
One of the most significant advancements in modern medicine has been the shift away from large incision “open” surgeries to video-assisted endoscopy, a groundbreaking innovation invented and pioneered by Camran Nezhat, MD, in the late 1970s.[Reference Tokunaga1–Reference Kelley4] Initially referred to as “keyhole,” “Band-Aid,” video surgery, or video laparoscopy, video-assisted endoscopy and video-assisted thoracoscopy (VAT) are now universally referred to as “minimally invasive surgery” (MIS), with or without robotic assistance. Dismissed as a barbaric and dangerous gimmick just 30 years ago, today MIS is recognized for profoundly improving the health outcomes of hundreds of millions of patients around the world. Indeed, with countless lives saved and millions of hospitalizations and surgery-related permanent disabilities prevented, the transformative impact that MIS has had on patients has been so remarkable that it has been described as a change to surgery as revolutionary for our era as anesthesia was for the nineteenth century.[Reference Tokunaga1–Reference Kelley4]
Unanimously Hailed as the Gold Standard
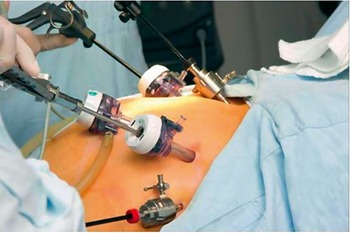
Today, the minimally invasive method of video-assisted endoscopy is recognized throughout the world as the unequivocal new gold standard in essentially every discipline of surgery.[Reference McMahon, Fischbacher, Frame and MacLeod5–14] Even for procedures like bowel resection, traditionally dominated by large incisions as the standard of care, a dramatic shift eventually occurred by approximately the mid-2000s, with leading authorities like the New England Journal of Medicine in 2004 finally acknowledging that open abdominal surgery for bowel resection should be converted to minimally invasive approaches, the same procedures that were called barbaric when Camran Nezhat, Farr Nezhat, and their team developed it.[15,Reference Nezhat, Kavic, Nezhat and Nezhat16] Notably, too, in oncology, pediatrics, and emergency medicine – where MIS had been staunchly contraindicated for most of the twentieth century – a remarkable reversal has taken place as well, as practitioners in these fields are now urging their peers to phase out over-reliance on large incision open surgeries in favor of MIS [Reference Nelson17,Reference Pappas and Jacobs18] (Figure 1.1).
Dr. Nezhat and fellows in the simulation lab.

Figure 1.1 Long description
In the foreground, a highly realistic medical training mannequin lies on a gurney, draped in blue and green sheets, with its chest cavity open for a simulated procedure. One male individual, likely a doctor or medical student, stands beside the mannequin, wearing a white lab coat and a tie, holding a surgical instrument and seemingly performing a procedure. To his left, another male individual in a lab coat observes. To the right of the individual performing the procedure, a male individual in a dark sweater. Further to the right, a female individual, dressed in a lab coat over blue scrubs, is observing the scene. The room itself is equipped with medical instruments and technology, including a wall-mounted monitor, a medical cart with various equipment, and two clocks on the back wall.
In the context of our modern understanding, MIS may appear as an evolutionary inevitability akin to the natural progression of humans walking upright. However, a retrospective examination reveals that reaching this pinnacle of acceptance almost didn’t survive the intense academic conflicts that erupted for calling into question 170 years of established surgical norms and asserting that large incisions were no longer optimal care. More than this, the new surgical reality brought to light that, in many cases, large incisions were not just unnecessary but also posed risks of increased chronic pain, morbidity, and even mortality compared to the original illness.
Yet, the practical reality was that asking established surgeons to abandon all that they knew and relearn how to perform surgery from a TV monitor through tiny portholes using “long sticks” was viewed as not only entirely scandalous but too risky to attempt. This was especially true during the 1980s for very advanced procedures like laparoscopic treatment of multi-organ stage IV endometriosis, including management of endometriosis of the bowel, bladder, ureter, diaphragm, and so on, that were being performed by Drs. Camran and Farr Nezhat and their team.[16,19] This also came at a time when early reports of miraculous outcomes – of blood loss measured in teaspoons instead of cups, of patients returning home within hours after major surgery instead of after days or weeks in the hospital – were still being largely dismissed by academic medicine as utter impossibilities. It wasn’t long, however, that disbelief devolved into false accusations that the early pioneers were hiding their complications or fabricating their results. In other words, rather than seeing MIS as the future of surgery, what most saw was an innovation that appeared to be not only unnecessary but also a dangerous deviation from established norms without any possible present or future value. Faced with such an impenetrable fortress of resistance, for many years, it proved exceedingly difficult to convince anyone that MIS could – or should – replace traditional open surgeries (Figures 1.2 and 1.3).
Open surgery.

Modern-day surgery. It stunned Nezhat to realize how outraged others were with his “after” version of surgery, even though it was associated with lowered morbidity and significantly less pain than traditional open surgeries like the one shown in the “before” image.

Diagnostic & Early Forms of Therapeutic Laparoscopy
To get a better understanding of just how stacked the odds were to have overcome such seemingly insurmountable obstacles, it’s helpful to step back and evaluate the surgical landscapes of both gynecology and general surgery as they stood during the formative years of the late 1970s and early 1980s when modern-day video laparoscopy emerged. Something that is not so clearly spelled out in other historical accounts is that there was actually already significant skepticism in the late 1970s concerning the use of pre-video laparoscopy in surgical applications. In fact, many historical accounts erroneously suggest that gynecologists, in particular, had “fully embraced” pre-video laparoscopy as a standard modality by the 1970s.[Reference McMahon, Fischbacher, Frame and MacLeod5,20] While there is a grain of truth to this, with respect to diagnostic laparoscopy and some minor therapeutic indications, for advanced operative procedures, the story was quite different.
To understand this paradox, it’s also critical to step back in history even further and consider the separate histories of video laparoscopy’s two most important predecessors: diagnostic laparoscopy and operative laparoscopy. Diagnostic endoscopy and laparoscopy have antecedents stretching back as early as the sixteenth century, when polished metal reflectors, combined with modified tubes or specula, were used to attempt visualization of internal body cavities. However, most regard Philip Bozzini’s 1806 introduction of a (relatively) more sophisticated system as the beginning of modern-day diagnostic endoscopy.[Reference Bozzini21] Yet, for most of modern history, applying the endoscope abdominally (laparoscopy) proved far too treacherous an enterprise. This meant that, for centuries, the body’s most critical organs could not be viewed or easily accessed through minimally invasive means. While some attempts of diagnostic laparoscopy from the nineteenth century and even earlier have been reported, most consider the German gastroenterologist Georg Kelling as the first to successfully utilize an abdominal approach when he viewed the abdomen of an anesthetized dog in 1901 with what was referred to as a coelioscope and later performed this new minimally invasive diagnostic technique on a small series of patients.
Regarding laparoscopy’s operative history prior to video, French urologist Antonin Desormeaux is often acknowledged as the first, in 1853, to conduct a large series of clinically successful therapeutic cystoscopic procedures guided by true endoscopic visualization. However, it wasn’t until 1910 that the first successful minor operative laparoscopic procedure would be achieved by Swedish internist Hans Christian Jacobaeus, who was the first to coin the term laparoscopy and went on to laparoscopically lysed adhesions in the abdominal cavities of 17 patients and in the chest area of 2.
Thereafter, a new generation of laparoscopic pioneers from around the world emerged, including Drs. Abbot Beling, Bertram Bernheim, Edward Benedict, Boesch, Karl Fervers, Heinz Kalk, Roger Korbsch, Severin Nordentoeft, B. H. Orndoff, Raoul Palmer, Richard Telinde, and John Ruddock, who performed simple therapeutic and diagnostic laparoscopic procedures in the pre-video era of the early twentieth century. In fact, the field had gained enough acceptance as a predominantly diagnostic modality that Roger Korbsch published in 1927 what is believed to be one of the first textbooks on the subject.[Reference Nordentoeft22–24]
From this field of acclaimed innovators, the work of Heinz Kalk stands out in particular, earning him the honor as the founder of the German school of laparoscopy. Kalk’s achievements at the time were legendary and include technical innovations as well as groundbreaking publications, including his 1939 article reporting a series of 2000 liver biopsies with no fatalities. In the US, John Ruddock was also one of the most advanced laparoscopic pioneers of his era, whose contributions also included technical improvements to his newly designed peritoneoscope, which was successfully utilized in 200 patients by 1934. Throughout the 1930s, Ruddock was also one of the most vocal in imploring others to incorporate diagnostic laparoscopy as a way to avoid the exploratory laparotomies that were rising in popularity at the time, but which he bluntly stated “should be condemned.” To help persuade his colleagues, Ruddock offered some of the earliest statistics, reporting that, in his experience, clinical diagnoses had an error rate of 48%, compared to just 6% with diagnostic laparoscopy. By 1937, Edward Benedict reported on the laparoscopic aspiration of a large ovarian cyst on an 85-year-old patient. Benedict’s general techniques were similar to those prevailing at the time, such as the use of two trocar sites, atmospheric air to insufflate the abdomen, and relying only on local anesthesia in conjunction with sedative drugs. Although Korbsch introduced an insufflation needle in 1921, it was in 1938 that Janos Veress significantly improved the technology with his spring-loaded version with a beveled point for cutting through tissue. As the field expanded, formalized reporting of contraindications emerged, with Beling providing one of the most extensive reviews of the literature in 1939. By 1943, internationally recognized pioneer Raoul Palmer entered the field and began performing diagnostic and simple therapeutic laparoscopies in Occupied Paris during World War II, including biopsies and lysis of adhesions for gynecologic conditions. Using a modified McCarthy cystoscope, coupled with redesigned insufflators that he designed and initially built himself, Palmer placed patients in the Trendelenburg position for better pneumoperitoneum and was one of the earliest to recognize the importance of careful monitoring of insufflation. Medical historians now regard Palmer as a pioneering figure in laparoscopy, having produced the most significant published work on the application of the technique in women’s medicine during that era.
Concerns about Over-Enthusiasm
Throughout this early-twentieth-century time frame, interest in this exciting new field was reportedly so heightened that concerns about over-enthusiasm began to surface. However, the euphoria was short-lived, as reports of potentially serious and sometimes fatal complications quickly circulated. Given the abundance of vital organs, veins, and arteries in the abdomen, all forms of laparoscopy initially faced significant morbidity and mortality rates. Setting aside the small number of early pioneers with outsized skills, the vast majority of practitioners would never be able to reach this level of expertise. Progress was also severely curtailed due to the outbreak of World War II. The end result was that diagnostic and therapeutic laparoscopy gradually faded into relative obscurity, essentially abandoned by the majority of US practitioners by the 1950s, with just a handful of virtuosos continuing to defy the odds. This shift was also influenced by the increasing safety of open abdominal procedures, making them not only the preferred operative approach but which also allowed for the notorious exploratory laparotomy to continue as a favored diagnostic modality for much of the second half of the twentieth century.
With both diagnostic and operative laparoscopy now viewed as too dangerous to pursue further, it would take years to revitalize the same level of interest in the field that had enthralled the world just a couple of decades earlier.
Laparoscopy Revival of Interest during the 1950s–1970s
It was only after the introduction of crucial technologies in the 1950s–1970s, coupled with the advocacy work by the era’s acclaimed practitioners to keep the field alive, that a modest resurgence of interest in all forms of endoscopy emerged, particularly in gastroenterology and gynecology.[Reference Hopkins and Kapany25–27] Our team covered a more complete history of the legendary pioneers of laparoscopy of the 1950s–1970s in Nezhat’s History of Endoscopy, but some of the most preeminent include Drs. Henk De Kok of the Netherlands, Victor Gomel of Canada, M. A. Bruhat of France, Jacques Donnez of France, Carl Levinson of the US, Kurt Semm of Germany, Hubert Manhes of France, Hans Frangenheim of Germany, and Patrick Steptoe of England, as well as continued innovations by Palmer.[Reference Nezhat and Page28]
One of the most spectacular moments arrived in 1958 when Frangenheim produced his famous color film of a laparoscopically captured ovulation in progress, a feat that would reverberate throughout the world of gynecologic surgeons for years to come.[Reference Fragenheim and Finzer29] Although Palmer had presented one of the world’s first color films of a laparoscopic procedure earlier, in 1955, it was Frangenheim’s captivating milestone in particular that catalyzed a wave of renewed interest in laparoscopy’s capabilities.
In terms of operative progress, numerous gynecologists continued the work of pre-war pioneers in laparoscopic sterilizations. Notably, British physiologist and future Nobel Prize winner Dr. Robert Edwards and his gynecologist collaborator, Dr. Patrick Steptoe, were pioneers in this field. Dr. Steptoe routinely performed laparoscopic tubal ligations, utilizing the two-puncture technique, during the 1950s and early 1960s. His expertise in laparoscopy proved instrumental when he applied his skills to retrieve oocytes, ultimately leading to the birth of the first in-vitro fertilization (IVF) baby, Louise Brown. Throughout this same period, Jacques Donnez and his team were also instrumental in advancing laparoscopy in the field of IVF.
Perhaps more than anyone, the legendary Dr. Kurt Semm defined the era and advanced the field tremendously, with several innovations and over 1000 publications. Renaming laparoscopy as “pelviscopy,” Semm began developing newly designed instrumentation and techniques as early as 1960, including an improved automatic insufflator and innovations in laparoscopic suturing, which enabled him to perform procedures throughout the 1970s, including the first reports of pre-video laparoscopic ovarian cystectomy, as well as adenectomy and myomectomy.
By 1971, H. M. Hasson introduced “open laparoscopy,” which allowed for direct visualization of trocar entrance, a crucial innovation since trocar injuries were and continue to contribute to as much as 40% of mortality in laparoscopic surgery. In 1972, H. Courtenay Clarke introduced new laparoscopic suture techniques, performed operative procedures, and designed and built newly improved instrumentation. As early as 1973, laparoscopic treatment of ectopic pregnancies was advanced and routinely performed by Bruhat of the University of Clermont-Ferrand in France, along with his colleagues Mage, Pouly, and Manhes, with Manhes developing several instrument innovations. Victor Gomel was one of the most prominent laparoscopic pioneers of the era as well and reported good results with infertility patients undergoing corrective laparoscopic surgery. By 1977, the first laparoscopic appendectomy was achieved by De Kok, who went on to publish one of the largest series of laparoscopic appendectomies at the time, followed by Semm, whose first laparoscopic appendectomy was performed in 1980. In 1979, Bruhat et al. introduced the CO2 laser for laparoscopy, while Yona Tadir of Israel independently accomplished the same in approximately the same period. In the US, past president of the American Association of Gynecologic Laparoscopists (AAGL), Carl Levinson, was one of the most respected laparoscopists of the era for his work in advancing the field, including the laparoscopic treatment of ectopic pregnancies and management of various infertility conditions.
During this period, the establishment of pioneering organizations also emerged. In 1941, the American Gastroscopic Club, now known as the American Society of Gastrointestinal Endoscopy, was founded under the leadership of Rudolf Schindler, one of the most prominent figures in gastroenterology. Similar clubs were also taking shape in Europe, South America, and Asia. By 1959, the Japan Gastrocamera Society came into existence, marking the inaugural release of their society journal, Gastroenterological Endoscopy. In 1960, the European Endoscopic Club laid its foundation, serving as a precursor to the eventual establishment of the European Society of Gastrointestinal Endoscopy. Following closely thereafter, in 1962, the World Endoscopy Organization was founded. As for laparoscopy, Dr. Jordan Phillips founded the AAGL in 1971, marking a significant milestone. A decade later, in 1981, the Society of American Gastrointestinal Endoscopic Surgeons was established, further contributing to the evolution of endoscopy in multiple disciplines.
Through the tireless work of these early laparoscopic pioneers of the pre-video era, the volume of procedures being performed skyrocketed, with one source reporting that the number of tubal sterilizations performed laparoscopically increased from just 1% in 1971 to an astonishing 60% by 1976.[Reference Ricci30] By 1981, pre-video laparoscopy training had also been incorporated into “all major gynecologic residency programs” in the US,[Reference Nordentoeft22] an incredible rate of change considering that, just a decade earlier, in 1972, there were only about 30 centers in the US where laparoscopic procedures of any kind were being performed.[Reference Berci and Mitchell31]
Video Laparoscopy’s Technological Predecessors: TV, Film, Video, and Light Sources
In terms of technologies, there were also many important milestones being achieved. In fact, precursor component parts to video laparoscopy had actually been developed decades earlier. Cinematography and television had been used modestly since the early 1940s, with US pioneers Frank Dolley and Lyman Brewer presenting in 1942 what is believed to be the first known color motion picture of a live bronchoscopy.[Reference Dolley and Brewer32] By 1950, Japanese pioneers Dr. Tatsuo Uji, Mr. Fukami, and Mr. Sugiura, in collaboration with Olympus, had developed the gastro-camera, the world’s first miniaturized endoscopic camera for photography, about half the size of a nickel.[Reference Hadley33]
Soon thereafter, some of the most sensational moments in endoscopy’s history debuted, with the world’s first television broadcasts of live bronchoscopies, achieved separately in 1955 by the French bronchoscopists A. Soulas and J. M. Dubois de Montreynaud.[Reference Soulas34] As mentioned, Palmer and Frangenheim were also at the forefront of laparoscopy and color film, presenting their firsts in 1955 and 1958, respectively. By 1960, another significant advancement emerged with the introduction of the first commercially available flexible fiber-optic endoscope, co-invented by Basil Hirschowitz and Larry Curtiss in 1957. This groundbreaking technology played a pivotal role in propelling gastroenterology far ahead of other medical disciplines of its time.
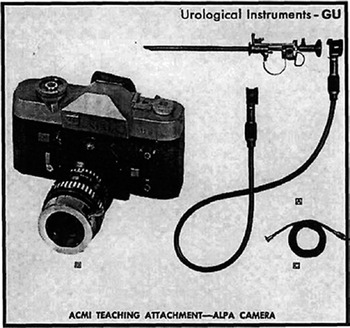
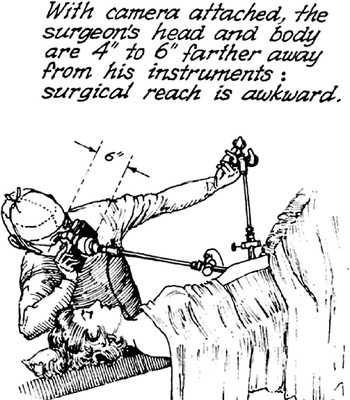
Still, these systems were not designed with operative video-assisted endoscopy in mind. Even as late as 1977, an article summarizing the latest in endoscopic TV and video devices – back then referred to as “teaching attachments” – described these technologies as useful for teaching and documentation purposes only; there is no mention of changing the method of performing endoscopic procedures to advance its operative potential [Reference Berci and Mitchell31,35] (Figure 1.4). And, as the figures from this article illustrate, even though 1977-era laparoscopes were equipped with cameras, the era’s most advanced laparoscopists, like Semm, were still using the endoscope in the traditional manner, hunched over and peering awkwardly through the eyepiece. Additionally, teaching attachments were limited, allowing only a limited number of participants to be involved in the learning process [Reference Phillips36,37] (Figure 1.5).
A catalog ad for a “teaching attachment,” circa 1960s, which is what laparoscopic camera systems were referred to before Nezhat’s introduction of video-assisted endoscopy. The old way of performing laparoscopy.

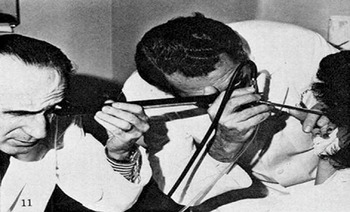
Dr. Berci, one of the pioneers performing laparoscopy in the late 1970s.[Reference Berci38]

Delayed: What Seemed Like an Endless Wait at Tubal Ligations
In other words, even with these cutting-edge technologies, it eventually became clear that pre-video laparoscopy was of limited utility for more advanced operative procedures. This was attributable to its seemingly inescapable, centuries-old design, which required surgeons to hunch over, squinting with one eye closed and one hand encumbered in order to view the surgical field directly through the small aperture of the scope. In this manner, there was no way for laparoscopists to avoid those infamous painful contortions they found themselves in just so they could obtain what amounted to no more than a negligible view of the anatomy. As a result, for the vast majority of surgeons, advanced operations with the laparoscope were essentially infeasible at best and perilous at worst (Figure 1.5).
Given so many seemingly insurmountable obstacles, it’s easy to understand why progress toward more advanced laparoscopic procedures had essentially stagnated by the late 1970s, entrapped by imaginary boundaries beyond which it was forbidden to go. It wasn’t too long ago, in fact, that most surgeons were aghast at the mention of using the laparoscope to remove even just ectopic pregnancies, let alone resecting the bowel. As for gynecology’s operative laparoscopic superstar of the 1960s–1970s – tubal sterilization – its origins trace back to 1936 when Swiss surgeon Boesch performed the world’s first documented laparoscopic tubal sterilization using electrocauterization.[Reference Ricci30,Reference Boesch39] Naturally, the technique underwent refinements over the years. Yet, by the close of the 1970s, conceptually, the procedure had not changed much from its 1930s debut.
Indeed, with the exception of the achievements of the era’s inimical surgical superstars, in gynecology the entire discipline seemed stalled at the tubal ligation as if it were the final frontier. Even as recently as 1977, Semm received a decidedly reserved reception at an AAGL medical conference where he demonstrated various operative laparoscopic procedures that he performed in the traditional manner of peering directly into the scope. “Kurt Semm’s pelviscopy presentation struck people in that meeting as going too far,” recalls Richard Soderstrom, one of the founding members of the AAGL. And this was the response from one of the most welcoming societies in the world for laparoscopic innovation. With the debate titled “Laparoscopy Is Replacing the Clinical Judgment of the Gynecologist,” it was abundantly clear that advancing the scope beyond its prescribed therapeutic and diagnostic roles was simply too unsettling and unacceptable for most.[Reference Soderstrom40]
Overcoming the Mythology of Laparotomy
Perhaps the greatest mythology to overcome was the nearly universal consensus that a large abdominal incision – laparotomy – was irreplaceable as a surgical modality. At the time, it was ingrained in the surgeon’s mind that the bigger the surgery, the larger the incision should be. This was true, despite the many vocal protests from female patients, who had been insisting on vaginal entry surgeries for more than a century just so they could avoid laparotomies.[Reference Short24] And even though surgeons too had been bemoaning its significant mortality rates since at least 1898, by about the mid-twentieth century, laparotomy’s perceived benefits began to overshadow its formidable downsides, a change brought about by the introduction of antibiotics and safer anesthesia. Transformed now into a paragon of surgical virtue, its often serious complications were somehow downplayed as normal and necessary for the sake of saving a patient’s life.
With classical surgery’s large incision allowing ample room to view and palpate the internal viscera, to be free of any spatial confinements or depth-of-field distortions, to see in 3D and directly (as nature intended), attending to hemorrhages with the greatest of ease: these were all undeniable advantages for surgeons, believed to be crucial for the very survival of patients and thought to be unattainable by any other means. And, with the introduction of even more advanced medical adjuvants in the late twentieth century that made laparotomies even safer – improved anesthetics, intramuscular antibiotics, and anti-hemorrhagic agents – morbidity and mortality rates began to decline.
Meanwhile, microsurgery, a more refined version of large incision surgery, emerged as a popular modality. By the late 1970s, it was beginning to be touted as a possible panacea for all the flaws associated with the more traumatic “gross” laparotomy. Although microsurgery was still open surgery, only in disguise, nevertheless, at first glance, it actually had a lot to offer, apparently almost as much as video laparoscopy: a more comfortable operating position, magnification, and reduced damage to tissue, resulting in fewer adhesions. And, when applied to fertility surgery, spectacular results with microsurgery were reported, with purportedly doubled, even tripled, fertility rates commonly cited. Other sensational milestones soon followed, like the world’s first vascularized fallopian tube transplant by Brian Cohen in 1975, achieved with the aid of microsurgical techniques. With rock star moments like these, who needed a new surgical philosophy? The existing ones appeared to be working just fine.[Reference Soderstrom40]
To be fair, such sentiments were understandable for much of the twentieth century when there were indeed few other choices for open surgery. The fact is that large incision surgeries during modern times saved more lives than they took, which is why attempting to define just who the real antagonist is in this story is not only futile but also an exercise that wouldn’t provide much meaningful insight anyway. Rather, these historical vignettes provide a greater understanding of just how easily biases can slip past the scientific process and how beliefs can become “a form of blindness,” even when they’re slipping toward obsolescence.
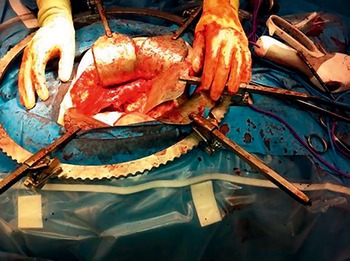
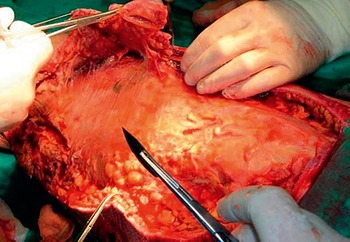
By the time pioneers and patients alike began pushing for more advances in MIS, the surgical opinions that were being questioned had been viewed as nearly infallible truths for almost two centuries. However, prevailing opinions are only as good as the data that inform them. We assume that evidence-based medicine and the peer-review process will weed out the bad and usher in the good, but don’t such systems fall apart if the right questions are not being asked in the first place? Even with the best of intentions, aren’t clinical observations imperfect inputs, viewed as they so often are through the distorted lens of an observer’s own flawed assumptions? These were the sorts of issues that had to be carefully considered in order to convince others that the time had come to reevaluate the surgical status quo (Figure 1.6).
A recent image of a laparotomy, metal retractors and all.

Backlash to Laparoscopy for the Second Time in the Twentieth Century
As if these conceptual plateaus were not enough, gynecologic laparoscopy in the US experienced another season of discontent, just beginning to surface in the late 1970s. Growing concerns over complication rates associated with pre-video laparoscopic sterilizations began to surface. Although some aspects of the reporting were sensationalized, the unexpected rise in complications triggered a nearly instantaneous backlash against laparoscopy in general, as articles forewarning of its potential for serious mishaps began seeping into the medical literature and eventually the lay press. One of the first such articles to gain national attention was published in 1977 by the founder of the AAGL, Jordan Phillips. Phillips’s exposé, which outlined in stark detail the estimated complication rates associated with laparoscopic tubal sterilizations, struck a raw nerve within surgical communities and served for a time to temper enthusiasm.[Reference Phillips41]
Soon thereafter, urgent congressional hearings and other governmental advisory panels were called into session to address concerns about the rapid technological changes affecting endoscopic medical devices in particular and medical technologies in general. Symbolic actions were taken against all forms of endoscopy, beginning most conspicuously with the Medical Device Regulation Act, passed in 1976. Later, in 1981, the Centers for Disease Control and Prevention (CDC) in Atlanta issued a terse public rebuke over patient deaths apparently linked to unipolar electricity sources used in laparoscopic sterilizations.[Reference Fuller, Scott, Ashar and Corrado42,Reference Jamieson, Hillis and Duerr43]
Only a handful of physicians were swift to publicly advocate for this procedure in this time period. One in particular, Dr. Preston Williams, published an article in 1974 highlighting the recent increase in gynecologic laparoscopic complications, and attests this to the lack of proper training with the newfound technology. Williams advocates for a more structured and informed approach to disseminating these procedures in the field of medicine, stating that the generally accepted paradigm “do one, see one, teach one” was not sufficient in these cases.[Reference Williams44] Alternatively, Williams stresses that these complications are highly avoidable, and highlights the minutiae among each category of complications, and how to improve each one. Williams vehemently argues that if proper precautions are taken and these procedures adhere to a strict set of guidelines, the complication rates can be greatly decreased.[Reference Williams44] He further explains that the lack of mastering diagnostic laparoscopy is the downfall of surgeons attempting surgical laparoscopies, and that with more knowledge and instruction, patient safety can be protected. Despite this article being one in favor of the safe usage of laparoscopy, the nature of the lengthy paper accentuating all of the current drawbacks of this procedure was only a reinforcement to the public opinion: laparoscopic surgery is undertrained, unsafe, and unwanted by the medical community.
In such an environment of growing controversy, eventually, failed sterilizations became the second leading cause of lawsuits for obstetrician-gynecologists in the US. Since the medical community tends to err on the side of caution, such adverse reports – whether exaggerated or not – were nearly the death knell for endoscopic innovation in those days.
Operative Progress Ossified in Its Tracks
The impact of these growing controversies and lingering conceptual constraints are plainly evident when one reviews the literature and textbooks from the 1970s–1980s, which reveal that the laparoscopic procedures being performed were essentially no more advanced than those that had been introduced nearly 50 years earlier: draining cysts, lysing adhesions, biopsies, cautery of neoplasms, and tubal ligations.[Reference Soderstrom45–Reference Wheeless51] For all of the most complex gynecologic pathologies that required surgery, large incision laparotomies remained the only surgical solution available to essentially most surgeons, as the work of Semm and other virtuosos unfortunately failed to be widely adopted due to the still insoluble issues of scalability and reproducibility. By the late 1970s, these same limitations of laparoscopy could be seen in general surgery as well, which had essentially advanced no further than liver biopsies, the same procedure that Kalk had mastered in the 1930s.
And so it unfolded that the revivalist heyday, which laparoscopists had so enjoyed during the post-war period, had been nearly neutralized by the end of the 1970s, leaving operative progress practically ossified in its early twentieth-century tracks. As is usually the case, it would be psychological resistance to change that proved to be the far more formidable element to overcome.
A Dream Is Born: The Introduction of Video-Assisted Endoscopy
Dr. Camran Nezhat simply could not reconcile what he was witnessing: the glaring inconsistencies of laparoscopy itself, fully actualized in its diagnostic domain, then bounding forward toward essentially just one operative procedure – tubal ligations – gynecologic laparoscopy’s apparent operative endpoint. Meanwhile, progress toward other surgical procedures remained elusive rarities, isolated achievements performed by a few gifted outliers in just a few centers throughout the world.[Reference Fragenheim and Finzer29,35,36] It was a peculiar paradox to see the entire field stopping short of more advanced procedures that were so close anatomically. Seeing how quickly patients recovered from laparoscopies compared to laparotomies, it became inescapably clear that something was terribly amiss.
It seemed evident that one of the most significant hindrances thwarting laparoscopy’s surgical progress was the awkward positioning it required. Whether in diagnostic or operative mode, the entire enterprise left everyone contorted in the most absurd positions, bent over sideways, craning to peer down the scope’s tiny aperture held by one hand, leaving only one free to perform procedures. It was essentially a futile enterprise (Figures 1.7 and 1.8). Nezhat knew that if he could just find a way to circumvent these physical constraints, more surgeons would be able to tap into endoscopy’s true potential as an advanced operative force (Figure 1.9).
A recreation illustrating the traditional method of performing laparoscopy, involving squinting and being hunched over.

Another image showing the awkward angles required when performing laparoscopy in the old manner.

Figure 1.8 Long description
The professional is holding a long, slender instrument that extends towards the patient’s mouth or throat area. The patient is lying on what looks like an examination table, with part of their body covered by a sheet. A line with an arrow indicates a measurement of 6 degree above the professional’s head, suggesting an angle or specific positioning.
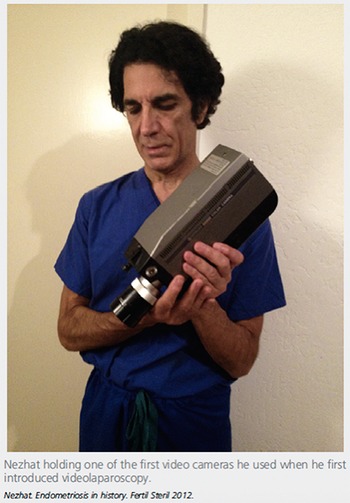
Dr. Camran Nezhat holding one of the first video cameras he used when he first introduced video laparoscopy.

By the late 1970s, Nezhat figured out just the right configuration of positions and parts. Of course, numerous modifications and technical innovations had to be made, including the deployment of two laparoscopes instead of one in order to deliver more light to the abdominal cavity. With the two laparoscopes and two light sources, he could now see well enough to operate while looking at the images on the TV monitor (Figure 1.10). With the equipment thusly transformed, Nezhat began operating “off the TV monitor,” which became the defining factor that enabled him to perform the most advanced procedures video laparoscopically. The surgeon’s two hands were now free, and both eyes could remain open now that squinting through an eyepiece was no longer necessary. Surgeons could also finally operate in a comfortable, upright position, which meant that operator fatigue no longer stood in the way of performing more lengthy and complex operations. And, with the entire surgical team able to see the surgery on the TV monitor, assistants could better anticipate the surgeon’s needs (Figure 1.11). In 1982, he added a CO2 laser to his instrumentation and called it video laser laparoscopy or video laseroscopy.
Nezhat performing video laparoscopy; two scopes are used in the abdomen, one was purely used for delivery of light as the light sources were inadequate.

Nezhat performing video laparoscopy, circa late 1970s – early 1980s: notice how large the video camera is compared to today’s instruments. Given this initially cumbersome setup, most found it impossible to believe that video endoscopy would be the future of surgery, leaving many to wonder about Nezhat’s sanity.

After this pivotal breakthrough, by the early 1980s, Nezhat was able to take on cases once deemed inoperable by the traditional pre-video laparoscope, pioneering for the first time video laparoscopic and truly comprehensive treatment of severe endometriosis involving major resections of multiple organs; complex cancer surgeries; bowel, bladder, ureter, diaphragm, lung, and liver resections and reanastomosis; pelvic and para-aortic node dissection and radical hysterectomy; ovarian remnant; sacral colpopexy; dermoid cyst removal; adnexal mass removal during advanced pregnancy; vesico- and rectovaginal fistula repair; and more.[16] During this period, his research faced repeated rejections from medical journals, leading Nezhat to shift his focus to teaching through postgraduate courses starting in 1982 and offered often biweekly at the Georgia Institute of Technology in Atlanta, Georgia, and Northside Hospital, in collaboration with Dr. Scott Crowgey. This educational endeavor continued at Stanford University Medical Center in Palo Alto, California (Figures 1.12, 1.13, and 1.14).
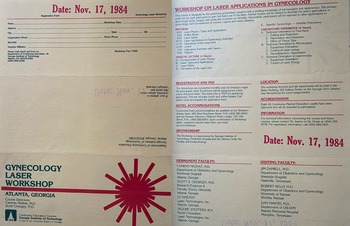
Brochure from a workshop on laser applications for gynecology directed by Camran Nezhat and Scott Crowgey in Atlanta in 1984.

Figure 1.12 Long description
The document is organized into several sections providing event details. Key information includes a registration form with fields for personal and professional details, a detailed workshop application for WORKSHOP ON LASER APPLICATIONS IN GYNECOLOGY, and sections outlining the program’s schedule, didactic lectures, and laboratory experience. Further details include registration and fee information, hotel accommodations, accreditation details, and contact information. The bottom part of the document lists permanent and visiting faculty members, indicating a roster of medical professionals involved in the workshop.
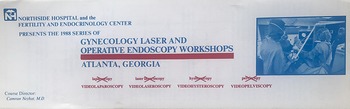
Brochure from one of the first workshops on MIS (video laparoscopy) directed by Camran Nezhat in 1988. He started teaching MIS in 1982.

Figure 1.13 Long description
The flyer lists various types of workshops, including Videolaparoscopy, Videolaseroscopy, Videohysteroscopy, and Videopelviscopy. At the bottom left, the course director is identified as Camran Nezhat, M.D. The flyer includes a screenshot of medical professionals in an operating room setting.
Brochure for a course on Minimally Invasive and Robotic Surgery taught by Camran Nezhat and his brothers in Northside Hospital (Atlanta, GA) and Stanford University (Palo Alto, CA) in 2003 and 2004. This was one of the first robotic surgery courses ever offered.

Figure 1.14 Long description
The surgeon, dressed in surgical scrubs, is actively manipulating instruments. A monitor displaying the surgical field is visible in the background. The image appears to be the cover or part of a brochure for a medical course titled Hysteroscopy Laparoscopy and Introduction to Robotic Surgery. It lists course locations in Palo Alto, California (Stanford University Medical Center) and Atlanta, Georgia (Northside Hospital). Specific course dates are provided for 2003 (October second to fourth, December fourth to sixth) and 2004 (March fourth to sixth, May thirteenth to fifteenth, October twenty eighth to thirtieth, December second to fourth). The brochure also mentions course directors: Camran Nezhat, Doctor of Medicine; Ceana Nezhat, Doctor of Medicine; and Farr Nezhat, Doctor of Medicine. At the bottom, it specifies Nezhat Medical Center Endoscopy Laser Institute. A circular text box at the top right indicates Current trends covered, including ultrasonography, cryoablation, embolization, and more.
Over the subsequent two decades, more than 10000 physicians and surgeons attended these postgraduate courses, seminars, or live demonstrations facilitated by Dr. Camran Nezhat and his team, including his brothers Drs. Farr and Ceana Nezhat. Notable attendees from various parts of the world included, alphabetically listed, David Adamson, Veasy C. Buttram Jr., Steve Carson, Donald Chatman, Alan DeCherney, Celso-Ramon Garcia, Victor Gomel, Linda Guidice, Harriet Hassan, Grace Janik, Ron Levin, Carl Levinson, Barbara Levy, Cy Liu, Frank Loffer, Tony Luciano, Dan Martin, William Parker, Resad Paya Pasic, Hosanna Phillips, Mary Lake Polan, Harry Reich, Alvin Siegler, Radha Syed, Ray Valle, and Paul Wetter, among others. Many of these individuals served as presidents of the American Society for Reproductive Medicine (ASRM) or the AAGL at some point.
It is noteworthy that the majority of ASRM members, formerly known as the American Fertility Society, were also among the earliest to embrace MIS. The first MIS fellowship was established by the Society of Reproductive Surgeons (SRS) of ASRM, with Dr. Ceana Nezhat as its inaugural fellow, under the guidance of Dr. Camran Nezhat in Atlanta, Georgia. Later, this fellowship was jointly conducted by ASRM and AAGL before eventually separating to establish their own fellowships.
Additionally, numerous prominent international physicians and surgeons visited during this time, including Drs. Evo Brosens, Jacques Donnez, Bruno Vanderhaul, Maurice Bruhat, Gerard Mage, Jean Luc Poulley, Michelle Canis, Arnuald Wattiez, Ray Gary, Errico Zuppi, Marcelo Ceccaroni, Maurizio Rosati, George Hillaris, Cihat Unlo, and many others from around the world.
Attendees who saw Nezhat perform these advanced operations video laparoscopically walked away forever awakened to the new horizon. As word spread of a new surgical wunderkind, the early 1980s became a blur of nonstop travel, as Nezhat was invited to operate or present at countless medical society meetings around the world, including at the American Association of Gynecologic Laparoscopists 14th Annual Meeting, November 19–23, 1985, the American College of Obstetricians and Gynecologists in Washington, D.C., May 1985, the World Congress of Gynecology and Obstetrics in Berlin, West Germany, September 15–20, 1985, and the American Fertility Society’s (now ASRM) 41st Annual Meeting, September 28–October 2, 1985, to name just some of the earliest.
Still, publications continued to be significantly delayed due to repeat rejections by the editorial boards of academic medical journals [Reference Amara, Nezhat and Teng46,Reference Nezhat, Malik, Nezhat and Nezhat52–Reference Nezhat, Nezhat and Green76] (Figure 1.15). Eventually, though, Nezhat’s video laparoscopic treatment of extensive endometriosis was finally accepted for presentation and publication in 1985 and 1986, respectively.[Reference Carter3,16,Reference Nezhat19,Reference Nezhat and Page28,Reference Nezhat77] As for some of the more controversial surgeries, such as those involving advanced-stage ovarian cancer, there would be several year-long delays before these would gain acceptance for publication.
Nezhat just a few years later: notice how much smaller the video camera is here, compared to the one pictured in Figure 1.11. After industry realized that video laparoscopy not only had a future, but would be the future of surgery, they began producing smaller, safer, customized cameras made specifically with video laparoscopy in mind.

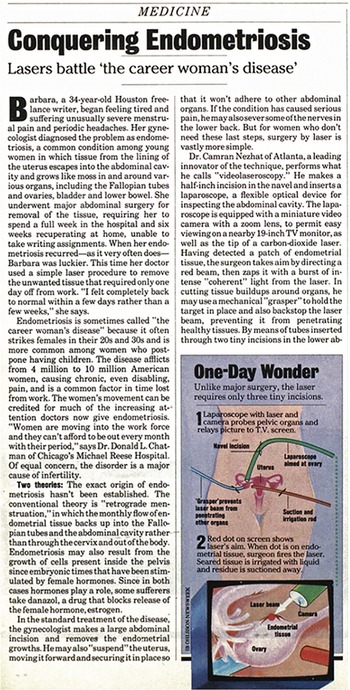
Eventually, the lay press picked up on these dramatic technological advancements in surgery, with Atlanta magazine featuring Nezhat on its cover in 1984, followed by national coverage in Time magazine in the April 28, 1986, issue, and in Newsweek magazine in the October 13, 1986, issue [Reference Wallis78,Reference Clark and Carroll79] (Figures 1.16 and 1.17).
In 1986, Camran Nezhat is featured in Time magazine [Reference Wallis78].

In 1986, Camran Nezhat raises awareness about endometriosis and minimally invasive surgical treatments in Newsweek magazine [Reference Clark and Carroll79].

Figure 1.17 Long description
A magazine titled Conquering Endometriosis Laser battle the career woman’s disease features two pictures. The first picture, titled One-Day Wonder, is labeled with: Navel incision, Laparoscope aimed at ovary, Uterus, and Suction and irrigation (red). The second picture is labeled with: Ovary, Camera, Laser beam, and Endometrial tissue.
Indeed, it seemed as if the public and the press couldn’t get enough of these fantastical, sci-fi surgery stories: videos and lasers and long metal sticks siphoning organs out of small holes, patients up and about in a day, all patched up with Band-Aids instead of sutures. Of course, the reality was not that simple. There was a lot of work to be done, namely perfecting the instrumentation, refining the procedures, and, most importantly, gathering sufficient clinical evidence to prove that this decidedly more difficult technique with a steep learning curve was providing benefits to patients that were more than just marginally better than traditional surgical techniques. But calls for temperance couldn’t stop the floodgates from bursting wide open in what we would recognize today as a viral moment. Nezhat’s phone began ringing off the hook with hundreds of requests by surgeons, patients, and the media to visit his OR or receive one of his videotapes so that they could confirm with their own eyes that these reports were real. Eventually, Semm and Nezhat were invited to debate the merits of traditional laparoscopy, which Semm called pelviscopy, versus video laparoscopy, in 1988 at the 3rd European Congress on Hysteroscopy and Endoscopic Surgery in Amsterdam, the Netherlands, marking a watershed moment where the tipping point away from analog and toward modern-day digital MIS was occurring right before our eyes. Dr. William Saye was another early visitor to Nezhat’s operating room. Later, Saye became renowned for pioneering the first video laparoscopic cholecystectomies in the US in 1988 and 1989, leading his team consisting of Drs. McKernan, Reddick, and Olsen.
Dr. Camran Nezhat engaged in several other notable debates during the late 1980s and early 1990s. On November 9, 1988, at the AAGL conference, Nezhat discussed the advantages of video laparoscopy and operating on the monitor with Dr. Richard Soderstrom. Additionally, Nezhat debated the topic “Should the Conservative Surgical Management of All Stages of Endometriosis in the Infertile Female Be Performed Almost Always by the Endoscopic Route?” with Dr. Joseph Feste at the 2nd International Symposium on Endometriosis held May 1–3, 1989, at the Westin Galleria Hotel in Houston, Texas.
It was through these various inroads – national lay press articles, meetings, publications, mailed videotapes, visits to his OR in Atlanta – that Nezhat’s work gained even more global recognition, and invitations continued to pour in.
One of the most memorable came from Bruhat, who invited Nezhat to deliver a presentation at the University of Clermont-Ferrand in France in 1985. During this visit, Nezhat had the opportunity to work with some of France’s foremost laparoscopists, such as Mahnes, Canis, Wattiez, and Pouly, along with the pioneering American surgeon Harry Reich, who later adopted Nezhat’s techniques to report the world’s first video laparoscopic hysterectomy in 1989. Nezhat’s groundbreaking work also left a lasting impact on other French pioneers of that era, including Mouret, who subsequently conducted the world’s second laparoscopic cholecystectomy in 1987, after Erich Mühe’s first in 1985. Dr. Camran Nezhat met Dr. Mouret again at the International Workshop of Operative Laparoscopy in Vichy, France, April 26–27, 1988, where he, along with Dr. Hubert Mahnes, were co-presidents. Though Mouret initially performed this groundbreaking procedure in the traditional manner of peering through the scope, he would later convert to video laparoscopy, as would French general surgeons Francois Dubois and Jacques Perissat, who went on to perform among the earliest video laparoscopic cholecystectomies by approximately 1988–1989. Many medical historians leave out this sequence of events, but these were the precipitating developments that persuaded general surgeons from academic centers around the world to begin adopting video laparoscopy. General surgeons themselves mark 1989 as one of the most critical tipping points for their discipline when Perissat presented his videotape of a video laparoscopic cholecystectomy at the annual Society of American Gastrointestinal Endoscopic Surgeons (SAGES) meeting in Louisville, Kentucky, an event memorialized in a 1999 SAGES Presidential Speech as follows:
Ten years ago something happened at this meeting that forever changed the future of the Society of American Gastrointestinal Endoscopic Surgeons (SAGES). Jacques Perisatt … brought to the meeting a videotape of a laparoscopic cholecystectomy that he performed in Bordeaux, France… . After watching Dr. Perisatt’s video, the leaders of SAGES started whispering to each other: “Should we be involved? Is laparoscopy for us?” By the autumn of 1989, at the American College of Surgeons (ACS) meeting in Atlanta, the answer was clear. Yes, SAGES would do laparoscopy … [Reference Hunter80]
With Wickam coining the catchy new term of minimally invasive surgery in 1987 and opening Britain’s first MIS center, the burgeoning new digital era of tiny incision surgery was poised to cause a sea change that finally began rippling throughout all disciplines of surgery in the late 1980s and early 1990s.
Nezhat continued to apply video laparoscopy to various subspecialties, such as urology, colorectal surgery, thoracic surgery, and urogynecology. Facilitated by the many instrument innovations he would make, with over 30 patents, Nezhat went on to perform the first laparoscopic bowel, bladder, ureter, and diaphragm resection and reanastomosis, along with laparoscopic sacrocolpopexy, vesicovaginal fistula repair, and excision of liver endometriosis, initially reported between 1989 and 1994.[Reference Carter3,Reference Kelley4,16,Reference Nezhat and Nezhat63] Nezhat also introduced the safe laser excision and vaporization of endometriosis, extending his expertise to encompass extragenital endometriosis and deep infiltrating endometriosis, including cases involving the rectovaginal septum.[Reference Nezhat and Nezhat64,Reference Nezhat, Nezhat and Pennington69] Notably, in 1989, Nezhat and his team also performed the groundbreaking first laparoscopic radical hysterectomy with para-aortic and pelvic node dissection, a complex procedure lasting seven hours, which was published in June 1991.[Reference Nezhat, Burrell, Nezhat, Benigno and Welander74,Reference Nezhat, Nezhat and Burrell75] With these early successes, Nezhat firmly asserted that wherever a cavity exists or can be created in the body, MIS is not only possible but also often preferable. The limiting factors, he emphasized, are the surgeon’s skill and experience, along with the availability of proper instrumentation. Dr. Alan DeCherney, of the National Institutes of Health, was one of the earliest to recognize Nezhat’s contributions and aptly captured his trailblazing efforts, stating, “Like Star Trek, Camran went where no man had gone before, opening new frontiers for surgeons across the globe.” In 2000, Kurt Semm also acknowledged Nezhat’s central role in advancing MIS, affirming, “With his genius, he expanded the operative field, introducing innovative techniques and utilizing new instruments and apparatuses. Collaborating with his two brothers, Camran enriched the entire domain of surgical laparoscopy.”[Reference Nezhat and Page28]
Patient Demand for Video Laparoscopy Drives Progress
It wasn’t just surgeons who were expressing a viral interest in learning about video laparoscopy. Patients themselves, having read the same mainstream news articles, began demanding that their surgeons perform these new “Band-Aid” surgeries. With patient-driven demand seeming to now drive the bus, so to speak, it marked a profound departure from centuries of traditional paternalistic medicine, where doctors held nearly unquestioned authority over the lives of patients. Meanwhile, mainstream media continued to report on Nezhat, including Newsweek again in 1990, with glowing descriptions of miraculous, seemingly bloodless surgeries (Figure 1.18). Unfortunately, though, it triggered a new wave of growing concerns among the academic medical community, which had become unsettled by the radical technological changes that not only had occurred seemingly overnight but also appeared to have breached the normal gatekeepers of medicine with unstoppable patient-led momentum.
In a 1990 issue of Newsweek magazine, Camran Nezhat openly advocates for the advantages of minimally invasive techniques and boldly predicts, “In 20 years, major abdominal surgery will be nearly extinct.”

Indeed, it wouldn’t be long before battle lines would soon be drawn. Even so, throughout this era, a new generation of pioneers continued to push forward progress, including Dan Martin’s award-winning innovations in the US, especially with the use of laser laparoscopy for the treatment of ovarian cystectomy in 1984.
Organizational innovations continued with the establishment of the SAGES in 1981, founded by Gerald J. Marks, MD. The Chinese Society of Digestive Endoscopy (CSDE) was founded in 1985 as part of the Chinese Society of Gastroenterology and later became an independent organization in 1991. In 1987 the first issue of the journal Surgical Endoscopy was published, and in 1988 the first World Congress of Endoscopic Surgery was held in Berlin, (then) West Germany. And, just two years later, in 1990, Dr. Paul Wetter founded the Society of Laparoendoscopic Surgeons (SLS), now the Society of Laparoscopic and Robotic Surgeons.
Endometriosis’s Role in Shaping Surgical History
Patients with endometriosis, in particular, played an especially central role in shifting surgery toward minimally invasive methods. Often invisible to the naked eye, inscrutable in its etiology, for most of the twentieth century, endometriosis had defied understanding, causing many patients with the excruciating condition to be just as likely to be sent to a psychiatrist as a gynecologist, their inexplicable, multi-organ symptoms mistaken as psychosomatic disorders instead. Some reports even suggested that women with pelvic pain without apparent organic basis tended to be more emotionally disturbed, neurotic, or hysterical than those without such symptoms.[Reference Nezhat, Nezhat and Nezhat81–Reference Wilde84] Lingering beliefs associating pelvic pain with promiscuity also meant that patients were sometimes blamed for their illnesses. Women from US minority communities were especially susceptible to being misdiagnosed with diseases that implied sexual transgression. One study from 1993 found that “as many as 40 percent of African American women [were] misdiagnosed as having a sexually transmitted pelvic inflammatory disease (PID) when in fact they [suffered] from endometriosis.”[Reference Williams85] Also, a 1995 study reported that, on average, up to 50% of patients complaining of chronic pelvic pain were found to have no apparent organic basis after surgical evaluation. This meant that nearly half of all women seeking medical care for pelvic pain were susceptible to receiving inadequate care, enduring unflattering assumptions about their character, or being viewed as suffering from imaginary ailments.[Reference Gomel and Taylor86,Reference McCracken87] Additionally, in a study conducted in 2020, the mean reported diagnostic delay of endometriosis remained at 8.6 years.[Reference Bontempo and Mikese88] In this large sample of surgically confirmed endometriosis patients, these women had to wait an average of 8.6 years to receive a proper diagnosis and therefore medical treatment. In sum, even though the large incisions of laparotomies should have helped practitioners detect its presence, endometriosis continued to evade the clinical gaze.
Video Laparoscopy Helps to Secure Greater Understanding of Disease States
It was not until late in the twentieth century that the multitude of morphologies the disorder can take was more fully recognized, a change attributed to video laparoscopy, which began displacing laparotomy as the preferred diagnostic and operative modality for endometriosis during the same time frame.[Reference Bontempo and Mikese89,Reference Hunt90]
Like many of his colleagues familiar with the confounding disorder, Nezhat suspected endometriosis was the cause behind many enigmatic symptoms, even when the anatomy initially appeared normal. When he pioneered video laparoscopy, Nezhat was able to consistently visualize atypical lesions that could have easily been mistaken as normal tissue but that now, under video magnification, could be clearly seen as pathological formations. He had never obtained such stunning visualization while performing diagnostic laparoscopies in the old method of peering into the eyepiece or even from the vantage point of the supposedly superior views afforded by the large incisions of open surgery.
With an improved ability to see pathologies that had gone undetected, video laparoscopy began contributing to an era of greater understanding of the true nature of endometriosis, as well as many other disorders. Now Nezhat was able to find organic causes in patients more than 90% of the time.[Reference Dumesic91] By the late 1980s, he and other newly converted video laparoscopists began reporting clinical findings that overturned nearly a century of statistics that had misrepresented endometriosis’s true prevalence and proclivities, finally uncovering what patients had been suffering from all along.[Reference Perper, Nezhat, Goldstein, Nezhat and Nezhat92–Reference Moore, Copley and Morris99]
Regarding the 50% of patients from the 1990s initially believed to have no organic cause to their pelvic pain, as it turned out, reports began to surface in the early 2000s indicating that endometriosis had been routinely overlooked in the days before video laparoscopy as often as 50% of the time.[Reference Koninckx100,Reference Soriano, Yefet and Seidman101] Just as importantly, as a result of the more accurate data obtained using video laparoscopy, Nezhat uncovered surprising new insights about endometriosis, including research that suggests that endometriosis is at least a 50% genetically driven disorder, which has been in existence for thousands of years and most likely affects as many as 25–30% of women and adolescent girls, including some premenarchal, as well as an unknown number of men, transgender, intersex, and non-binary individuals globally.[Reference Wallis78,Reference Clark and Carroll79] Given a world population estimated at about 8 billion and assuming approximately half to be female, this would mean that an estimated 874 million to 1.04 billion individuals either have had, will have, or currently do have endometriosis.[Reference Cullen102] These figures are strikingly higher, by 5–6 times, than the 178 million commonly cited as the estimated number of endometriosis sufferers worldwide.
Bowel, Bladder, Ureter, Diaphragm, Lung, and Liver Endometriosis
Having identified a correlation between pain relief and improved fertility rates when treating endometriosis thoroughly, Nezhat chased down endometriosis wherever it appeared, a fact which ultimately led him to examine bowel, bladder, ureter, diaphragm, liver, and lung endometriosis. Many don’t realize it, but video laparoscopic cholecystectomy and appendectomy are actually some of the least complex laparoscopic procedures to perform, which is why they were the starting points for many early converts to video surgery. In contrast, surgeries involving the bowel, bladder, and ureter have been considered some of the most challenging to perform minimally invasively, and even during the days of laparotomy. This sentiment was expressed as early as 1919, when Thomas Cullen, one of the earliest American specialists in endometriosis, declared bowel surgeries for endometriosis to be “infinitely more difficult than [even] hysterectomies for carcinoma.”[Reference Cullen102]
Yet, after combining video laparoscopy with a CO2 laser, which provided a more controllable and predictable energy source than electrocautery, Nezhat and colorectal surgeon Dr. Earl Pennington achieved a groundbreaking advancement by becoming the first to achieve a video laparoscopic bowel resection and reanastomosis for deeply infiltrating endometriosis. After again facing difficulty in having their results published, they independently presented the data in 1988 and finally published the results from 1989 to 1992.[Reference Amara, Nezhat and Teng46,Reference Nezhat, Malik, Nezhat and Nezhat52–Reference Nezhat, Nicoll and Bhagan54,Reference Nezhat, Nezhat, Nezhat and Rottenberg59,Reference Nezhat and Nezhat63,Reference Nezhat, Nezhat and Pennington66–Reference Nezhat, Burrell, Nezhat, Benigno and Welander74,Reference Nezhat, Nezhat and Green76] For the delicate procedures for treating endometriosis of the bladder and ureter, Nezhat applied this same combination of techniques with unprecedented success, navigating around the frozen pelvises that such extensive disease creates and eventually completing a fully video laparoscopic segmental bladder resection, ureter resection, and reanastomosis for the first time.[Reference Duncan and Taylor82,103]
Poor Resolution Almost Foils the Advance
Unfortunately, the era’s existing technologies were not advanced enough to support video surgery to its fullest potential. Specifically, operating off the monitor was barely feasible because the early-generation optics, TV, and video systems could not produce the level of high-pixel resolution needed to make the images of the anatomy clearly visible when projected onto the monitor. Nezhat attempted to avert these deficiencies by using an extra endoscope to provide additional illumination (Figure 1.10). Still, this failed to solve the problem. This was because, even by the late 1980s, the highest level of resolution in medical TV monitors and cameras was still only between 275 and 450 lines, no match for the naked eye.[Reference Beard, Belsey, Lieberman and Wilkinson83] Even despite the superior illumination afforded by the latest fiber optics, it was still not enough to effectively split the images toward the monitor. “Illumination sources are in a chaotic state” is how one frustrated surgeon described the situation as it stood in 1977.[Reference Berci and Mitchell31] One exception was in the field of orthopedic surgery, where video laparoscopy enjoyed early and wide acceptance due to the bone being white, which meant less lighting was required. Modest improvements were made when more advanced technologies were finally invented, such as beam-splitters like the ones introduced by Japanese company Topcon in 1981.[Reference Hadley33] Sophisticated new optics eventually hit the market, too, including high-refractive fiber optics coated with a thin film of magnesium fluoride to help decrease the otherwise nearly 30% loss of light that commonly occurred with earlier versions.[Reference Hadley33]
However, these technologies were not always widely available. With the benefits of video surgery still not readily perceived, along with the unpalatably substantial capital costs involved in its initial setup, most found it challenging to secure funding for the needed upgrades. Thus, throughout the 1980s–1990s, many centers continued to use outdated endoscopes, lighting, and TV monitors, making it difficult for other surgeons to replicate Nezhat’s results, which had been achieved using the most advanced technologies on the market.
Forever-Scopy
Video laparoscopy was also certainly not without other flaws. One of its least attractive features was the extra time it took for most new converts to perform advanced procedures, so much so that video laparoscopy earned the nickname “forever-scopy.” During this extended learning curve, for example, laparoscopic ectopic pregnancy surgeries were taking up to 4–5 hours, while Nezhat’s – and the world’s – first laparoscopic radical hysterectomy with para-aortic and pelvic lymphadenectomy actually took 7 hours. In contrast, Nezhat can perform the same procedure today in less than 35 minutes.[16,Reference Nezhat19,Reference Nezhat77]
Although today many minimally invasive surgeries are commonly completed in less time than open procedures, during the early days, this wasn’t the case, making the increased duration a factor that wasn’t helping to convince anyone that video surgery was better or safer than large incision surgeries.[Reference Crosignani and Vercellini104,Reference Shushan, Mohamed and Magos105] The loss of haptic feedback has also been one of the more challenging changes to adjust to. Without the ability to palpate organs, it’s difficult for surgeons to estimate the physical force needed to handle tissue or determine how extensively organs have been affected by pathology. Insufflating the abdomen also brought with it special new categories of complications. Eventually, though, robotic surgery re-introduced some haptic-like features, while insufflation issues ultimately resolved after Fishburne and other innovators invented new anesthetic techniques that were more suitable for the deep Trendelenburg positioning and insufflation pressures that came with the territory.[Reference Soderstrom93,Reference Siegler and Berenyi106]
Oncology and Video Laparoscopy
One of the most serious initial concerns raised about video endoscopy was the belief that it would lead to iatrogenic spread or upstaging of known or occult neoplasms. Specifically, tumor spillage and port-site metastasis were thought to be more likely if surgeons attempted to remove neoplasms through the tiny laparoscopic port holes instead of through a large laparotomy incision.[Reference Warshaw, Tepper and Shipley107–Reference Grimes109] And no one could deny that MIS may not be able to offer what a laparotomy could: the ability to digitally palpate suspicious-looking nodules, the most deified surgical feedback of all time.
Dr. Camran Nezhat in collaboration with Drs. Matthew Burrell, Benedict Benigno, Nelson Tang, and Farr Nezhat were the earliest pioneers to challenge these assumptions, achieving in 1989 the first laparoscopic radical hysterectomy with para-aortic and pelvic node dissection in cervical and ovarian cancer, and subsequently published in 1991.[Reference Nezhat, Nezhat and Silfen73–Reference Nezhat, Nezhat and Burrell75] Many refused to believe the procedure had even been performed at all, asserting that “it is at this time impossible to explore paraaortic nodes by laparoscopy.”[Reference Cullen102] More than anything, though, even early advocates of video laparoscopy felt that the Nezhats had gone too far this time, proof that they were letting “their enthusiasm run ahead of their science.”[Reference Nezhat, Burrell, Nezhat, Benigno and Welander74,Reference Nezhat110] Even with growing condemnation, the field advanced, and other early pioneers in video laparoscopic oncology include Jo Childers, Daniel Dargent, Denny Querleu, Achim Schneider, Marc Passover, Michel Canis, and many others.
In 1992, Dr. Nezhat received an invitation from Dr. John Lewis, the former chair of OBGYN at Memorial Sloan Kettering Cancer Center, to serve as a visiting professor for a week from May 18 through May 22. Throughout his stay, Dr. Nezhat engaged in lectures and live surgery demonstrations, where he discussed and performed surgery for cases such as laparoscopic radical hysterectomy and para-aortic and pelvic node dissection. Additionally, in the Department of Surgery, Dr. Nezhat demonstrated a laparoscopic bowel resection under the chairmanship of Dr. Murray Brennan.
Vulnerable Patients Are the Ones Who Needed MIS the Most
As a result of these deeply entrenched apprehensions, it wouldn’t be until the mid-2000s that patients with cancer would finally be spared the burden that open surgery often exacted upon their already beleaguered bodies. Farr Nezhat could see that it was going to take a lot more than a few successful surgeries for oncology to break free from beliefs that had stood unchallenged for centuries. He decided to redirect his energies toward earning board certification in gynecologic oncology, seeking out the tutelage of Dr. Carmel Cohen, one of the world’s leading pioneers in the field. With specialized training now secured, Farr Nezhat achieved groundbreaking firsts, including the first laparoscopic and robotic-assisted radical hysterectomies, laparoscopic staging, and tumor debulking in advanced cancer.[Reference Nezhat72–Reference Nezhat, Nezhat and Burrell75] Contemporary studies have substantiated that “tumor-free margins … and lymph node dissection counts secured by MIS have all been demonstrated to be equivalent to those achieved with conventional open surgery.”[15,Reference Nezhat, Cohen and Rahaman111–Reference Acholonu, Chang-Jackson, Radjabi and Nezhat114]
The Era of Hostility
Amidst glowing lay press reports that described seemingly miraculous results still inundating the airwaves, it wasn’t long before concerns about the accuracy of Nezhat’s data, in particular, began to surface. Skeptics were particularly incredulous at Nezhat’s extremely low rate of complications. It all seemed so suspicious, technological and biological aberrations almost too good to be true.[Reference Wallis78,Reference Clark and Carroll79,Reference Nezhat110,Reference Pitkin115] Eventually, much like Semm, Muhe, and so many other surgical pioneers, Nezhat became a favorite target of derision for many years. Even though by this time, more than 20 years of sound clinical data proved MIS could spare patients from many severe complications that were more common in open surgeries, it continued to be met with nearly universal ridicule for most of the twentieth century and even into the first decade of the twenty-first century. “Why look through the keyhole,” skeptics quipped, “when you can open the door?” In terms of endoscopy’s history, such responses were far from unique, as resistance to unconventional ideas had nearly derailed progress since Bozzini and beyond. Yet, opposition to operative video laparoscopy proved to be especially fierce, for it forced surgeons to lose three vital sensory mechanisms: tactile, spatial, and direct visualization.[Reference Dubois, Icard, Berthelot and Levard116,Reference Clarke117]
It didn’t help that many prominent figures in the field of laparoscopy, including Dr. Kurt Semm in Germany, Drs. Dan Martin and Jim Daniel in the US, and many others, were also initially opposed to video laparoscopy and continued to perform their laparoscopic procedures by looking through an eyepiece. Dr. Dan Martin, Professor Emeritus of the University of Tennessee, Memphis, the current Scientific and Medical Director of the Endometriosis Foundation of America, and a Community member of the Virginia Commonwealth University Institutional Review Board, recalled his initial hesitancy occurring as early as 1982, when Nezhat presented video laparoscopy as part of a training workshop. Reflecting on this first meeting with Nezhat, Martin noted in recent communication dated October 8, 2023, “I have told many how I told you [Dr. Camran Nezhat] it [operative video laparoscopy] would not work from when we first met in July 1982 until 1986, when my students wanted me to teach them your techniques. You let me join you in Atlanta so I could learn your techniques and teach them” (Figure 1.19).
In this picture, which was taken by Dr. Dan Martin and shared with us, Dr. Camran Nezhat is looking through the eyepiece of the laparoscope.

Yet, the decisive tipping point began in the late 1980s after the mainstream media had picked up the story and when it became clear that video laparoscopy had breached beyond gynecology, finally infiltrating the hitherto untrammeled territory of general surgery. Although gynecologic surgeons had already achieved some of the most complex operative procedures laparoscopically by the early 1980s, it was the rapid transformation that ensued after the first series of video laparoscopic cholecystectomies had been performed in the late 1980s, which seemed to have become the proverbial last straw, pushing dissenters over the edge into growing defiance against anything with “scopy” in its name.
By the late 1990s, opposition had transformed into searing hostility toward those who dared to flout convention that would scour the MIS landscape. The first provocateurs published articles questioning MIS with such titles as “Operative Laparoscopy: Surgical Advance or Technical Gimmick?”[Reference Pitkin115] Soon the literature was teeming with similar accusations of intemperance, with another author stating, “After several years of euphoria with the laparoscope, surgeons have started to look critically at the extravagant claims of minimal-access surgery.”[Reference Barham118]
Even as recently as 2003, some continued to call into question the safety and necessity of video laparoscopy, insinuating the worst with rhetoric such as “just because we can [do endoscopy] doesn’t always mean that we should” [Reference Advincula119] (Figure 1.20). The same article goes on to implicate excesses of industry and the “glitz” of new technology as culprits with the following:
Surgical technology in the area of endoscopy seems to be exploding, but at what cost? … Today, I ask the question: Who is driving the bus? Industry or physician? The focus on the basic principles of surgery is fast becoming blurred amongst the glitz of new technology.[Reference Seidman and Nezhat121]
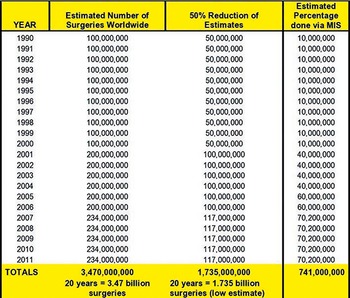
Extrapolations calculated based on several articles, including a 2008 WHO article, “An Estimation of the Global Volume of Surgery: A Modelling Strategy Based on Available Data,” by TG Weiser, SE Regenbogen, KD Thompson, et al., The Lancet, 2008;372:139–144.[Reference Weiser, Regenbogen and Thompson120]

Figure 1.20 Long description
The table has four columns: Year, Estimated Number of Surgeries Worldwide, 50 percent Reduction of Estimates, and Estimated Percentage done via minimally invasive surgery. It reads as follows: Row 1: 1990; 100,000,000; 50,000,000; 10,000,000. Row 2: 1991; 100,000,000; 50,000,000; 10,000,000. Row 3: 1992; 100,000,000; 50,000,000; 10,000,000. Row 4: 1993; 100,000,000; 50,000,000; 10,000,000. Row 5: 1994; 100,000,000; 50,000,000; 10,000,000. Row 6: 1995; 100,000,000; 50,000,000; 10,000,000. Row 6: 1996; 100,000,000; 50,000,000; 10,000,000. Row 7: 1997; 100,000,000; 50,000,000; 10,000,000. Row 8: 1998; 100,000,000; 50,000,000; 10,000,000. Row 9: 1999; 100,000,000; 50,000,000; 10,000,000. Row 10: 2000; 100,000,000; 50,000,000; 10,000,000. Row 11: 2001; 200,000,000; 100,000,000; 40,000,000. Row 12: 2002; 200,000,000; 100,000,000; 40,000,000. Row 13: 2003; 200,000,000; 100,000,000; 40,000,000. Row 14: 2004; 200,000,000; 100,000,000; 60,000,000. Row 15: 2005; 200,000,000; 100,000,000; 60,000,000. Row 16: 2006; 234,000,000; 117,000,000; 70,200,000. Row 17: 2007; 234,000,000; 117,000,000; 70,200,000. Row 18: 2008; 234,000,000; 117,000,000; 70,200,000. Row 19: 2009; 234,000,000; 117,000,000; 70,200,000. Row 20: 2010; 234,000,000; 117,000,000; 70,200,000. Row 21: 2011; 234,000,000; 117,000,000; 70,200,000. Row 22: TOTALS; 3,470,000,000 20 years equal to 3.47 billion surgeries; 1,735,000,000 20 years equal to 1.735 billion surgeries (low estimate); 741,000,000.
Threats of Lawsuits Scared One Journal into Retracting Articles
When all was said and done, Nezhat and his brothers, Drs. Farr and Ceana, withstood accusations of barbarism, commercialism, and even medical terrorism.[Reference Nezhat110] At the height of this absurdity, the FBI, IRS, the criminal division of the Justice Department, and multiple state medical boards were all chasing after Nezhat, with countless false accusations now being reported in the press as well. So suspect had the new surgical revolution become that he and his brothers ultimately had their academic integrity called into question. When a new dean at Stanford University felt pressured to answer to the public fervor that had developed, he chose the most politically expedient action by launching a highly publicized, formal investigation into Nezhat’s work, issuing in the process a temporary suspension of his professorship to appease the public outcry. Gynecologists have been viewed with particularly harsh skepticism throughout the ages, referred to by such derisive names as “baby catchers and uterus snatchers.”[Reference Scully122] And so it seemed that the tabloids somehow tapped into these ancient underlying sentiments about the field of gynecology, and such was the power of propaganda that the mere suggestion of impropriety was enough to convict Nezhat in the eyes of the public.
The Long Journey Back
Back at Stanford, top brass from around the country – including experts from Harvard and former state supreme court justices – were convened to form a Blue Ribbon committee tasked with examining the allegations that the accusers had offered as evidence against Nezhat. They poured over thousands of documents and crisscrossed the nation interviewing hundreds of physicians, patients, nurses, technicians, and other medical personnel who had worked side by side with Nezhat for years in the operating room. In the end, the Blue Ribbon committee determined that all of the allegations were unsubstantiated and without basis.[Reference Nezhat110] After the Blue Ribbon committee released their findings, Nezhat’s work was finally cleared by the highest authorities from Stanford University, two state supreme courts, and the California and Georgia state medical boards.[Reference Perlman123]
In what can only be described as one final bizarre twist, just a few years after this slew of false allegations, studies began pouring forth that confirmed Nezhat’s initial impressions of video laparoscopy’s advantages.[Reference Yong, Law, Lo and Lam124,Reference Rashid, Goad, Aron, Gianduzzo and Gill125] Not only this, but the very procedures that triggered Nezhat’s suspension just two years earlier, the ones referred to as “barbaric,” were now being encouraged by the most prestigious journals.[Reference Nelson17,Reference Pappas and Jacobs18] Referencing the same procedures that Nezhat had performed in the mid-1980s, a 2004 editorial from the New England Journal of Medicine stated, “Surgeons must progress beyond the traditional techniques of cutting and sewing … to a future in which … minimal access to the abdominal cavity [is] only the beginning.”[Reference Pappas and Jacobs18] Meanwhile, a once-skeptical editor of a prestigious obstetrics and gynecology journal, who had summarily dismissed video laparoscopy as a gimmick in 1992, conceded in a 2010 article that “operative laparoscopy confers unequivocal advantages over older surgical techniques.”[Reference Pitkin and Parker126] In the final analysis, it is Nezhat’s method of MIS – video-assisted endoscopy – that has replaced all previous forms of endoscopy and is now being taught at every medical school around the world.
The Legacy of MIS: A New Surgical Philosophy Is Born
Operating off the images on the TV monitor and inventing the accompanying advanced procedures – and then performing them successfully – were the crucial links that allowed surgery to be freed from large incisions and hundreds of years of history of peering directly through a tube, specula, or scope. Most accounts of video laparoscopy’s history leave out its formative years when Nezhat was at the forefront, balancing on the brink, struggling between the exhaustive extremes of dreaming and doubting. In fact, many set video laparoscopy’s launch date as the late 1980s, after general surgeons had finally discovered its teeming shores after its happy destiny was already underway. Yet, a laparoscopic cholecystectomy – the starting point for most general surgeons – did not come to be via immaculate invention. For that procedure to have been possible at all, the old method of performing laparoscopy – hunched over, peering into the eyepiece – had to be completely abandoned and replaced with a way that made more advanced operative procedures safe, feasible, and reproducible on a broad scale. And the person who delivered that critical change was Nezhat.
When he introduced the idea of projecting the surgical images onto a TV screen and operating off the images, Nezhat provided the platform that made it possible for operative procedures to actually be practicable on a large scale.[Reference Podratz2–Reference Kelley4] While a few surgeons – perhaps a half dozen – had used the laparoscope to perform a limited number of basic operations in the old way, the vast majority would never be able to perform advanced operative endoscopic procedures of any kind by peering into the eyepiece. It was essentially this one factor, as unassuming as it may seem today, that had actually stood in the way of nearly all operative progress. The impact has been profound. In the early 1980s, before video laparoscopy had yet to be embraced, the majority of all operations worldwide were performed using large incisions, meaning that upwards of 50–100 million people each year underwent procedures fraught with painful and often debilitating effects that could take months to recover from, while others were left with permanent pain, disability, or organ dysfunction.[Reference Nezhat, Nezhat and Nezhat127] Since its official launch in the early 1980s, more than a billion people and counting are now being spared such outcomes as a result of MIS, and billions more at least now have the option of choosing a safer form of surgery (Figure 1.20).
By introducing a medical breakthrough that so drastically reduced surgical morbidity and mortality on such a global scale, Nezhat’s work has indirectly saved countless lives and profoundly improved millions of others, one of the few true advances in medicine that our world has witnessed for generations. Authorities such as the New England Journal of Medicine now recognize the advent of video laparoscopy as the crucial catalyst responsible for inaugurating MIS as a viable surgical discipline, a change that is said to have “revolutionized the practice of surgery, just as antibiotics have changed the practice of medicine.”[Reference Pappas and Jacobs18;Reference Podratz2–Reference Kelley4,Reference Schropp, Lobe and Schropp128]
Video laparoscopy not only brought about a revolution in all surgical disciplines, but it also played a pivotal role in paving the way for the era of robotic surgery, as the conceptual framework for making this paradigm shift was now established. Today, the most widely utilized robotic surgical system is the Da Vinci robot, developed by a team led by Dr. Ajit Shah and Phil Green at Stanford Research International in collaboration with Camran Nezhat, MD.[Reference Nezhat, Nezhat and Nezhat127] This advanced system is equipped with a robotic arm controlled through a computer console, and which includes haptic feedback, anti-tremor technologies, 100-fold magnification, and an impressive 7 degrees of rotation, which exceeds the capabilities of the human hand, which has only 5 degrees of rotation. Taken together, the system enables a broader number of surgeons to more easily perform minimally invasive procedures.
Perhaps of greatest significance, the profound shift away from traditional open surgery to minimally invasive modalities set off intense scientific and philosophical debates, calling into question centuries of unexamined assumptions about pain, patient rights, disease states, and surgical complications. Today, paternalistic medicine has largely fallen out of favor with patients, who increasingly expect a more collaborative approach in shaping their healthcare decisions. This shift is evident in the rise of patient-driven global movements like the Worldwide EndoMarch, where individuals with endometriosis unite together to advocate for their healthcare needs and urgently needed policy changes.
An entirely new way of thinking about surgery’s role in health outcomes emerged as well, one that catalyzed a long-overdue moment of reckoning when all surgical traditions were finally held up to the light of scrutiny. For example, with the new minimally invasive philosophy leading the way, a dramatic paradigm shift in gynecologic surgery emerged, one that emphasized the preservation of reproductive organs – a minimally invasive approach – as the new standard of care rather than the exception. Of equal importance, it wasn’t just the category of surgery that was reevaluated. Rather, questions arose having to do with a wide range of medical issues, with concepts relating to pain management emerging as one of the most critical changes to have come about due to the minimally invasive movement.
Complications Once Considered Unavoidable Now Being Reevaluated
An eventual rethinking in expectations about surgical outcomes also arose. Complications once considered unavoidable in the days of open surgery were suddenly reevaluated and revised in the minimally invasive era. By now, of course, there’s probably not a physician on the planet who isn’t familiar with minimally invasive surgery’s main advantages: smaller incisions, faster recovery, less pain, decreased blood loss, fewer adhesions, fewer complications, few hospitalizations, better results, better personal and societal results, and less expensive, too. However, after video laparoscopy became available as an alternative to laparotomy, patients, as well as physicians, were also able to finally recognize just how many serious, permanent, and life-threatening complications, including a higher incidence of death, large incisions had imposed on patients.[Reference Podratz2,15,Reference Bozzini21,Reference Berci37,Reference Phillips41,Reference Nezhat, Nezhat, Gordon and Wilkins57,Reference Williams86] Although these open methods were convenient for the surgeon, the large incision wounds actually caused patients to undergo acute, multi-organ distress. Excessive injury to tissue activates a cascade of deleterious physiologic mechanisms, with the systemic inflammatory process alone causing the release of a bewildering array of tissue-damaging enzymes like fibrinogen, plasminogen activators, and tissue thromboplastin. Since the inflammatory response is actually maintained long after the initial surgery, a patient’s health can deteriorate for weeks after a large incision surgery, while a chronic condition of “continued malfunction of one or more organ systems can occur, despite … the absence of persistent infection, and other identifiable insults.”[Reference Schropp, Lobe and Schropp129]
By today’s standards, the loss of blood was staggering as well, often exceeding 1000 ml and necessitating large-volume blood transfusions in up to half of all cases. Life-threatening pulmonary embolisms were significantly more common with open surgery than with MIS. Serious, chronic wound disorders, particularly wound dehiscence, were also once considered nearly inescapable, with the potential to leave patients in pain for months or even years with incisions that just wouldn’t heal.[Reference Handa and Le130–Reference Bucknall, Cox and Ellis132]
The extensive adhesion formations after large incision surgeries also had the potential to cause years of severe complications, including compromised organ function and chronic pain, all of which were completely unrelated to the original illness. While any form of surgery can produce adhesions, laparotomies cause significantly more severe and extensive adhesions and occur in an estimated 93% of cases. Of those, studies have shown that within 1 year, up to 33% require an additional open surgery – possibly even more than one – to manage the potentially life-threatening bowel obstructions that develop. And of these, some studies have found that up to 8% end fatally. Extrapolating from multiple studies, this means that each year potentially more than a million patients in the US alone could be at risk for developing an entirely new set of debilitating conditions and severe morbidity, all stemming from their original open surgery.
The minimally invasive philosophy has also helped reduce what were incredibly high rates of unnecessary removal of healthy organs in the days before video-assisted endoscopy. For example, unnecessary appendectomies, sometimes referred to euphemistically as negative or nontherapeutic appendectomies, occurred – and still do, unfortunately – when patients were misdiagnosed as suffering from a life-threatening case of a ruptured appendix.[Reference Deutsch, Zelikovsky and Reiss133] Such diagnostic missteps were significantly more common before video-assisted endoscopy, with as many as 20–44% of all open appendectomies performed proving to be unnecessary. For women, the figure was even higher, with as many as 52% of open appendectomies proving to be unwarranted, according to some studies.[Reference DeArmond, Dent and Myers134–Reference Balthazar, Rofsky and Zucker140]
In a study conducted in 1999, C. Barrat et al. investigated the incidence rate of finding histologically normal appendices after conducting laparoscopic exploration versus an open appendectomy. It was found that in the open-appendectomy group, the rate of histologically normal appendices found postoperation was 25.1%, while in the laparoscopic exploration group, it was only 8.2%.[Reference Barrat, Catheline, Rizk and Champault141] The study provided statistical evidence that performing appendectomies laparoscopically significantly reduced the number of unnecessary procedures. This is due to the fact that oftentimes when a patient presented with the common symptoms of right iliac fossa guarding and leukocytosis greater than 10 000, only a laparoscopic exploration was able to differentiate this false positive by showing acute mucosal involvement that could potentially be resolved through only antibiotics.[Reference Barrat, Catheline, Rizk and Champault141]
In just these instances alone, every year’s delay in advancing MIS translated to several hundred thousand patients undergoing the pain and risk of open surgery for what would turn out to be only a mild or even nonexistent pathology.
Such scenes were not the exclusive domain of gynecology. These same harrowing results crisscrossed the landscape of all disciplines, where even higher mortality rates and more invasive techniques prevailed. The gridiron incision, a crisscross of two 10- to 14-inch incisions – the horizontal one, hip bone to hip bone, followed by a similarly aggressive vertical incision – was standard procedure for many general surgeries of the upper abdomen. Surgeries for tumors embedded inside the jaw were even more extreme; the jaw had to be broken, with 4 to 5 teeth extracted. The incision was made either across the throat, from ear to ear, or from the top of the ear, running clear down to the bottom of the neck. It was only after all that skin and tissue had been peeled back with those same metal retractors that the tumor could finally be accessed. Not only were patients left with disfiguring facial scarring, but in as many as 30% of the more severe cases, patients would end up losing their ability to swallow, requiring them to eat through a feeding tube for the rest of their lives.
In other words, all around the world, in all surgical disciplines, shock-inducing incisions were chasing after what sometimes turned out to be the mildest of maladies.[16,Reference Nezhat19,Reference Nezhat77]
Relieved of Any Meaningful Culpability
The combination of these effects left millions of patients each year in tremendous postoperative pain, with 2–3 weeks in the hospital, including time in the ICU, considered as normal outcomes: so normal, in fact, that the medical literature prior to MIS rarely mentioned these events as complications at all, demonstrating that they had come to be viewed as unavoidable and, therefore, acceptable aftermaths. If one had only the medical literature of the pre-minimally invasive era as a gauge, it would seem as if all was right in the world of surgery, so thoroughly legitimized as scientific truths had these assumptions become (Figure 1.21).
This, an acceptable outcome?

If deaths did occur, laparotomy had become so beyond reproach that such outcomes were invariably attributed to other causes, such as anesthesia-induced effects or the patient’s advanced age, with the age of 60 often counted as “advanced.” Relieved from any meaningful culpability, “death by laparotomy” was rarely suggested as a cause of catastrophic outcomes, as it would have held little explanatory power.
In short, with open surgery reigning as an unchallenged authority over human lives for so long, catastrophic outcomes remained unrecognized as such. It was only after overwhelming evidence in favor of MIS accreted to a point where it became impossible to ignore, especially by patients themselves, that large incision surgeries were finally subjected to more rigorous critical analysis. This seismic shift in surgical standards took nearly 30 years to unfold and ultimately led to the worldwide downfall of open surgery as the former gold standard of surgery (Figure 1.22).
The transition from open surgery to MIS propelled by video surgery with and without robotic assistance.
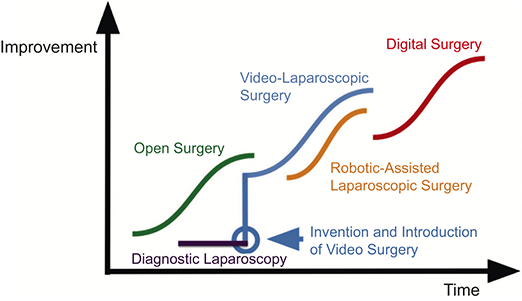
Figure 1.22 Long description
The x-axis represented as Time, y-axis represented as Improvement. It shows the progression from Open Surgery (gradual improvement), to Diagnostic Laparoscopy (an initial step), then Video-Laparoscopic Surgery, followed by Robotic-Assisted Laparoscopic Surgery, and finally Digital Surgery (showing rapid improvement). Each curve represents the typical adoption and maturation cycle of a disruptive technology in surgery.
Moving Ahead: The Future of MIS
Robotic surgery, also known as computer-enhanced telesurgery, has played a crucial role in the increased adoption of video laparoscopy. Urologists have utilized the enhanced degrees of freedom offered by robotic systems to navigate the male pelvis adeptly and suture structures that were previously challenging or even impossible. Gynecologists have widely embraced video laparoscopy, both with and without robotic assistance, for various conditions, including the management of endometrial, cervical, ovarian, and fallopian tube cancers. These advancements have significantly improved patient outcomes, with similar positive results observed in urology, gastroenterology, thoracic surgery, and more.
The development and application of new technologies, such as fluorescence-guided surgery (FGS), using indocyanine green (ICG), have taken a step further in minimizing the invasiveness of complex procedures by enhancing safety and accuracy while also providing overall cost-effectiveness procedures like pelvic and para-aortic lymphadenectomy or sentinel node biopsy have become less complicated, leading to reduced morbidity. Additionally, encouraging results in the use of neoadjuvant chemotherapy for advanced ovarian cancer have made the role of MIS more practical.
The harnessing of artificial intelligence, neural networks, and even social media networks can also be applied to patient advocacy and improving access to timely and accurate diagnoses. For example, Dr. Camran Nezhat has made significant contributions in democratizing access to medicine, especially in the context of endometriosis. Through his advocacy work, such as the EndoMarch initiative, Nezhat has raised awareness internationally about this often-overlooked condition, allowing for enhanced medical care worldwide. Nezhat has proved a pivotal role in increasing the early diagnosis rates of endometriosis through tirelessly promoting better understanding and more effective treatment methods. Additionally, the creation of Dr. Nezhat’s app “Nezhat Endometriosis Advisor” is a testament to his commitment in democratizing medical care. This app utilizes free and widespread technology to provide valuable information about endometriosis and the treatment options, serving as a critical tool in patient advocacy.
Now, the focus turns to training and educating future surgeons to become proficient in MIS techniques, ensuring standardized surgical procedures. Enabling devices, like robotic arms, have made minimally invasive technology more accessible and easier to learn.
The vision is for surgery to be customizable, replicable, and democratized. While medical treatments are standardized globally, surgery lacks this uniformity. Standardizing surgery becomes crucial for ensuring comparable metrics. Out of 8 billion people worldwide, 5 billion lack access to proper surgical care. An estimated 143 million more operative procedures are needed annually, and 19 million deaths can be avoided if proper surgery is performed. Studies indicate that less experienced surgeons have higher complication rates and increased operative times compared to high-volume surgeons.
The question arises: How can surgery be standardized and, consequently, democratized? Future techniques from the best surgeons in each field will combine to create standardized procedures for different pathologies, ensuring the highest quality of care is available to all. This involves making better use of surgical technologies, including digital surgery and subsequent developments.
Digital surgery, a fusion of robotics, data analytics, machine learning, artificial intelligence, neural networks, enhanced visualization, and enhanced instrumentation, is the path forward. Predictions suggest that intelligent robots will surpass human surgeons’ capabilities through self-learning and scaling. Various technologies, like image-guided ultrasound therapy, prosthetic limbs, 3D printing, artificial vessels, genome editing, fluorescence-guided surgery, and augmented reality, offer near-limitless possibilities, leading to incision-less surgical procedures.
The pace of advancement is accelerating, with improvements in energy modalities and noninvasive procedures replacing traditional surgeries. Technologies like high-intensity focused ultrasound (HIFU) and genome surgery with CRISPR/Cas9 are already changing the landscape.
The future direction involves combining digitized surgical methods with advances in imaging and energy generation to more accurately correct defective tissue and subcellular disease. The goal is visibility beyond the surface and distinguishing critical structures. The vision is for all surgical procedures for tissue removal or debulking to be incision-less. The belief is that this transformative future will arrive within the lifetimes of those reading this report, while the standardization, democratization, and expanded access to medicine and surgery will start with continued adoption and scaling of artificial intelligence and automation.
Final Reflections: Patient Advocacy Still Needed
We know such great transformations are possible, as we’ve seen in our lifetimes MIS transform from an impossible dream to the standard of care for nearly every major procedure. Just in gynecology alone, the proportion of hysterectomies performed video laparoscopically has significantly increased in recent years, up to 65.8% in 2018, compared to only 9.9% in 1997, with many performed in an outpatient setting.[Reference Deutsch, Zelikovsky and Reiss133,Reference DeArmond, Dent and Myers134] In contrast, abdominal open hysterectomies are falling out of favor, now accounting for only 28.3% of all hysterectomies.[Reference Morgan, Kamdar and Swenson143]
Despite this progress, the advocacy work to standardize, democratize, and expand access to MIS is not complete. Considering how much is at stake for the estimated 5 billion people who currently can’t access any form of surgery, it’s more urgent than ever to inspire this generation of medical professionals to expedite the harnessing of today’s technological advancements. This is essential for accelerating the standardization and democratization of surgical care, ultimately ensuring that improved health outcomes are accessible to all patients, regardless of economic or geographic demographics.
Though challenges remain, humankind is nevertheless now closer than ever to the ideal of performing the most advanced surgeries through the least traumatic incisions. For this reason, the introduction and adoption of MIS turned out to be one of the greatest achievements of twentieth-century medicine. More than that, it evolved into one of the world’s most important health rights movements, a change that transformed the lives of millions of patients who had suffered too long in the shadows of silence [Reference Lohman144] (Figure 1.23).
Nezhat and his fellows in the OR.

In a remarkable triumph that touched the hearts of countless people, Dr. Camran Nezhat achieved the pinnacle of recognition. Despite enduring the arrows of resistance and adversity throughout his tireless journey for almost 30 years, he was honored with the prestigious Distinguished Service Award by the American Medical Association (AMA) in November 2020 for his exceptional dedication to advancing the art and science of medicine and surgery. This inspiring achievement shines as a testament to the boundless potential of human innovation and resilience [16] (Figure 1.24).
Camran Nezhat was honored with the AMA’s Distinguished Service Award in recognition of his exceptional contributions to the science and art of medicine.