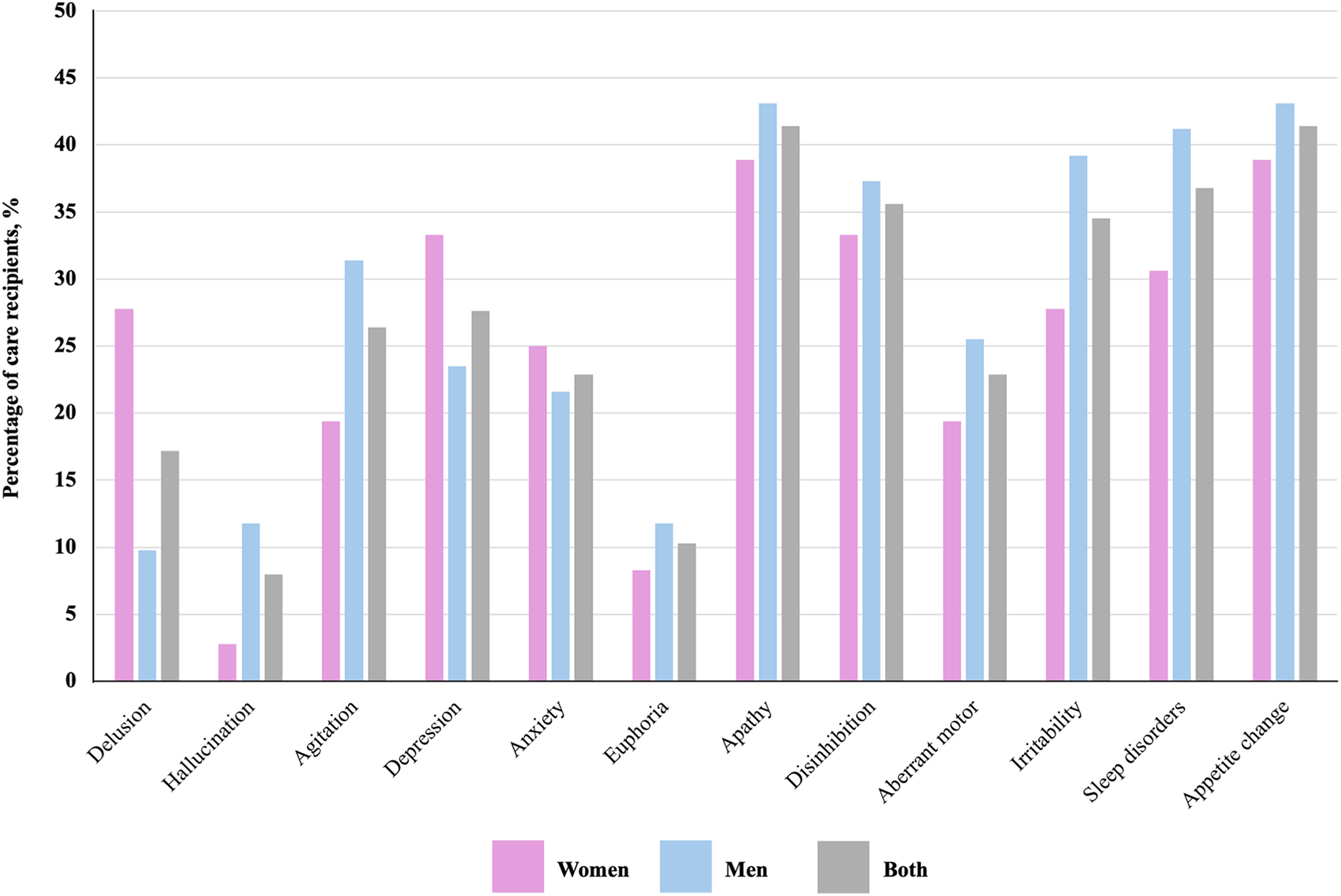
Most respondents (74%) stated that their burden was never formally assessed during their journey in the healthcare system. Respondents reported experiencing substantial caregiver burden according to the ZBI, with a mean score of 23.1 points (SD = 8.3). More than half of respondents (59.4%) had a ZBI score in the moderate to severe to very severe range (Figure 2). Regarding NPS, the mean total NPI score was 28.6 points (SD = 17.6). Most frequently reported NPS were apathy (41.1%) and appetite change (41.4%), followed by sleep disorders (36.8%), disinhibition (35.6%), and irritability (34.5%) (Figure 3). Minimally one clinically significant NPS was reported in 79.3% of care recipients. Delusions were more frequently reported in women care recipients than men care recipients (27.8% vs. 9.8%, p = 0.043). Respondents reported substantial distress from their loved one’s NPS according to the NPI distress subscale (NPI-D), with a mean total score of 15.3 points (SD = 10.9). Most respondents (75.4%) had an NPI-D score in the severe to very severe distress range (Figure 2). Bivariate correlation analyses revealed that score on the ZBI significantly correlated positively with the total NPI score, total NPI-D score, and with the NPI item score for agitation, apathy, disinhibition, irritability and sleep disorders (Supplementary Data). After adjusting for caregiver’s age and gender, and disease duration, burden significantly correlated positively with the total NPI score (β = 0.261, p = 0.021), the total NPI-D score (β = 0.571, p < 0.001), disinhibition (β = 0.356, p = 0.002) and irritability (β = 0.295, p = 0.007).
Reported burden and distress of respondents according to their gender. (A) Severity of burden according to the Zarit Burden Interview. (B) Distress according to the neuropsychiatric inventory distress scale.

Reported neuropsychiatric symptoms according to care recipient’s gender. Data represent the percentage of care recipients in whom caregivers reported the presence of clinically significant symptoms.

Discussion
This survey highlights some of the complex realities faced by Canadian caregivers of individuals with FTD. Respondents were predominantly educated women in their 50’s and 60’s, often spouses, but many also balanced employment, childcare or care for another individual. These multiple responsibilities, combined with average caregiving durations exceeding five years, underscore the sustained impact of FTD on families. Obtaining a diagnosis was lengthy and difficult. Caregivers reported an average TTD of 3 years, nearly seven clinical visits and consultation with multiple physicians before a final diagnosis was reached. Almost half of cases were initially misdiagnosed, most often as psychiatric disorders or AD. Delays were greater in younger-onset and sporadic cases, in men care recipients, and in those without early motor manifestations – consistent with the challenges of attributing behavioural changes to neurodegeneration. These healthcare journey patterns closely mirror those reported in international studies, underscoring the global nature of the diagnostic challenges in FTD. Reference van Vliet, de Vugt and Bakker19– Reference Loi, Goh and Mocellin31 Encouragingly, more recent cases showed shorter TTD, suggesting that awareness and access to specialized expertise may be improving.
Respondents’ characteristics in our study broadly parallel those reported in national caregiving data, including the Canadian Centre for Caregiving Excellence Caring in Canada survey, where caregivers are most commonly middle-aged women providing care to a spouse or parent, often over several years. 32 In our sample, caregivers had been providing care for a mean duration of 5.7 years, longer but comparable to national estimates (around 4.6 years), and a similar proportion lived with their care recipient (43.3% vs. 41% nationally). 32 Rural representation was also comparable (one-fifth of participants in our study). However, we noted important differences. Men were underrepresented in our study, and the proportion of spousal caregivers was higher than typically observed in broader caregiving populations, likely reflecting the younger age of onset of FTD compared to other dementias such as AD, which may reduce the proportion of adult-child caregivers. In addition, racialized and socioeconomically disadvantaged caregivers appear underrepresented, consistent with the online and network-based recruitment strategy, which may preferentially reach individuals with greater access to digital resources, higher health literacy, and stronger connections to support organizations. Interestingly, a higher proportion of care recipients in our study were residing in LTC (31%) compared to national estimates of approximately 15% reported by the Canadian Centre for Caregiving Excellence. 32 While this may suggest overrepresentation, it may also reflect disease-specific trajectories. Individuals with FTD often experience earlier and more severe behavioural and NPS, Reference Desmarais, Lanctôt and Masellis20 which can precipitate earlier institutionalization. Prior reports indicate that time to LTC admission is shorter in FTD (approximately 4–5 years post-diagnosis) compared to other dementias, such as the 5-year risk of admission in AD estimated at around 20%. Reference Huyer, Brown and Spruin33–Reference Davies and Howe35 These differences highlight that, while our sample may overrepresent certain caregiving contexts, it may also accurately capture the higher care complexity and earlier transitions to institutional care characteristic of FTD. Nonetheless, the lack of detailed national data specific to FTD caregiving limits our ability to fully assess representativeness, and findings should be interpreted with caution, particularly with respect to underserved populations.
Caregivers reported multiple barriers across the care continuum. The most common obstacles were limited knowledge of FTD among frontline clinicians, including mental health care providers, and insufficient access to specialized clinics and community services, particularly for YOD. Across provinces, home support services are generally designed for older adults and mental health care programmes focus on common psychiatric conditions, leaving many individuals with FTD – who often require elements of both – unable to meet eligibility criteria and inadequately served by existing care pathways. As a result, many respondents turned to private resources, raising concerns about equity. Reference Franzen, Nuytemans and Bourdage36 However, given that our sample was predominantly highly educated and likely more resourced, the reliance on private care observed here may not fully reflect the experiences of caregivers with fewer financial means, and may underestimate barriers in more disadvantaged populations. Similarly, the relatively high proportion of care recipients in institutional or supported living settings may limit generalizability, particularly for rural or lower-income populations where access to such options may be more constrained. Although we explored differences between urban and non-urban caregivers, income-level stratification was not available in our dataset and remains an important area for future research. Consequences of unmet needs were reflected in high rates of ER visits, hospitalizations and relocations due to behavioural crises. Caregiver burden was substantial: nearly two-thirds scored in the moderate-to-severe range on the ZBI. Similar high levels of burden have been reported in other FTD studies. Reference Armstrong, Schupf, Grafman and Huey37,Reference Besser and Galvin38 FTD caregiver burden is notably higher than caregivers in other neurodegenerative disorders, where average ZBI scores tend to be in the mild to moderate range, such as in AD Reference Skoda, Conant and Couture39–Reference Haro, Kahle-Wrobleski and Bruno41 and LBD. Reference Skoda, Conant and Couture39,Reference Haro, Kahle-Wrobleski and Bruno41,Reference Hayashi, Kobayashi and Shibuya42 Burden correlated strongly with NPS, especially disinhibition and irritability, which are both prevalent and distressing. Reference Desmarais, Lanctôt and Masellis20,Reference Desmarais, Gao and Lanctôt43,Reference García-Martín, de Hoyos-Alonso and Delgado-Puebla44 Notably, three-quarters of respondents stated that their burden had never been formally assessed, pointing to a gap in recognizing and supporting caregiver needs within the health system.
Our study also highlights potential sex- and gender-related dynamics in caregiving. Men caregivers were most often spouses, whereas women caregivers included spouses, daughters and siblings, consistent with broader societal caregiving roles for women. Reference Duangjina, Jeamjitvibool and Park45,Reference Sourial, Arsenault-Lapierre and Margo-Dermer46 Men care recipients were more likely to remain at home despite similar reported disease duration. While this observation may be consistent with hypotheses related to biological differences (e.g., relative preservation of functional abilities) or gendered caregiving roles, our data do not allow us to determine underlying mechanisms, and unmeasured factors – such as socioeconomic context, and access to services – may have contributed to this association. Reference Li, Manuel and Isenberg47,Reference Memel, Staffaroni and Ilan-Gala48 Differences in reported clinical presentations were also observed, with mood changes more frequently identified at onset in women and language difficulties, including PPA, more often reported in men. These findings should be considered exploratory, as they may reflect a combination of biological variation, caregiver perception or clinician diagnostic practices. Reference Silvestri, Almici and Libri49,Reference Pengo, Alberici and Libri50 Importantly, prior work in AD suggests that sex and gender can substantially influence both the perception and reporting of symptoms, with women caregivers generally reporting a higher number and greater severity of symptoms than men. Reference Abken, Ferretti, Castro-Aldrete, Santuccione Chadha and Tartaglia51,Reference Kroenke and Spitzer52 Moreover, informant-related characteristics – including relationship to the patient, sex and gender, and cultural or socioeconomic context – are known to shape the assessment of dementia symptoms and perceived disease severity, potentially contributing to observed differences. Reference Abken, Ferretti, Castro-Aldrete, Santuccione Chadha and Tartaglia51,Reference Kroenke and Spitzer52 Finally, men care recipients were reported to experience longer diagnostic delays, whereas men caregivers reported shorter ones. These differences may reflect variations in perception or reporting rather than true differences in healthcare trajectories. Evidence from AD also indicates that sex- and gender-related factors can influence the patient journey across diagnosis and treatment, including pathways to specialist referral, which may in turn affect TTD. Reference Berve, a and Fernandez53 Given the cross-sectional and self-reported nature of the data, and the absence of adjustment for potential confounders (e.g., disease severity, caregiver employment status, or regional healthcare factors), these findings should be interpreted as associative rather than causal. Reference Ballering, Olde Hartman, Verheij and Rosmalen54,Reference Aguzzoli, Walbaum and Knapp55
Limitations
Our study has several limitations that should be considered when interpreting its findings. As in most survey-based research, sampling and response biases are possible. Respondents were predominantly white, well-educated women, which may limit the generalizability of our results to more ethnoculturally diverse caregivers. Caregiving experiences can vary widely according to sex, gender, cultural background and socioeconomic status, and barriers to care may be amplified by financial constraints or systemic inequities. Consequently, our sample may not fully reflect the diversity of caregiving contexts in Canada. Provincial representation was uneven, with a higher proportion of respondents from Quebec and Ontario and fewer participants from other provinces. This distribution may reflect differences in the availability of specialized memory and FTD clinics, established research and clinical networks, and access to advanced diagnostic resources (e.g., PET imaging), which may have facilitated recruitment in certain regions. As a result, our findings may more strongly reflect the experiences of caregivers in provinces with greater access to specialized services. In addition, healthcare delivery for dementia varies across provinces, including differences in access to diagnostics, specialist care, community supports, and LTC resources, which were not accounted for in our analyses. The study was not powered to support meaningful province-level comparisons, limiting our ability to explore these interprovincial differences in detail. These factors should be considered when interpreting our results. Nevertheless, responses were obtained from multiple provinces and from caregivers residing in urban, suburban, and rural areas, offering valuable insight into common challenges faced nationwide. Diagnoses and clinical features were caregiver-reported and could not be independently verified, introducing potential for misclassification and uncertainty. For instance, some cases reported as late-onset (e.g., >80 years) may represent alternative aetiologies such as frontal-variant AD, and diagnoses were not neuropathologically confirmed. However, most respondents indicated that the diagnosis was established by a specialist following investigations in dedicated clinics (e.g., neuroimaging and, in many cases, genetic testing), which supports a reasonable level of diagnostic validity. Importantly, the retrospective nature of the survey introduces a risk of recall bias and temporal distortion, particularly given the prolonged caregiving trajectories observed in our sample. Approximately half of cases were diagnosed more than seven years prior to survey completion, and the average caregiving duration exceeded five years. As such, key variables – including TTD, number of clinical encounters and initial misdiagnoses – relied on long-term recall and may be subject to imprecision. Caregivers may unintentionally overestimate diagnostic delays or the number of healthcare interactions, and salient or distressing experiences may be preferentially remembered, potentially amplifying the perceived burden and challenges of the diagnostic journey. Conversely, some events may be underreported or inaccurately sequenced over time. These factors should be considered when interpreting estimates related to healthcare trajectories, although the consistency of our findings with prior international studies Reference van Vliet, de Vugt and Bakker19, Reference Libri, Altomare and Bracca30, Reference Loi, Goh and Mocellin31 suggests that the overall patterns observed are likely robust. Moreover, given the clinical heterogeneity and overlap among FTD syndromes, our relatively modest sample size – reflecting the epidemiological rarity of FTD – limited the ability to perform detailed subgroup analyses. Even so, the study identified key barriers and needs that appear consistent across the spectrum of FTD disorders. Finally, online recruitment may have preferentially reached caregivers already connected to dementia networks, potentially underrepresenting those less engaged with formal supports. Despite these limitations, this study represents the first survey specifically exploring the lived experience of Canadian caregivers of individuals with FTD. It offers novel, systematically collected data on diagnostic pathways, caregiver burden, and potential system-level barriers, thereby providing a foundation for improving caregiver support and access to specialized care in this population.
Conclusion
Caregivers of individuals with FTD in Canada face prolonged diagnostic journeys, high burden and limited access to specialized care. Barriers were particularly pronounced for younger-onset and sporadic cases and were compounded by behavioural symptoms that are distressing yet underrecognized. Key priorities include improving frontline clinicians’ awareness of FTD, expanding access to specialized clinics and community resources, integrating caregiver assessment into care pathways and addressing inequities in access – particularly for YOD and underrepresented populations. Greater public, clinical and policy awareness of FTD is essential to reduce diagnostic delays, support families and ensure more equitable, responsive dementia care in Canada.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cjn.2026.10609.
Data availability statement
Data access requests can be made by contacting the corresponding author. Requests will be assessed on a case-by-case basis and will require a data-sharing agreement.
Acknowledgements
We would like to thank all the individuals with frontotemporal dementia or a related disorder as well as their caregivers for partaking in this study. We would also like to thank Sylvain G. Bélisle for his assistance in creating the figures.
Author contributions
AM and PD designed the study. AM, MC and PD collected and analysed the data. AM, MC, KM, MN, EML, ES and PD interpreted the data. AM and PD drafted the manuscript. All authors contributed significantly to the content, critically reviewed and approved the final manuscript for publication.
Funding statement
This research received funding from the Canadian Consortium on Neurodegeneration in Aging, which is supported by a grant from the Canadian Institutes of Health Research with funding from several partners.
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship and publication of this article.
Disclaimer
All inferences, opinions and conclusions drawn in this study are those of the authors.



 Open access
Open access
Target article
Barriers to Clinical Care in Frontotemporal Dementia and Related Disorders: A Cross-Sectional Survey of Patients and Caregivers’ Journey in the Canadian Healthcare System
Related commentaries (1)
Reviewer Comment on Martineau et al. “Barriers to Clinical Care in Frontotemporal Dementia and Related Disorders: A Cross-Sectional Survey of Patients and Caregivers’ Journey in the Canadian Healthcare System”