


Introduction
Childhood maltreatment (CM) is a common form of early life adversity that includes sexual, physical, and emotional abuse as well as physical and emotional neglect [Reference Cicchetti and Toth1]. It is highly prevalent, ranging from 15% in individuals with no psychiatric disorders to over 50% in psychiatric patients [Reference Struck, Krug, Yuksel, Stein, Schmitt and Meller2]. CM is a public health concern and a risk factor for psychiatric disorders, such as depression, schizophrenia, and externalized disorders [Reference Heleniak, Jenness, Stoep, McCauley and McLaughlin3–Reference Warrier, Kwong, Luo, Dalvie, Croft and Sallis5].
Alterations in grey matter volumes (GMV) in limbic and reward processing regions have been reported using cross-sectional magnetic resonance imaging (MRI) in healthy adolescents and adults reporting CM [Reference Cohen, Grieve, Hoth, Paul, Sweet and Tate6, Reference Edmiston, Wang, Mazure, Guiney, Sinha and Mayes7]. However, both lower and higher regional GMV were reported, notably in the amygdala and hippocampus [Reference Hakamata, Suzuki, Kobashikawa and Hori8–Reference Teicher and Samson13]. This heterogeneity could stem from variations in the age of the participants, the definition of CM used, the explored population (clinical or general), differences in psychiatric diagnoses, and whether the analysis focused on specific brain regions or investigated the whole brain. For instance, community-based adult studies using whole-brain analyses have described GMV alterations in regions from the extended limbic system, such as the insula, anterior cingulate cortex (ACC), and prefrontal cortex (PFC) [Reference Ansell, Rando, Tuit, Guarnaccia and Sinha14].
In addition, whether these anatomical changes affect the brain reward system function remains to be explored. Functional magnetic resonance (fMRI) studies reported lower reward sensitivity in individuals reporting early-life adversity [Reference Herzberg and Gunnar15–Reference Novick, Levandowski, Laumann, Philip, Price and Tyrka17]. However, most studies focus on reward response in the context of substance use disorders, and studies in general-population adolescents are scarce. Only one report on reward response and CM in healthy adolescents [Reference Hanson, Hariri and Williamson18] focused on emotional neglect, ignoring whether altered functional reward response could overlap in other types of maltreatment, such as sexual and emotional abuse, and physical abuse and neglect.
Cross-sectional studies, by design, do not allow for the investigation of whether the GMV changes in individuals reporting CM persist over time. Longitudinal neuroimaging studies in CM and limbic GMV in the general population are scarce. In young adults between ages 25 and 33, a stable effect of life adversity on the GMV of limbic regions has been reported, with increased and decreased volume changes depending on the type of adversity [Reference Holz, Zabihi, Kia, Monninger, Aggensteiner and Siehl19].
A longitudinal study reported amygdala developmental delays linked to CM and early adversities [Reference Whittle, Dennison, Vijayakumar, Simmons, Yücel and Lubman20], whereas another study reported an increase in amygdala GMV in neglected females [Reference Rakesh, Elzeiny, Vijayakumar and Whittle21]. However, these longitudinal studies focused on hippocampal and amygdala GMV changes, without assessing other limbic and reward system structures [Reference Whittle, Dennison, Vijayakumar, Simmons, Yücel and Lubman20, Reference Rakesh, Elzeiny, Vijayakumar and Whittle21]. Thus, additional longitudinal studies with a larger adolescent sample and investigating an extended set of limbic regions are needed to provide further insight into the associations between CM and limbic GMV.
The overarching aim of the present study was to investigate both the cross-sectional and longitudinal associations between CM and the structure and function of the extended limbic system in a large sample of community adolescents. This study addresses the following questions: (1) is CM associated with structural alterations in the extended limbic system? (2) is CM associated with altered functional response during reward processing? (3) Are these alterations persistent over time?
Thus, we compared GMV and task-based functional activation within the extended limbic system between adolescents with and without CM at ages 14 and 18. Additionally, in this longitudinal study, we conducted a repeated-measure analysis to investigate whether these potential differences associated with CM were stable between ages 14 and 18.
Methods
Available dataset
Neuroimaging and psycho-behavioural data from the IMAGEN consortium (https://imagen-project.org), a database including N = 2257 community adolescents from eight European sites recruited at age 14 with a follow-up at age 18, were used. A detailed description of recruitment and assessment procedures and exclusion and inclusion criteria has been published elsewhere [Reference Schumann, Loth, Banaschewski, Barbot, Barker and Büchel22]. IMAGEN data are available from a dedicated database: https://imagen2.cea.fr.
Participant selection
Participant groups were defined based on the CTQ scores, which N = 1359 participants had completed at age 18 (Figure S1, Supplementary Materials). A categorical approach based on validated thresholds for the five subscales was used [Reference Bernstein, Stein, Newcomb, Walker, Pogge and Ahluvalia23]. Two groups were defined: participants were included in the maltreated group (CM+) if at least one of the five subscale scores indicated moderate to extreme levels of CM (N = 167), and participants were included in the non-maltreated group (CM-) if they had scores corresponding to none or minimal CM on all subscales (N = 790). Subjects presenting intermediate scores of CM were excluded (N = 402).
After preprocessing and quality control of structural neuroimaging data (described below) at ages 14 and 18, N = 634 participants were included in the GMV analyses and divided into a group of N = 529 CM- and a group of N = 105 CM+ adolescents.
From these participants, and after preprocessing and quality control of the task-based fMRI data (described below), N = 559 participants were included at age 14 (N = 471 CM, N = 88 CM+), and N = 357 were included at age 18 (N = 296 CM-, N = 61 CM+) for functional MRI analyses.
Assessment of childhood maltreatment, psychological characteristics, and puberty
Participants completed the Childhood Trauma Questionnaire short form (CTQ-SF; [Reference Bernstein, Stein, Newcomb, Walker, Pogge and Ahluvalia23] at age 18. The IMAGEN dataset includes the Strengths and Difficulties Questionnaire (SDQ) [Reference Goodman24] and the Development and Well-Being Assessment (DAWBA) [Reference Goodman, Ford, Richards, Gatward and Meltzer25]. Participants completed both SDQ and DAWBA at ages 14 and 18 (Supplementary Materials). Pubertal measures were based on self-report for feasibility reasons in a large sample and to minimize intrusion at age 14, with a computerized version of the Puberty Development Scale (PDS) on Psytools platform for online self-assessment (Delosis, London). The PDS scale has been validated for adolescent populations [Reference Petersen26].
Ethical considerations
Local ethics research committees approved the IMAGEN study. Participants’ parents provided informed written consent, while written assent was obtained from the adolescents at age 14 and eventually signed written informed consent when over 18 years old (for more details, see Supplementary Materials).
MRI T1 and fMRI data acquisition
MRI scans were acquired at eight IMAGEN assessment sites with 3-Tesla scanners from various manufacturers (Siemens, Philips, General Electric, and Bruker) at ages 14 and 18. Imaging protocol comparability between the different scanners was ensured through optimal standardization. More information about quality control can be found elsewhere [Reference Schumann, Loth, Banaschewski, Barbot, Barker and Büchel22].
Neuroimaging measures of interest included voxel-based morphometry (voxel-wise GMV) and task-based functional activation during reward anticipation and feedback.
The acquisition and sequence parameters of the high-resolution T1-weighted three-dimensional structural images are detailed elsewhere [Reference Schumann, Loth, Banaschewski, Barbot, Barker and Büchel22].
A modified version of the well-established monetary incentive delay task (MID task), probing functional correlates of reward anticipation and feedback, was used with an fMRI event-related design [Reference Cao, Bennett, Orr, Icke, Banaschewski and Barker27, Reference Knutson, Westdorp, Kaiser and Hommer28] (see Supplementary Materials).
MRI and fMRI data pre-processing
For all structural scans, spatial normalization onto the MNI template (Montreal Neurological Institute) and tissue segmentation in grey matter probability maps were performed using the CAT12 toolbox (CAT12.8.2) [Reference Gaser, Dahnke, Thompson, Kurth and Luders29] of Standard Statistical Parametric Mapping (SPM12, http://www.fil.ion.ucl.ac.uk/spm, Wellcome Trust Centre for Human Neuroimaging, University College London, UK) implemented in Matlab (https://fr.math-works.com/help/matlab/ref/edit.html). Automatic and visual quality control procedures for pre-processed structural and functional MRI were implemented (see Supplementary Materials).
Statistical analyses
Demographic and psychological characteristics
Descriptive analyses were conducted using JMP PRO 17.0.0. Student’s t-tests were carried out to evaluate differences in age, CTQ scores, total intracranial volume (TIV), and SDQ scores between CM+ and CM – participants. Pearson chi-squared tests were used to assess differences in sex and depression and PTSD diagnoses. Analyses were conducted at 14 and 18.
3D T1-weighted image analyses using voxel-based morphometry (VBM)
Structural MRI analyses were conducted using CAT12 (SPM) with a hypothesis-driven approach within a GM mask based on previous findings in the extended limbic system [Reference Haber and Knutson30, Reference Stringaris, Vidal-Ribas Belil, Artiges, Lemaitre, Gollier-Briant and Wolke31], assembled with the Wake Forest University (WFU) PickAtlas [Reference Maldjian, Laurienti, Kraft and Burdette32] (see Supplementary Materials).
Voxel-wise analyses of GMV were conducted separately within the general linear model (GLM) framework for participants at ages 14 and 18. Between-group comparisons (CM- > CM+, CM- < CM+ contrasts) were investigated using the full factorial model for cross-sectional data in CAT12, with pubertal status, age, sex, scanning site, and TIV as confounding variables.
Lastly, longitudinal differences in GMV between age 14 and age 18 groups were investigated by performing a repeated-measure analysis with the “flexible factorial model” for longitudinal data in CAT12. We examined Time (age 14; age 18) × Group (CM+; CM-) interaction contrasts to test for between-group longitudinal differences.
Significant differences were identified using a height threshold set at p < 0.001 uncorrected and an extent threshold set at p < 0.05 family-wise error (FWE) corrected (k > 500 voxels). The height threshold p < 0.001 uncorrected was used to get a more complete report, while still controlling for multiple comparisons at the cluster level (Lieberman & Cunningham, 2009) [Reference Lieberman and Cunningham33].
Functional MRI data analyses
Functional MRI analyses were conducted using SPM12.
For each trial (e.g. reward feedback for a large win), pre-processed functional data were convolved using the SPM default haemodynamic response function (HRF). Movement parameters (three translations, three rotations) estimated during preprocessing were used as confounding variables.
All analyses were conducted within the grey matter reward system mask described above. Both reward anticipation and feedback were conditions of interest. As reward magnitude is known to induce brain activation in reward-related brain regions, we focused on the large reward, as was done in previous studies [Reference Cao, Bennett, Orr, Icke, Banaschewski and Barker27, Reference Schneider, Peters, Bromberg, Brassen, Miedl and Banaschewski34]. Thus, contrasts of interest included anticipation of large win versus no win, and feedback of a large win versus no win.
A full factorial design, identical to the one described above in the structural analysis, was used to investigate functional activation between CM groups.
For both structural and functional analyses, the SPM extension AAL3 [Reference Rolls, Huang, Lin, Feng and Joliot35] and the XJView SPM Toolbox (http://www.alive-learn.net/xjview) were used to label significant clusters. For all comparisons, brain locations were reported in terms of Montreal Neurological Institute (MNI) coordinates. The XJView SPM Toolbox was also used to create the figures.
Results
Sample characteristics
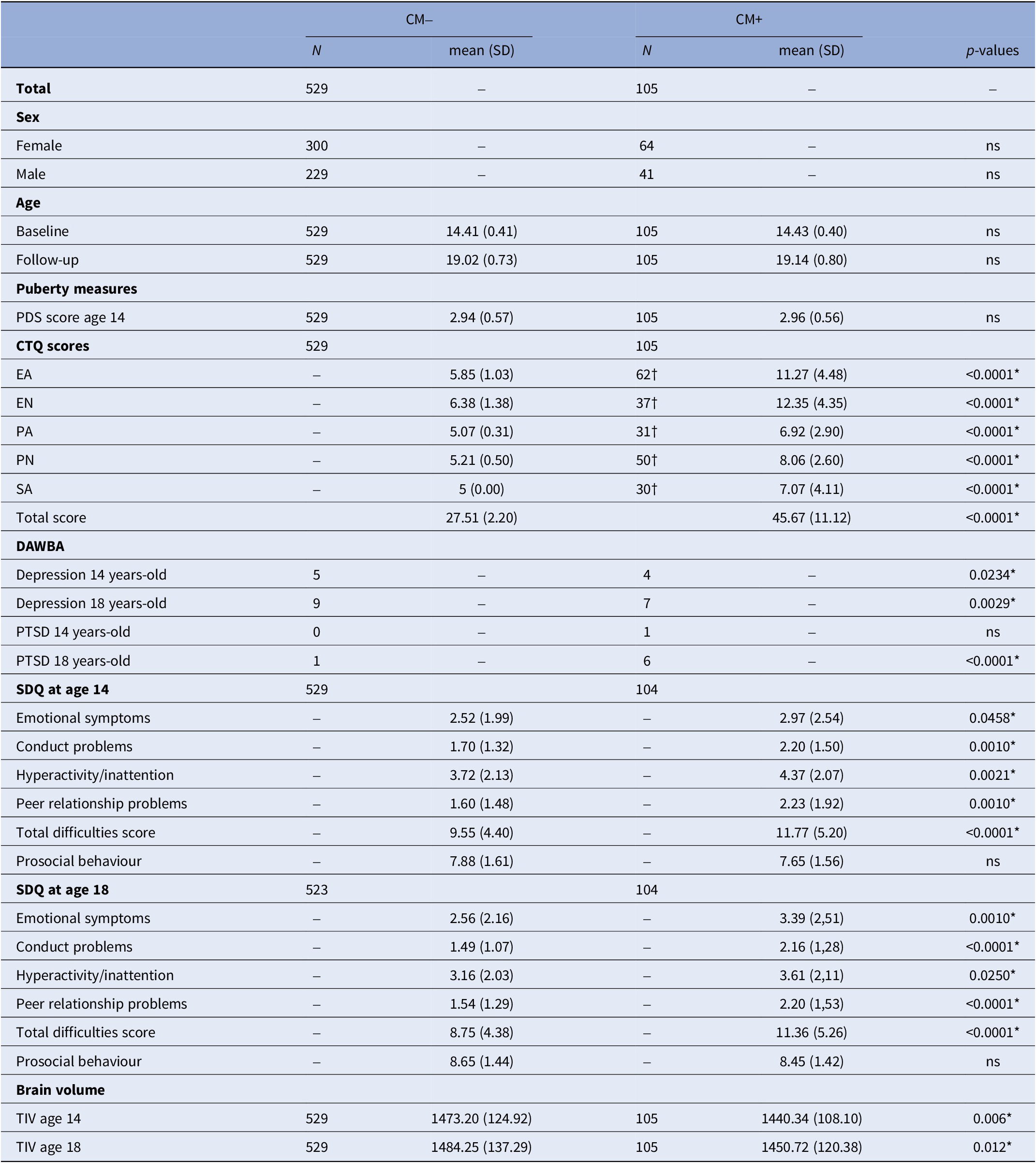
Sample characteristics and statistics are reported in Table 1. There were no significant differences in sex, age, and pubertal score between CM groups (Table 1). The CM+ group had significantly higher scores in all CTQ scores compared to the CM− group. No significant differences in sex distribution or age were detected between CM+ and CM−. The SDQ scales were significantly higher in the CM+ group, except for prosocial behaviour, which did not differ between CM groups. The CM+ group included a larger proportion of depressed participants at 14 and 18, and of participants with PTSD at 18, in comparison with the CM− group. There were no differences between CM groups in the proportion of participants with PTSD at 14. Finally, the CM+ group had a lower TIV at 14 and 18.
Sample characteristics and childhood maltreatment scores in N = 634 community adolescents

Note: *significant results (p < 0.05); †number of participants scoring above the threshold to consider CM. Group differences were tested using T-tests for continuous variables and chi-squared tests for categorical variables.
Abbreviations: CM- = no childhood maltreatment, CM+ = presence of childhood maltreatment, CTQ = childhood trauma questionnaire; EA = emotional abuse, EN = emotional neglect, PA = physical abuse, PN = physical neglect, SA = sexual abuse; DAWBA = Development and Well-Being Assessment; PDS = Puberty Development Scale; SDQ = Strengths and Difficulties Questionnaire; TIV = total intracranial volume.
Voxel-based morphometry results
Cross-sectional analyses
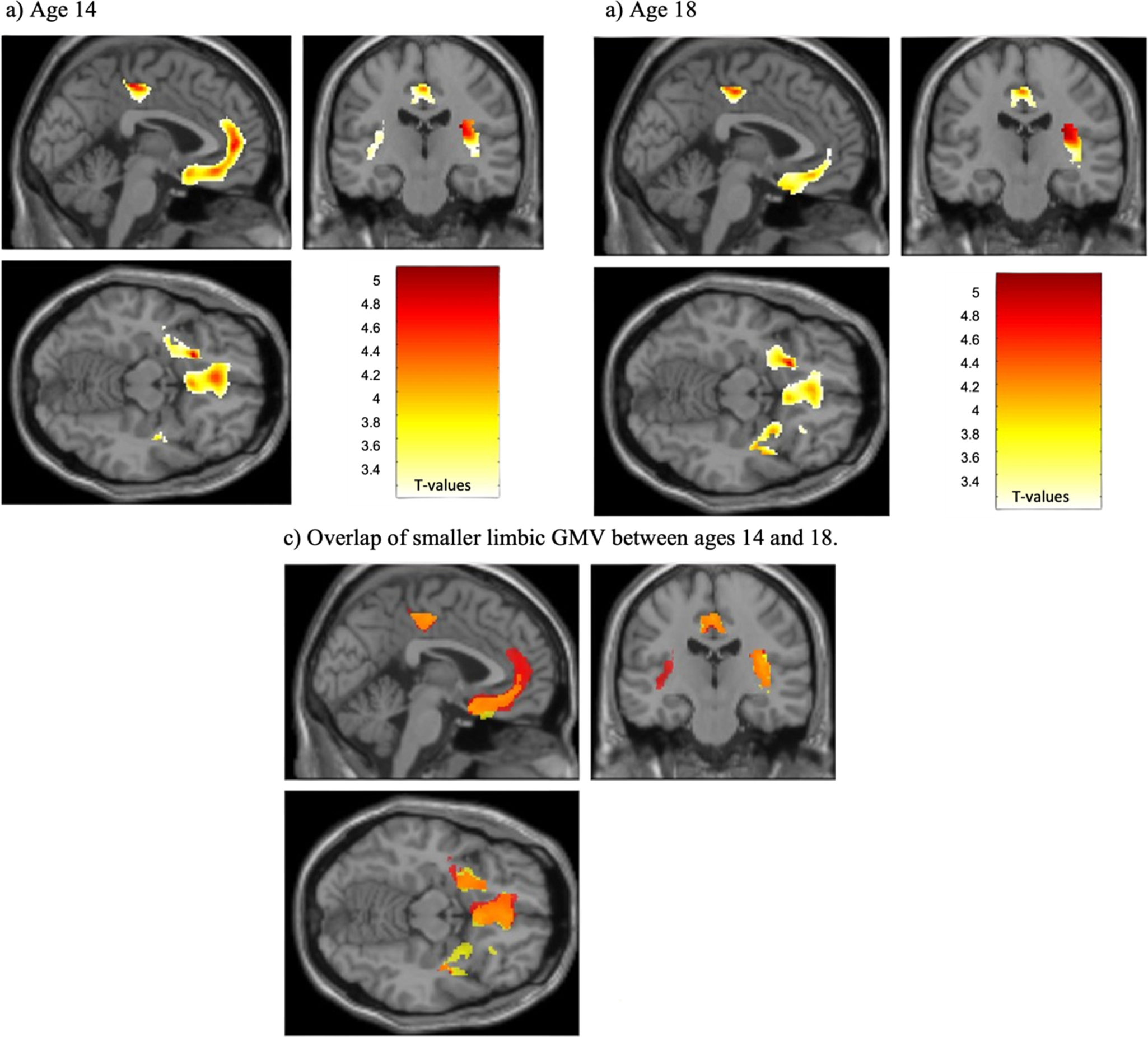
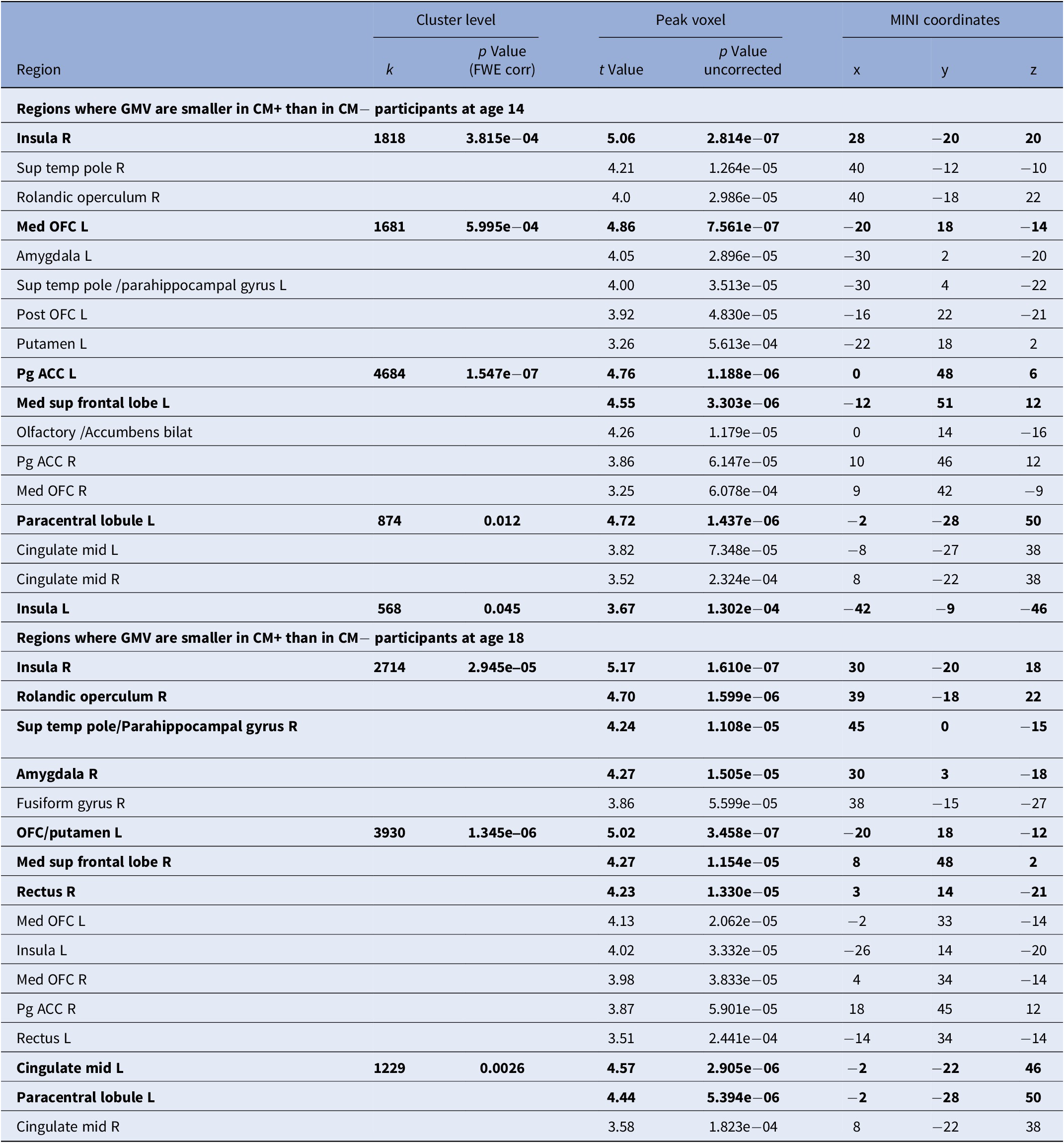
At age 14, a smaller GMV was found in the right posterior insula and left OFC, putamen, pregenual ACC, superior medial frontal cortex, subcallosal, inferior temporal lobe, and paracentral lobule in CM+ adolescents compared to CM− adolescents. We also report lower GMV in the left amygdala, medial OFC, parahippocampal gyrus, right rolandic operculum, pregenual ACC, OFC, bilateral middle cingulate, and superior temporal pole (Figure 1a and Table 2).
Smaller limbic grey matter volumes in CM+ versus CM- adolescents at ages 14 and 18. This figure shows the GMVs that are smaller in CM+ compared to CM- adolescents: a) at age 14, b) at age 18, and c) the overlap (orange) at ages 14 (red) and 18 (yellow). The height threshold is set at p < 0.001 uncorrected and the extent threshold is set at p < 0.05 Family-Wise Error (FWE) corrected (k > 500 voxels). CM+ = self-report of childhood maltreatment; CM- = no childhood maltreatment; GMVs = grey matter volumes.

Comparison of grey matter volumes in reward-related regions between CM+ and CM- adolescents at ages 14 and 18 (N = 634)

Note: Height threshold at p < 0.001 uncorrected. p values in bold are statistically significant at p < 0.05 Family-Wise Error (FWE) corrected; Extent threshold at p < 0.05 (FWE) corrected (k > 500 voxels).
Abbreviations: CM+ = self-report of childhood maltreatment; CM- = no childhood maltreatment; k = cluster size, expressed in number of voxels; MNI = Montreal Neurological Institute coordinates in millimeters; R = right; L = left; bilat = bilateral; med = medial; mid = middle; pg = pregenual; sup = superior; temp = temporal; GMV = grey matter volume; MNI: Montreal Neurological Institute (coordinates in mm).
At age 18, a smaller GMV was detected in the right insula and left OFC, right rolandic operculum, amygdala, superior medial frontal cortex, gyrus rectus, and left-sided middle cingulate and paracentral lobule. In addition, we report lower GMV in the right-sided temporal superior gyrus, fusiform gyrus, OFC, pregenual ACC, middle cingulate, and left rectus. No significantly larger GMV was detected in CM+ compared to CM− at ages 14 and 18 (Figure 1b and Table 2).
Longitudinal analysis
There were no significant Time (14; 18) × Group (CM+; CM−) interactions, denoting the stability of GMV within CM groups across time and showing a persistence of the smaller regional GMV in CM+ compared to CM−.
Functional results
No significant difference between CM+ and CM− adolescents was detected during the MID task for feedback or anticipation of large (vs. no) win at ages 14 or 18.
Discussion
Persistent grey matter volume (GMV) alterations were detected in a longitudinal sample of adolescents reporting childhood maltreatment (CM). Indeed, the repeated-measure analysis highlighted smaller GMV in the extended limbic system in adolescents with CM (CM+) compared to those reporting no CM (CM−) at ages 14 and 18 (regional overlap in Figure 1.c). In addition, CM+ adolescents reported higher levels of a possible diagnosis of depression at 14 and 18 and of PTSD at 18 than CM− adolescents. They also reported higher emotional symptoms, conduct problems, hyperactivity and inattention, peer relationship problems, and lower prosocial behaviour.
These findings align with abundant cross-sectional studies in children and youth reporting smaller TIV, insula, and amygdala GMV associated with CM [Reference Edmiston, Wang, Mazure, Guiney, Sinha and Mayes7, Reference Jeong, Durham, Moore, Dupont, McDowell and Cardenas-Iniguez36–Reference McLaughlin, Sheridan, Gold, Duys, Lambert and Peverill39]. These regions are involved in emotion awareness and regulation, fear and disgust processing, interoception, and self-recognition [Reference (Bud) Craig40, Reference Calder, Lawrence and Young41]. Surprisingly, we found no effect of CM on hippocampal GMV, although other authors have reported alterations in this region related to CM [Reference Hakamata, Suzuki, Kobashikawa and Hori8, Reference Paquola, Bennett and Lagopoulos10, Reference Pollok, Kaiser, Kraaijenvanger, Monninger, Brandeis and Banaschewski11]. However, smaller hippocampal GMV has mainly been described in PTSD [Reference Ahmed-Leitao, Spies, van den Heuvel and Seedat42, Reference De Brito, Viding, Sebastian, Kelly, Mechelli and Maris43] and adults with CM [Reference Hakamata, Suzuki, Kobashikawa and Hori8]. As our sample comprised general population adolescents rather than patients or adults, this could account for the absence of such alterations. Indeed, although our sample includes a few participants with PTSD (Table 1), their number is not substantial enough to observe an effect on hippocampal GMV. Furthermore, although SDQ scores indicated a poorer emotional and behavioral profile in the CM+ group, the mean scores remained within the normal range [Reference Goodman24], suggesting that while CM+ subjects exhibit a higher level of psychopathology, it may not be as severe as that observed in clinical samples. In addition, our results on hippocampal GMV align with other longitudinal studies involving community adolescents reporting CM [Reference Whittle, Dennison, Vijayakumar, Simmons, Yücel and Lubman20, Reference Rakesh, Elzeiny, Vijayakumar and Whittle21].
Beyond the results from previous longitudinal studies, we found a stable, smaller GMV in the medial cingulate cortex, left OFC, and left paracentral lobule. Smaller GMV in these regions has been reported in cross-sectional studies of adolescents and adults with CM [Reference De Brito, Viding, Sebastian, Kelly, Mechelli and Maris43–Reference Monteleone, Monteleone, Esposito, Prinster, Ruzzi and Canna45]. Nevertheless, it is the first time that longitudinal GMV alterations associated with CM can be reported in these regions.
In addition to the persistent alterations in limbic GMV associated with CM, the analyses at age 14 retrieved smaller GMV in the CM+ group compared to the CM− within the left pregenual ACC and inferior temporal gyrus. In the same line, analyses at age 18 detected smaller GMV in the operculum, gyrus rectus, and middle cingulate cortex. Cross-sectional studies have previously reported alterations associated with CM in these regions [Reference Monteleone, Monteleone, Esposito, Prinster, Ruzzi and Canna45–Reference Yang, Jin, Duan, Yu, Ping and Shen48] except for the gyrus rectus. Moreover, the longitudinal analysis showed no differences between age groups, suggesting that the same alterations were present at ages 14 and 18.
Surprisingly, the functional analysis of the reward system during the MID task did not retrieve significant differences in reward response between CM+ and CM− adolescents in the large-win vs no-win contrast, which taps into the sensitivity to reward. Still, the core regions activated by the MID task did not match those where smaller GMV was detected herein. In addition, in this sample with low psychopathology rates, GMV alterations associated with CM do not affect neuro-functional processing during the MID task. We cannot exclude that significant functional impairments only occur in adolescents with CM and marked psychopathology. For instance, reward sensitivity was assessed in a sample of depressed adolescents within the IMAGEN cohort, and OFC functional alterations were associated with depressive symptomatology [Reference Xie, Jia, Rolls, Robbins, Sahakian and Zhang49].
Overall, the aforementioned structural findings align with previous literature and add further evidence that limbic volumetric alterations associated with CM are enduring in adolescents. Indeed, cross-sectional GMV alterations have been consistently reported in children, adolescents, and adults [Reference Cohen, Grieve, Hoth, Paul, Sweet and Tate6–Reference Hakamata, Suzuki, Kobashikawa and Hori8, Reference Teicher, Samson, Anderson and Ohashi12, Reference Jeong, Durham, Moore, Dupont, McDowell and Cardenas-Iniguez36, Reference Yang, Jin, Duan, Yu, Ping and Shen48]. Even more so, most regions found altered in this study have been associated with depression [Reference McKay, Cannon, Chambers, Conroy, Coughlan and Dodd50, Reference Schmaal, Hibar, Sämann, Hall, Baune and Jahanshad51], anhedonia [Reference Zhu, Ward, Cullen, Lyall, Strawbridge and Lyall52], and PTSD [Reference Xiao, Yang, Su, Gong, Huang and Wang53]. Therefore, we hypothesize that these persistent brain alterations could underlie the well-established association between CM and severe psychiatric disorders. Consequently, the present findings insist on the need for research on targeted preventive interventions for adolescents who have experienced CM [Reference Teicher, Gordon and Nemeroff4, Reference Hardcastle, Bellis, Hughes and Sethi54, 55].
Strengths and limitations
This is the largest longitudinal study on GMV alterations in adolescents reporting CM to date. It includes general-population adolescents from eight sites across Europe, which improves generalizability and replicability but could also increase heterogeneity within the sample.
There are several limitations to this study. First, it is based on a declarative assessment of CM, which could be biased by the subjective memory of events. However, retrospective assessments were performed with commonly used and validated instruments to measure CM [Reference Gur, Moore, Rosen, Barzilay, Roalf and Calkins56]. In addition, CTQ scores are generally associated with an underestimation rather than an overestimation of CM. Selecting participants with scores above the threshold for a severe to extreme level of at least one type of CM may reduce bias by preventing the misclassification of maltreated individuals. Another limitation is that the CTQ is retrospective. Retrospective measures of CM were found to be less predictive of structural alterations than prospective measures [Reference Holz, Zabihi, Kia, Monninger, Aggensteiner and Siehl19, Reference Gehred, Knodt, Ambler, Bourassa, Danese and Elliott57]. In addition, due to the nature of the retrospective data, we could establish no causal effect of CM on GMV.
Second, the timing and duration of CM exposure could not be measured in this study. Brain developmental pace varies across different regions, highlighting the importance of CM timing in influencing developmental outcomes [Reference Brouwer, Klein, Grasby, Schnack, Jahanshad and Teeuw58, Reference Fox, Levitt and Nelson59]. Accordingly, the timing of CM exposure can shape both the alterations in GMV and the type of psychiatric disorder that emerges later on [Reference Kaplow and Widom60, Reference Luby, Barch, Whalen, Tillman and Belden61].
Third, this study could not determine whether the smaller GMVs associated with CM are present beyond the studied ages. However, another longitudinal study described persistent smaller GMVs associated with early adversity at ages 25 and 33, and replicated their results in a sample of individuals aged 22 [Reference Holz, Zabihi, Kia, Monninger, Aggensteiner and Siehl19]. This suggests that GMV alterations associated with early adversity persist into adulthood.
Lastly, this study could not distinguish between types of CM due to the CM+ sample size. Studies suggest that GMV alterations may vary depending on the specific types of CM reported. Consequently, not differentiating between these types could result in more heterogeneous samples and lower the statistical power of the analyses. Nonetheless, different types of CM often co-occur and can be challenging to disentangle [Reference Lim, Hart, Mehta, Worker, Simmons and Mirza62].
In conclusion, adding to prior reports in youth and adults, this study highlights a persistent smaller GMV in the extended limbic system in adolescents reporting childhood maltreatment. In the existing literature, structural alterations in these regions have been associated with vulnerability to affective disorders. Whether the present findings could be mitigated through psychological and pharmacological interventions remains at stake.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1192/j.eurpsy.2025.10111.
Financial support
This work received support from the following sources: the European Union–funded FP6 Integrated Project IMAGEN (Reinforcement-related behavior in normal brain function and psychopathology) (LSHM-CT − 2007-037286); the Eranet Neuron (Grant ANR-18-NEUR00002–01– ADORe); Agence Nationale de la Recherche (Grant ANR-12-SAMA-0004 -GeBra); Assistance-Publique Hôpitaux-de-Paris and INSERM (interface grant); Paris Descartes University (Grant collaborative-project-2010); Paris Sud University (Grant IDEX-2012); Fondation de l’Avenir (Grant AP-RM-17-013); Fondation de France (Grant 00081242); Fédération pour la Recherche sur le Cerveau, and Fondation pour la Recherche Médicale (Grants DPA20140629802 and ADOLIMIS DPP20151033945); the Ile-de-France Region (Action 16700103 -grant to QIM– VEAVE, n°23002745–23002747); the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London, and the Bundesministerium für Bildung und Forschung (BMBF grants 01GS08152; 01EV0711; Forschungsnetz AERIAL 01EE1406A, 01EE1406B; Forschungsnetz IMAC- Mind 01GL1745B); the Deutsche Forschungsgemeinschaft (DFG project numbers 186318919[FOR 1617], 178833530 [SFB 940], 386691645 [NE 1383/14–1], 4022170461 [TRR 265], 45425598 [IRTG 2773]); the Medical Research Foundation and Medical Research Council (grants MR/R00465X/1 and MR/S020306/1). The INSERM (PI: David Cohen); and Strasbourg University and SATT CONECTUS, provided sponsorship (PI: Jean-Luc Martinot).
Competing interests
TB served in an advisory or consultancy role for ADHS digital, Infectopharm, Lundbeck, Medice, Neurim Pharmaceuticals, Oberberg GmbH, Roche, and Takeda. He received conference support or speaker’s fee by Medice and Takeda. He has been involved in clinical trials conducted by Shire & Viforpharma. He received royalties from Hogrefe, Kohlhammer, CIP Medien, Oxford University Press. He has been involved in clinical trials conducted by Shire & Viforpharma. GB has received honoraria from General Electric Healthcare for teaching on scanner programming courses. LP served in an advisory or consultancy role for Roche and Viforpharm and received speaker’s fee by Shire. She received royalties from Hogrefe, Kohlhammer and Schattauer. The present work is unrelated to the above grants and relationships. The other authors report no conflicts of interest.



 Open access
Open access
Comments
No Comments have been published for this article.