


Iodine is an integral component of thyroid hormones, which are crucial for proper neurological development. The interval between conception and the first 2 years of life, known as the ‘first 1000 days’, has a fundamental influence on long-term child brain development(Reference Mattei and Pietrobelli1). The consequences of severe iodine deficiency during pregnancy are well known and include infant mortality, miscarriage and congenital iodine deficiency disorders(Reference Laurberg, Cerqueira and Ovesen2). Mild to moderate iodine deficiency can also have consequences for human health, especially during pregnancy, and observational studies have found it to be associated with learning disabilities and poorer verbal intelligence quotient scores in the offspring(Reference Levie, Korevaar and Bath3). The data on a possible association with autism are conflicting(Reference Levie, Bath and Guxens4).
Iodine is obtained almost exclusively from the diet. The daily iodine intake should be increased during gestation by up to 50 % compared with normal requirements. From mid-gestation onwards, the iodine pool is shared between the mother and the fetus, following development of the fetal thyroid and its consequent functional autonomy.
Therefore, it is very important to closely monitor iodine status during pregnancy and ensure an adequate daily iodine intake in order to reach the recommended requirement of 250 μg/d. According to the World Health Organization (WHO) guidelines, median urinary iodine values ≥ 150 ug/l constitute an adequate iodine intake for pregnant women(Reference Laurberg, Cerqueira and Ovesen2).
Knowing the current iodine status of pregnant women in the Veneto region of Italy would be of great value in programming iodine prophylaxis campaigns and would help clarify whether or not iodine supplementation should be recommended in this crucial period of a woman’s life. The last survey of iodine status in 322 pregnant women residing in the Veneto region was conducted in 2008, and it reported a median urinary iodine concentration (UIC) of 83 μg/l, far lower than the desirable range (150–249 μg/l)(Reference Mian, Vitaliano and Pozza5). A subsequent, but more limited study of ninety-two pregnant women based on data collected between 2016 and 2017 reported a UIC of about 56 μg/l(Reference Censi, Watutantrige-Fernando and Groccia6). Data collected from school-aged children (SACs) show that iodine sufficiency has recently been reached in Italy, including the Veneto region, thanks to a sustained iodine prophylaxis programme that has been running since 2005(Reference Olivieri, Andò and Bagnasco7).
However, since the iodine status of SACs may not necessarily reflect that of women of childbearing age or pregnant women, it was necessary to verify the progress in iodine sufficiency among pregnant women since the 2008 survey.
There are still no clear, consistent guidelines regarding the need for iodine supplementation in pregnancy. The American Thyroid Association recommends iodine supplementation during pregnancy, but the WHO does not consider it necessary for women living in countries running effective and sustained iodised salt programmes. An Italian consensus document does not recommend iodine supplementation and only advises gynaecologists to suggest using iodised salt and consuming iodine-rich foods(Reference Marangoni, Cetin and Verduci8). These differing recommendations reflect the differences in iodine status across regions, and, consequently, the variations in iodine-prophylaxis policies, which are adapted to the needs of specific areas. We therefore need to assess the situation in our region in order to adapt iodine-prophylaxis policies for pregnant women to the local context.
While mean urinary iodine concentration is a useful measure in populations, it is not useful in evaluating individual iodine status, which is highly variable and dependant on the individual’s very recent iodine intake(9). Thyroglobulin (Tg) may help to overcome this limitation. Tg has previously been found to be a valuable biomarker of iodine status during pregnancy in both iodine-sufficient and iodine-deficient areas(Reference Eltom, Elnagar and Elbagir10–Reference Stinca, Andersson and Weibel12). It seems to be especially useful in the second part of pregnancy, reflecting the long-term rather than recent iodine intake(Reference Censi, Watutantrige-Fernando and Groccia6). A previous randomised controlled trial on iodine supplementation in pregnancy carried out by our group confirmed the inverse relationship between higher iodine intake and lower Tg values during the second and third trimesters in women initiating iodine supplementation in the first trimester(Reference Censi, Watutantrige-Fernando and Groccia6). However, the value of Tg taken during pregnancy in predicting neonatal outcomes in relation to iodine status remains unclear.
Given the limitations of urinary iodine concentration for assessing individual iodine status, we investigated whether serum Tg could serve as a useful complementary biomarker in pregnancy to assess the need for iodine supplementation, if any, in order to avoid deficits and excesses of iodine intake, both of which are detrimental to fetal well-being.
Our primary goal was (i) to carry out an up-to-date assessment of the iodine status of pregnant women residing in the Veneto region. As secondary goals: (i) to identify the dietary and social factors that might influence iodine status; to investigate (ii) the possibility of Tg being a proxy for iodine status in pregnancy; (iii) the influence of iodine status on maternal thyroid function (TSH, FT4 and FT3) and on Tg values; (iv) the influence of the maternal iodine status on the offspring’s TSH at neonatal screening and (v) the influence of the maternal iodine status on the pregnancy and the newborn’s outcomes.
Patients and methods
We conducted a cross-sectional, observational study. A flow chart of the participants is depicted in online Supplementary Figure 1. Women were consecutively enrolled during their pre-delivery anaesthesiology pre-hospitalisation consultation from May 2020 to June 2022 (all eligible women who arrived during the study period were approached and included consecutively). We calculated the required sample size based on our primary outcome (evaluating iodine status among pregnant women residing in Veneto). Power was calculated separately for the logistic regressions and linear regressions, the main statistical analyses in the study. For the logistic regressions, assuming a weak effect size (odds ratio = 1·5) and an overall R2 of 30 % from all the other independent variables in the model, a sample size of 528 would provide 96 % power to detect a significant effect at an α level of 0·05. For the linear regressions, the number of initial independent variables varied across the models (ranging from 10 to 15). With a sample size of 528 participants, the statistical power ranged from 92 % (for models with fifteen independent variables) to 96 % (for models with ten independent variables) to detect a small effect size (f² = 0·05) at an α level of 0·05. Inclusion criteria were (i) resident in the Veneto region; (ii) in the third trimester of a singleton pregnancy; (iii) ≥ 18 years of age and (iv) freely given informed consent. Exclusion criteria were (i) having a known autoimmune or non-autoimmune thyroidal disease; (ii) on levothyroxine therapy and (iii) refusing informed consent. Upon enrolment, the subjects provided an early-morning spot urine sample to assay urinary iodine (UI) and creatinine concentrations (the UI/Creat ratio was used to measure iodine status), and a blood sample to measure TSH, FT4, FT3, and Tg. The day before the pre-delivery anaesthesiology pre-hospitalisation consultation, to which they were required to bring the early morning spot urine sample, and at which the blood sample was taken, we phoned the patients and explained the sample collection procedure (first morning urine, midstream). The women were also given a questionnaire (online Supplementary Figure 2) requesting the following information: personal details, age, anthropometric data, including height and pre-pregnancy weight, from which the pre-pregnancy BMI was calculated, gestational age (obtained from the questionnaire), lifestyle (smoking habits), geographical origin (categorised by country of birth as either ‘Italy’ or ‘abroad’, and further categorised by macro-region of origin as ‘Italy or Europe, excluding eastern Europe’, ‘eastern Europe’, ‘Africa’, ‘Asia’, ‘North or South America’), educational level, dietary habits (including use of iodised salt (IS) and consumption of cow’s milk), use of iodine-containing supplements (ICS) with the brand name (to obtain the quantitative iodine content, as reported in the manufacturer’s specifications), and the subject’s awareness of the iodine prophylaxis programme. The questionnaire was administered on the enrolment day, which coincided with the pre-delivery anaesthesiology pre-hospitalisation consultation and collection of the urine and blood samples. Participants completed the questionnaire with the guidance of a physician to verify data completeness and ensure each section was fully understood. Milk intake was scored as: 1 = never; 2 = a few times a week; 3 = one cup a day (at least 200 ml/d); and 4 = more than 1 cup a day. Cow’s milk consumption was also dichotomised as: 1 = regular (daily or more than once a day) or 0 = occasional (less than once a day). In light of the importance of milk, suggested by our previous reports on iodine sufficiency conducted in the Veneto region, we focused particular attention on this food category(Reference Censi, Manso and Barollo13). The consumption of other foods (i.e. yogurt, cheese, meat, eggs, fish, etc.) was scored as: 1 = never; 2 = at least once a week; 3 = more than once a week, and also dichotomised as regular if more than once a week, or irregular if once a week or less often). The questionnaire investigated the weekly frequency of intake, not the portion size. The newborns’ TSH levels were obtained in all cases from the congenital hypothyroidism screening programme, and were collected on the second or third day after birth, in accordance with Italian law (DM 13/10/2016). The following information on newborns was obtained from an electronic database: gestational age, sex, birth weight and height, and the presence of small-for-gestational age (SGA) (defined as a birth weight of less than the 10th percentile for gestational age). The following potential sources of bias were present: (i) women were asked to provide an early morning urine sample, but as they took it themselves at their homes we cannot be sure it was done correctly; (ii) language barrier: foreign women with an inadequate knowledge of Italian answered the questions with help from an interpreter (usually a relative) and the physician, but incomplete comprehension remains a possibility; (iii) the single spot urine sample may not reliably reflect the dietary habits reported in the questionnaire; (iv) information on the use of iodised salt may not be reliable, as some women may not be fully aware of the type of salt used in their households. The study was performed in accordance with the guidelines of the Helsinki Declaration and approved by the Local Ethical Committee (Padua General Hospital, Comitato Etico per la Sperimentazione Clinica (CESC), code number: 4603/AO/18). All patients gave their written informed consent.
Laboratory assays
The early-morning, non-fasting urine samples were divided into aliquots, and refrigerated at –20°C until assay. The blood samples were promptly aliquoted and stored at –20°C to preserve the integrity of the analytes. UIC was measured in duplicate using the colorimetric ceric ion-arsenious acid method in a second-generation Technicon Auto-Analyzer (Bran+Luebbe GmbH, Norderstedt, Germany)(Reference Garry, Lashley and Owen14). Between-run accuracy, assessed by repeatedly measuring two levels of an in-house quality control material (95 and 300 μg/l), was between 1·7 % and 2·8 %. At the start of each run, a standard curve was also verified with serial dilutions of a synthetic tester. Urinary creatinine was measured using the enzymatic method (Roche Cobas® 8000 Modular Analyzer; Roche, IN, USA) with a reference range of 0·1–54 mmol/l(Reference Busnardo, Nacamulli and Zambonin15). UI/Creat was measured as μg/g. Serum TSH, FT3, and FT4 levels were tested using commercial kits (Roche, Rotkreuz, Switzerland) with reference ranges, respectively, of 0·2–4 mIU/l, 3·90–6·80 pmol/l, and 9·00–22·00 pmol/l. Tg was measured by chemiluminescent immunoassay (CLIA; Beckman Coulter, USA), the normal range being 0–50 ng/ml. The analytical coefficients of variation used for the laboratory assays are provided in online Supplementary Table 2.
Statistical analysis
The Kolmogorov-Smirnov test was used to assess the normal distribution of each variable. As the quantitative variables were not normally distributed, they are reported as medians and interquartile range (IQR). The Mann–Whitney or Kruskal–Wallis tests were used, as appropriate, to explore the relationships between the quantitative and categorical variables. The χ² test was used to assess the associations between categorical variables. The performance of Tg was assessed through analysis of the receiver operating characteristic curve, from which the best statistical cut-off for iodine sufficiency (corresponding to a UI/Creat ≥ 150 μg/g) was identified; the sensitivity, specificity, positive predictive value, negative predictive value, and area under the curve (AUC) of the cut-off were then calculated. Correlations were analysed with Pearson’s or Spearman’s correlations after checking the data distribution. All analyses were performed using MedCalc and R (R Core Team 2023). The relationships between the independent variables of interest and the dependent variables was investigated by means of a series of multiple linear or logistic regression models. Further information on the statistical analyses are provided in the online Supplementary Materials.
Results
Primary goal: to provide an up-to-date assessment of the iodine status of pregnant women residing in the Veneto region
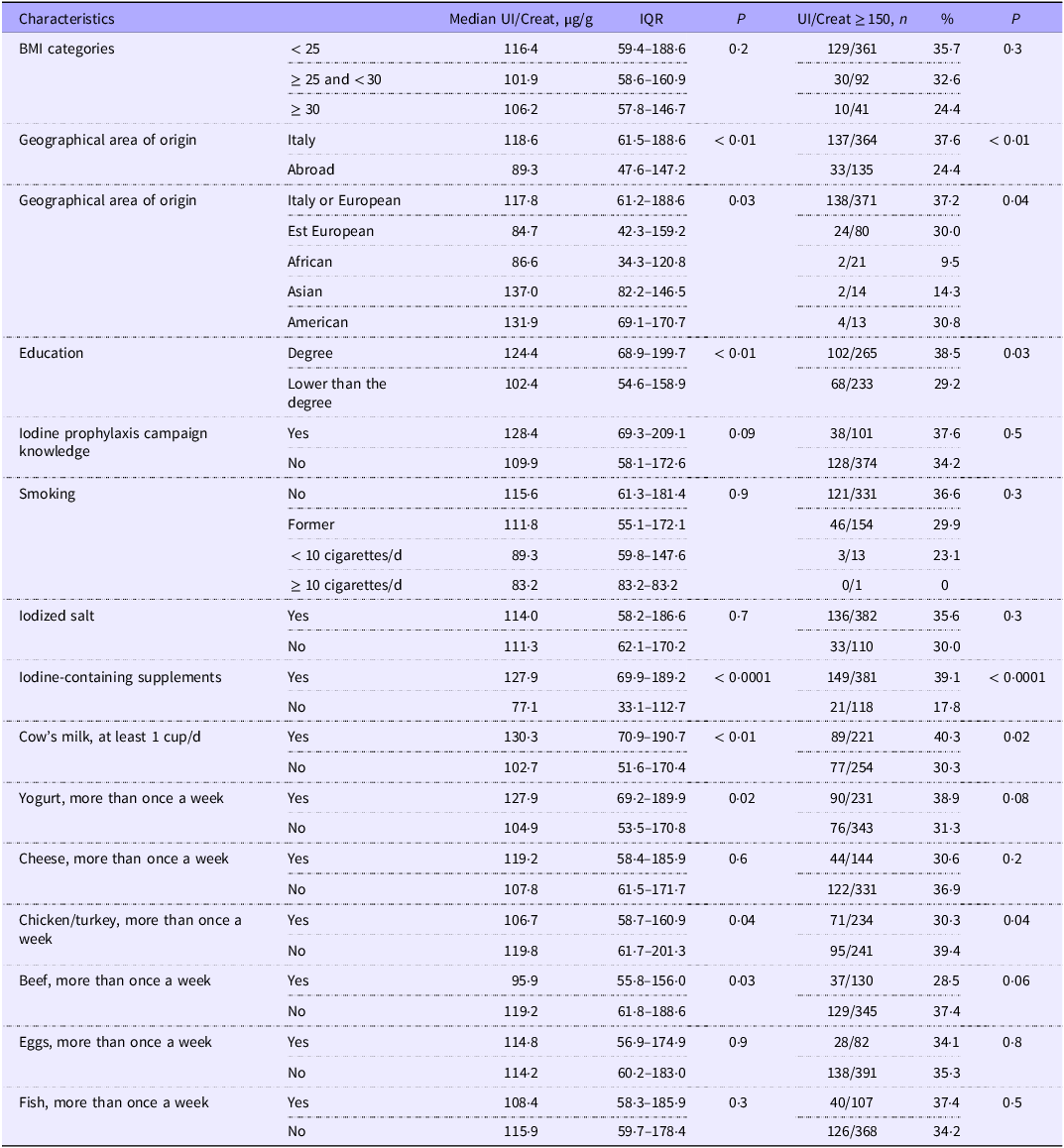
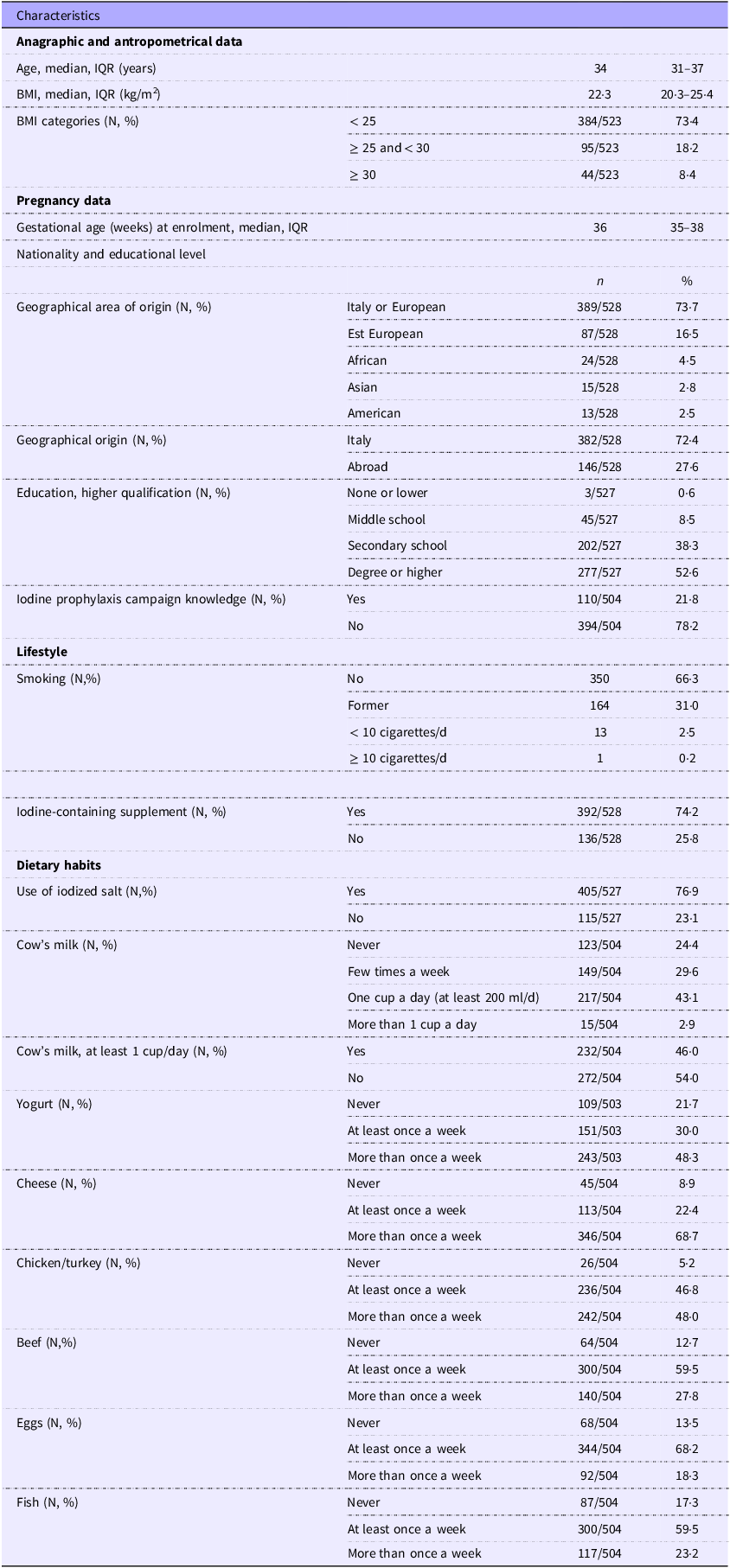
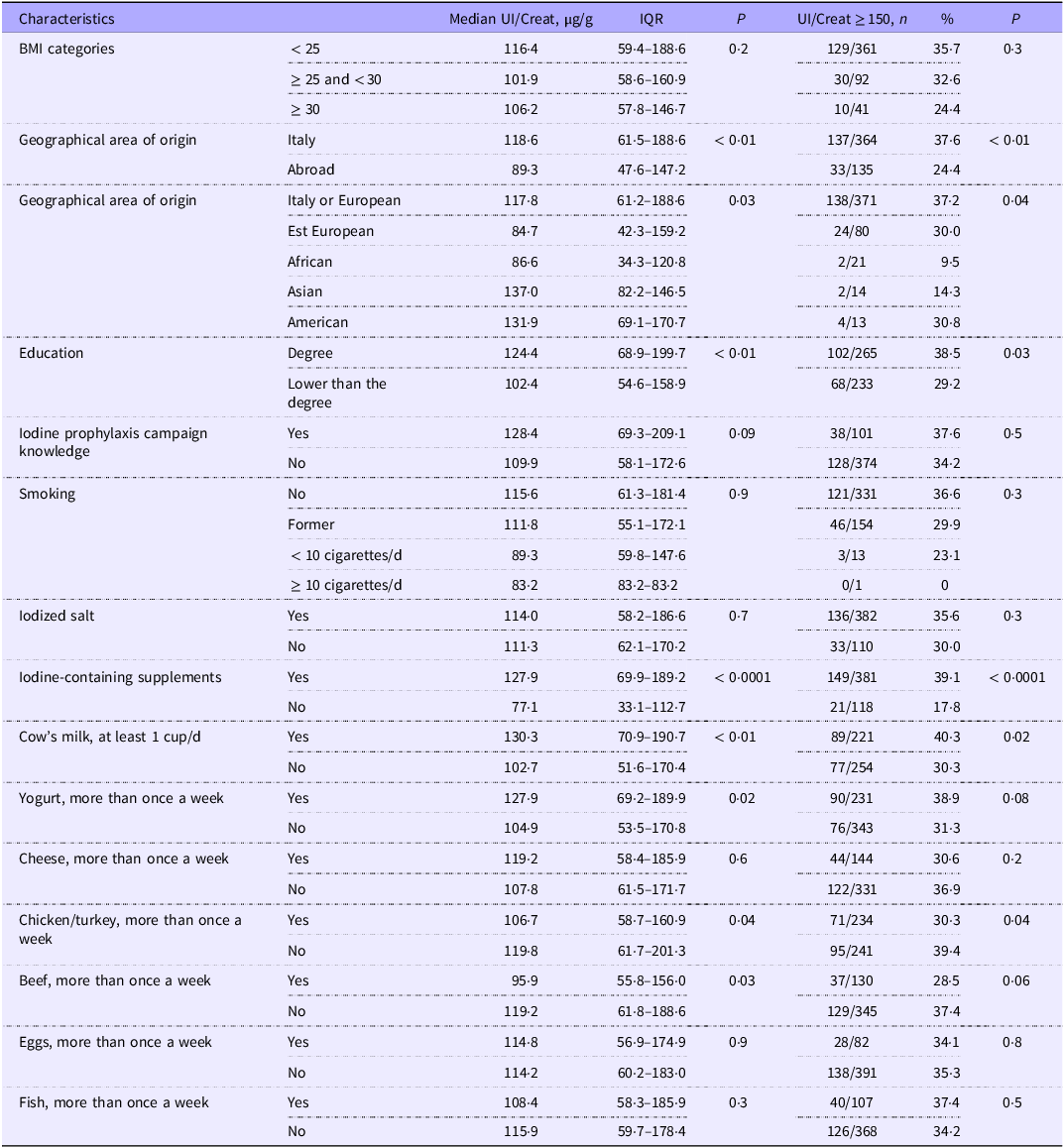
We consecutively enrolled 528 women with a median age of 34 years (IQR: 31–37 years) and at a median gestational age of 36 weeks (IQR: 35–38 weeks). The subjects’ characteristics are reported in Table 1. UI/Creat values were obtained for 499 subjects (the urine spot samples of twenty-nine subjects had deteriorated). Median UI/Creat was 112·8 μg/g (IQR: 58·9–176·7 μg/g), and only 170/499 subjects (34·1 %) had a UI/Creat ≥ 150 μg/g. In particular, UI/Creat was < 50 μg/g in 100/499 (20·0 %) subjects, ≥ 50 but < 150 μg/g in 229/499 (45·9 %), ≥ 150 μg/g but < 250 μg/g in 121/499 (24·3 %) and ≥ 250 μg/g in 49/499 (9·8 %). Only 110/504 (21·8 %) of the interviewed women were aware of the iodine prophylaxis campaign. Briefly, Italian women had higher UI/Creat levels than foreign women, the median values being 118·6 μg/g (IQR: 61·5–188·6 μg/g) and 89·3 μg/g (IQR: 47·6–147·2 μg/g), respectively (P < 0·01). Moreover, there was a greater frequency of UI/Creat ≥ 150 μg/g among Italian (37·6 %) than non-Italian women (24·4 %) (χ 2(1) = 7·6, P < 0·01). Highly educated women had a better iodine status than women with lower qualifications (median UI/Creat 124·4 μg/g [IQR: 68·9–199·7 μg/g] v. 102·4 μg/g [IQR: 54·6–158·9 μg/g], respectively [P < 0·01]) and also a higher frequency of UI/Creat ≥ 150 μg/g (38·5 % v. 29·2 %, respectively) (χ 2(1) = 4·8, P = 0·03). Further details are provided in Table 2.
Subjects’ characteristics
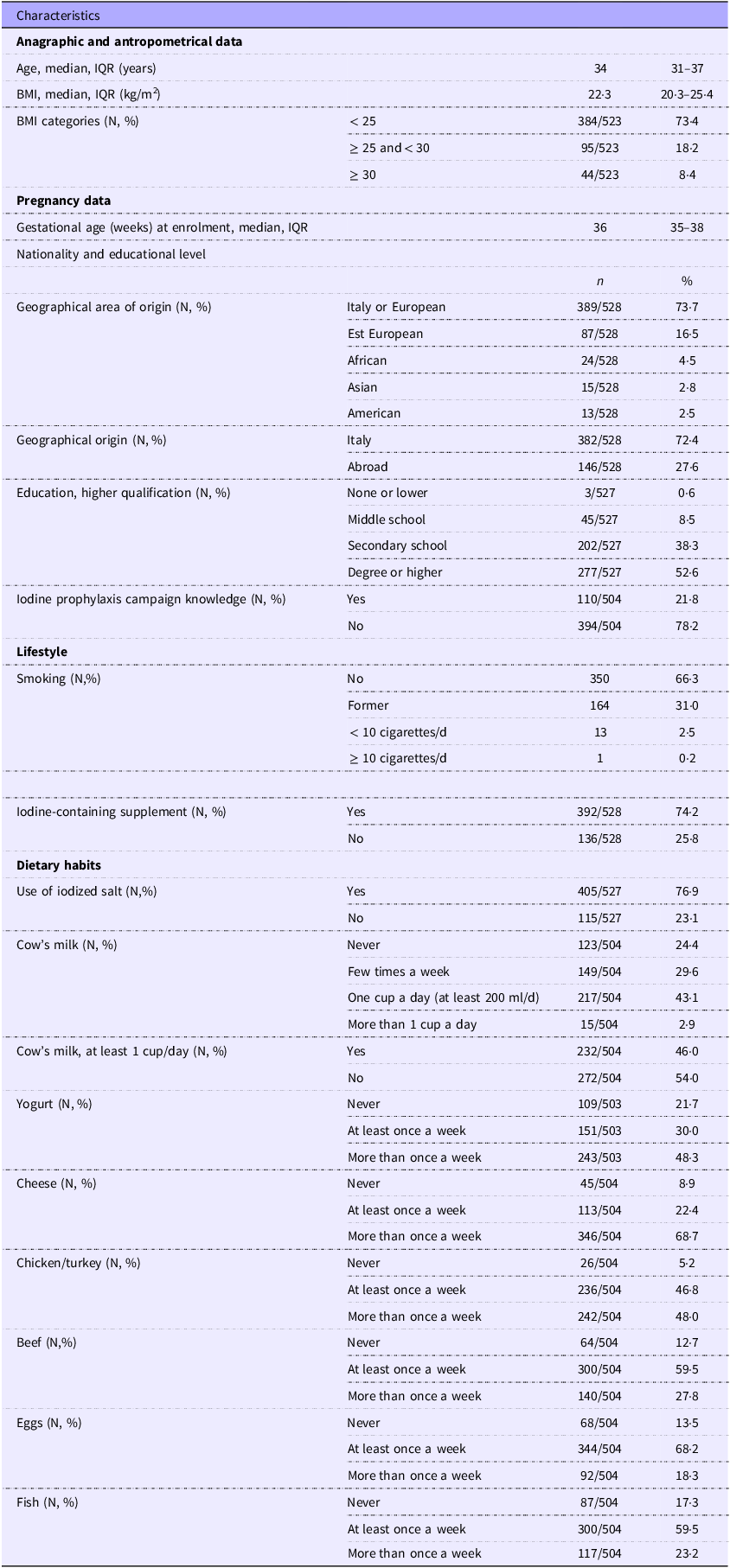
IQR, interquartile range.
Median UI/Creat and frequency of UI/Creat ≥ 150 μg/g according to social and dietetic factors
Secondary goal (i): to identify the dietary and social factors potentially influencing iodine status
Overall, 405/527 (76·9 %) women were using IS. We found no difference between the UI/Creat levels of users and non-users (see Table 2).
An ICS was being taken by 392/528 (74·2 %) of the women. The median iodine content of the iodine supplement was 175 μg (IQR: 175–220 μg). The women taking an ICS had a better iodine status (median UI/Creat 127·9 μg/g, IQR: 69·9–189·2 μg/g) than those who were not (median UI/Creat 77·1 μg/g, IQR: 33·1–112·7 μg/g) (P < 0·0001) and also more frequently had a UI/Creat ratio ≥ 150 μg/g (149/381, 39·1 % v. 21/118, 17·8 %) (χ 2(1) = 18·2, P < 0·0001) (Table 2).
Cow’s milk was regularly consumed (at least 1 cup/d) by 232/504 (46·0 %) by women. Regular consumers of cow’s milk had a better iodine status (median UI/Creat 130·3 μg/g, IQR: 70·9–190·7 μg/g) than non-consumers (102·7 μg/g, IQR: 51·6–170·4 μg/g) (P < 0·01) and also a higher frequency of UI/Creat ≥ 150 μg/g (89/221, 40·3 % v. 77/254, 30·3 %) (χ 2(1) = 5·1, P = 0·02) (Table 2). Data on other food categories and UI/Creat are reported in Table 2.
At logistic regression analysis, the only significant independent determinants for UI/Creat ≥ 150 μg/g were regular cow’s milk consumption (OR: 1·57, 95 % CI: 1·06, 2·32; P = 0·02) and use of an ICS (OR: 2·83, 95 % CI: 1·66, 4·82; P < 0·001). However, neither cow’s milk nor ICS alone seems to be enough to reach an adequate iodine status (online Supplementary Table 1).
Secondary goal (ii): to assess the possibility of Tg being a proxy for iodine status in pregnancy
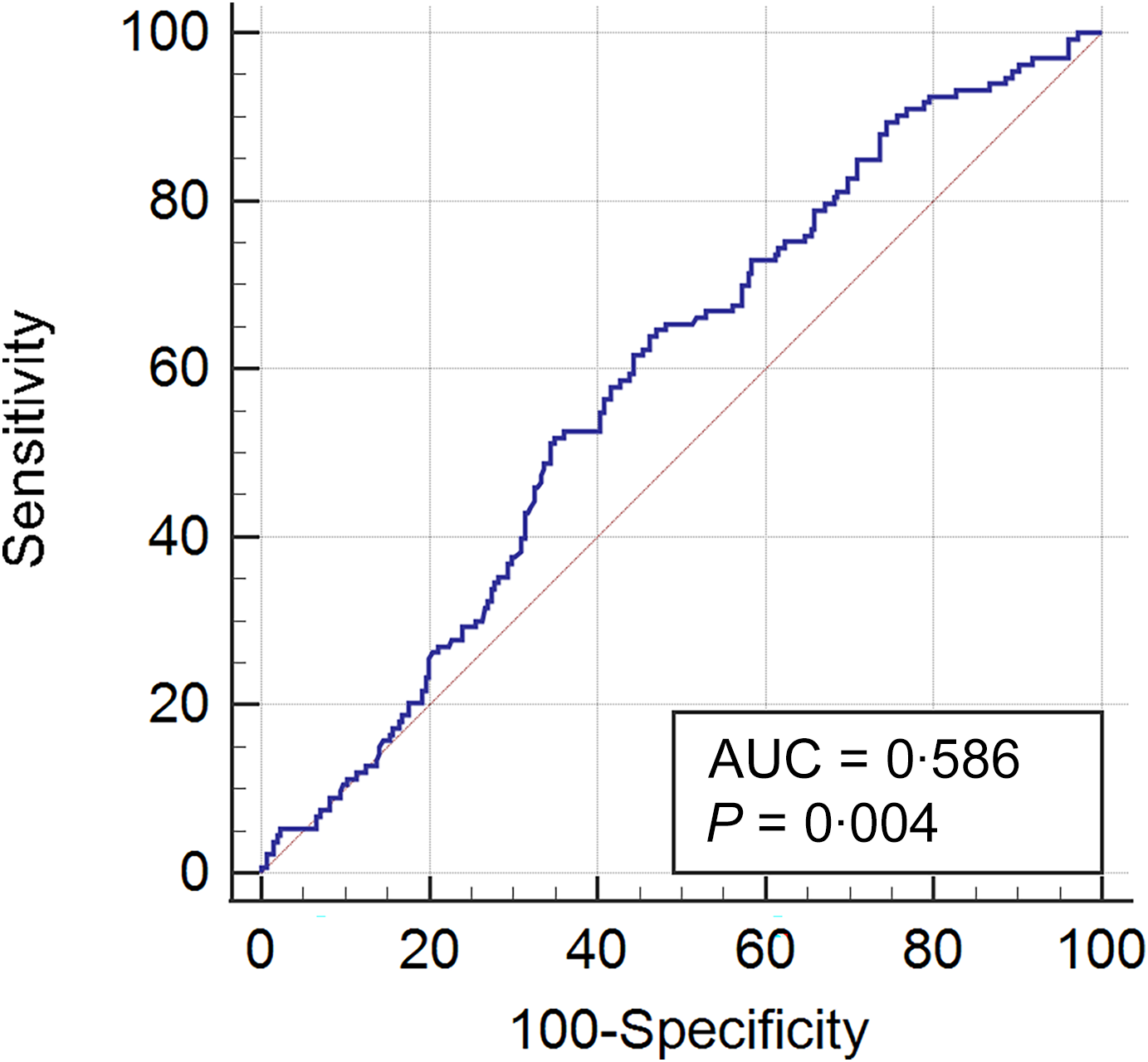
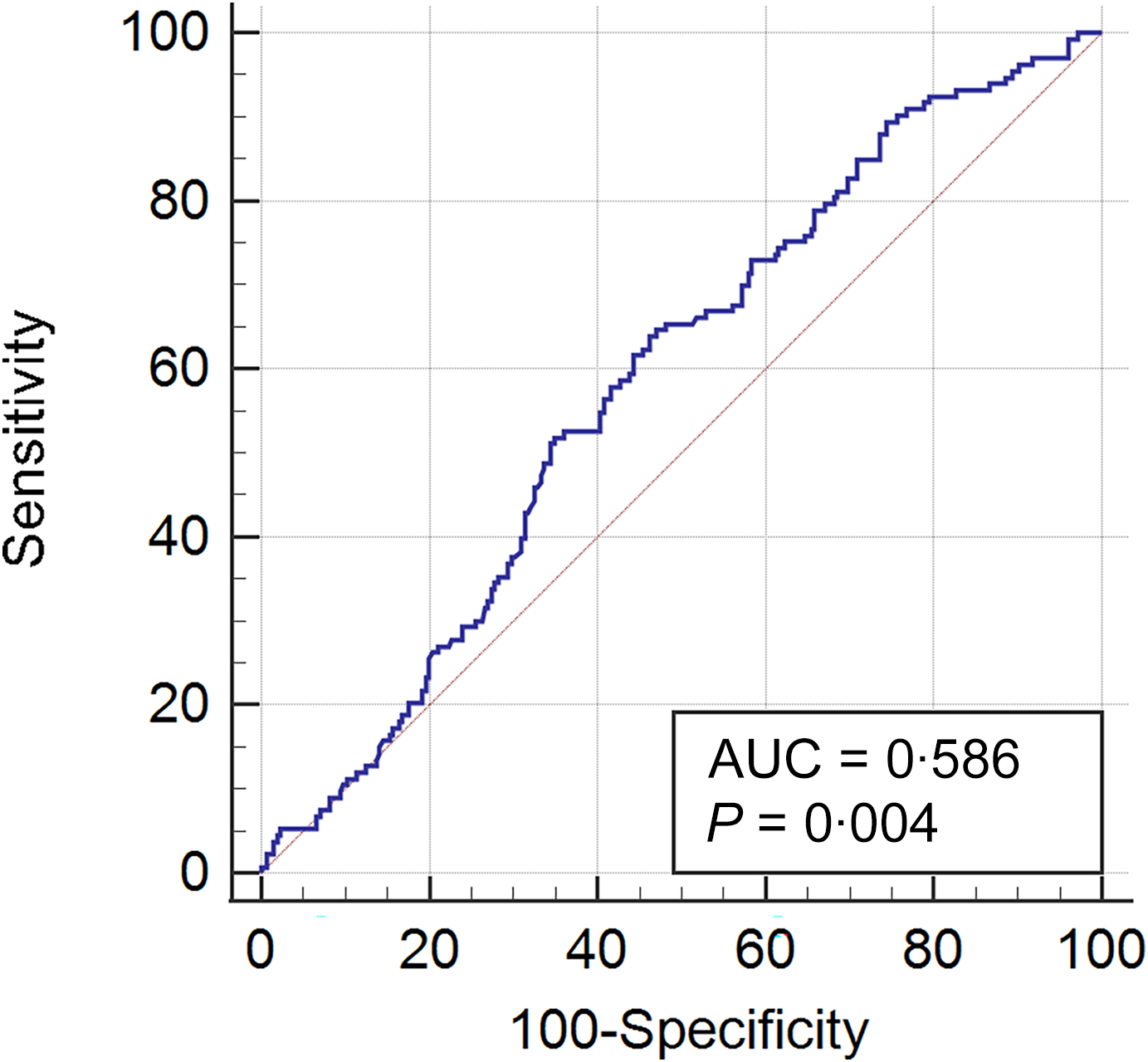
Blood samples to evaluate maternal thyroid function were available for 417 subjects. The median Tg value was 10·3 μg/l (IQR: 5·7–18·4 μg/l). UI/Creat and Tg were negatively correlated (P < 0·05, r = –0·17). Median Tg values were lower in women with UI/Creat ≥ 150 μg/g (8·3 μg/l, IQR: 5·1–14·8 μg/l) than in women with a UI/Creat < 150 μg/g (11·4 μg/l, IQR: 5·8–20·0 μg/l) (P = 0·005). Receiver operating characteristic curve analysis showed that a Tg value ≤ 10·61 μg/l (sensitivity: 63·9 %, specificity: 53·7 %, positive predictive value: 41·9 %, negative predictive value: 74·1 %, AUC: 0·586, 95 % CI: 0·528, 0·644) identified women with UI/Creat ≥ 150 μg/g (Figure 1). Tg was lower in those taking an ICS (median value 9·4 μg/l, IQR: 5·5–16·6 μg/l) than in those not taking one (median value 13·0 μg/l, IQR: 6·7–21·7 μg/l) (P < 0·01). Tg was low in both regular cow’s milk consumers (10·1 μg/l, IQR: 5·5–18·4 μg/l) and non-consumers (10·4 μg/l, IQR: 6·1–17·8 μg/l), the difference between them being non-significant (P = 0·6). At multiple linear regression analysis, only UI/Creat was associated with Tg, negatively (β = –0·16, P < 0·01, adjusted R-squared: 0·02). There were no differences in median Tg levels according to when the iodine supplementation was begun.
ROC curve analyses to identify the most accurate cut-off for thyroglobulin (Tg) serum levels to differentiate women with UI/Creat ≥ 150 μg/g from women with UI/Creat < 150 μg/g (sensitivity: 63·9 %, specificity: 53·7 %, PPV: 41·9 %, NPV: 74·1 %, AUC: 0·586, 95 % CI: 0·528, 0·644). NPV, negative predictive value; PPV, positive predictive value; ROC, receiver operating characteristic; UI, urinary iodine.
Secondary goal (iii): to assess the influence of iodine status on maternal thyroid function (TSH, FT4 and FT3) and on Tg values
Median TSH values were 1·7 mU/l (IQR: 1·3–2·2 mU/l), confirming our subjects as euthyroid. There was no correlation between TSH and either Tg, BMI or weight. TSH and UI/Creat were not correlated, regardless of whether UI/Creat was ≥ 150 μg/g or < 150 μg/g. At multiple linear regression analysis, no reliable model was identified after checking for assumptions. The median FT4 value was 12·1 ρmol/l (IQR: 11·0–13·1 ρmol/l). A negative correlation emerged between FT4 and BMI (P < 0·05, r = –0·02), but FT4 levels did not correlate with either UI/Creat or Tg, and there were no differences in the median FT4 values according to whether UI/Creat was ≥ 150 μg/g or < 150 μg/g. At multiple linear regression analysis, no reliable model was identified upon assumption checks. The median FT3 value was 4·1 ρmol/l (IQR: 3·8–4·4 ρmol/l). There was also a significant positive correlation between FT3 and BMI (P < 0·05, r = 0·23). No correlation emerged between FT3 levels and UI/Creat, and there were no differences in FT3 levels according to whether UI/Creat was ≥ 150 μg/g or < 150 μg/g. At multiple linear regression analysis, no reliable model was identified upon assumption checks. There was a significant positive correlation between FT3 and Tg (P < 0·05, r = 0·15). FT3 revealed to be higher in women with Tg > 10·61 μg/l (4·2 ρmol/l, IQR: 3·9–4·5 ρmol/l) than in women with Tg ≤ 10·61 μg/l (4·0 ρmol/l, IQR: 3·7–4·5 ρmol/l) (P < 0·01).
Secondary goal (iv): to assess the influence of maternal iodine status on the offspring’s TSH at neonatal screening
Neonatal TSH and neonatal parameters were available for 523 subjects. The median TSH value was 2·8 mU/l (IQR: 1·8–4·1 mU/l). We documented only one case of TSH > 20 mU/l in the series, consistent with congenital hypothyroidism (TSH = 50·3 mU/l). There was no significant correlation between neonatal and maternal TSH, nor between maternal UI/Cr and either Tg or maternal weight. Median TSH neonatal values did not differ according to whether the mother’s UI/Cr was ≥ 150 μg/g or < 150 μg/g or whether or not she was taking an ICS. The multiple linear regression analysis model identified only maternal FT3 (β = 0·35, P < 0·05), smoking habits (β = 4·42, P < 0·001) and BMI (β = 4·43, P < 0·01) as independent determinants of neonatal TSH values (adjusted R-squared: 0·08).
Secondary goal (v): to assess the influence of maternal iodine status on the pregnancy and the newborn’s outcomes
Median neonatal weight was 3320 g (IQR: 3020–3639 g). Neonatal weight had no direct correlation with UI/Creat, was negatively correlated with Tg (P < 0·05, r = –0·17) and was positively correlated with maternal weight (P < 0·05, r = 0·21) and BMI (P < 0·05, r = 0·17). Multiple linear regression analysis revealed maternal weight (β = 107·32, P < 0·001), Tg (β = –81·83, P < 0·001) and educational level (degree) (β = 115·74, P < 0·05) to be significant variables influencing neonatal weight (adjusted R-squared: 0·07). Specifically, for Tg, the negative β values indicate that neonatal weight increased as Tg levels decreased.
Median neonatal length was 49 cm (IQR: 47–50 cm). Neonatal length was not directly correlated with UI/Creat, but was negatively correlated with Tg values (P < 0·05, r = –0·13) and was also correlated with maternal weight (P < 0·05, r = 0·11). Multiple linear regression analysis revealed that maternal weight (β = 0·23, P < 0·05) and Tg (β = –0·3 P < 0·01) were significant determinants of neonatal length (adjusted R-squared: 0·02). Thus, for Tg, the negative β values indicate that neonatal length increased as Tg levels decreased.
Thirty-one babies out of 523 (5·9 %) were SGA. No association emerged between maternal UI/Creat (considered as categories) and SGA. We found no differences between SGA and non-SGA babies in median maternal TSH, UI/Creat or Tg. The mothers of SGA babies weighed less than the mothers of non-SGA children: 54·0 kg (IQR: 52·0–59·5 kg) v. 63·0 kg (IQR: 56·5–70·0 kg) (P < 0·0001). Logistic regression analysis showed that maternal weight was the only variable to influence the presence of SGA as a protecting factor (OR: 0·3, 95 % CI: 0·17, 0·65) (P < 0·001).
In the whole series, two cases of stillbirth were documented, and 163 patients had a history of previous miscarriages. No association was found between a previous history of miscarriage and either UI/Creat or Tg.
Twenty-eight cases of preterm delivery (< 37 gestational weeks) were documented. No association was found between UI/Creat and preterm delivery. ICS users had a lower rate of preterm delivery (15/368, 4·1 %) than non-users (13/123, 10·5 %) (χ 2(1) = 6·6, P = 0·03). No association was found with either regular cow’s milk/yogurt consumption or with IS. Women with preterm delivery tended to have higher Tg values (14·7 μg/l, IQR: 7·5–27·4 μg/l) than women with timely delivery (9·9 μg/l, 5·6–18·1 μg/l), although the difference was not statistically significant (P = 0·07). At the logistic regression analysis, higher Tg (OR: 1·52, 95 % CI: 1·20, 1·92; P < 0·01) and higher educational level (OR: 0·28, 95 % CI: 0·10, 0·77; P < 0·01) were significant independent determinants for preterm delivery, with higher Tg levels associated with a greater risk of preterm delivery.
Discussion
In the present survey, we found that pregnant women residing in north-eastern Italy had a median UI/Creat of 112·8 μg/g, far short of the target of iodine sufficiency in pregnancy, and were therefore still suffering from mild iodine deficiency. We also found that there had been no significant improvement in the same area since 2008(Reference Mian, Vitaliano and Pozza5), over which period we registered a median UIC among pregnant women of 83 μg/l, despite the more widespread use of IS during that time, up from 37·5–44·5 % to 76·9 %. There appears to be a mismatch between children and pregnant women in iodine status, as previous surveys in various European and non-European countries have also found(Reference Gowachirapant, Winichagoon and Wyss16–Reference Watutantrige Fernando, Cavedon and Nacamulli18). In Veneto, there is little difference in the use of IS between SACs (and their families) (81·6 %)(Reference Censi, Manso and Barollo13) and the pregnant women participating in the present study (76·9 %). Although IS plays a fundamental role in improving the iodine status of SACs(Reference Censi, Manso and Barollo13), it seems it is not equally effective during pregnancy. It could be that a lack of knowledge, especially among less educated women, of the importance of iodine for health – the responses to our questionnaire showed only around 22 % of pregnant women were aware of it − is at least in part responsible for the low use of any type of iodised salt. An alternative and more convincing explanation is that, given the greater need for iodine during pregnancy, the use of IS alone is not enough to reach an adequate iodine status. Indeed, multivariable analysis of the factors influencing iodine availability showed that only regular cow’s milk consumption and ICS use were independently associated with iodine sufficiency.
There was a high percentage of ICS users in our study (74·2 %), seemingly inconsistent with the low level of awareness of iodine prophylaxis. We think this can be explained by the fact that iodine is taken as part of a multivitamin preparation for pregnancy, rather than as a specific iodine supplement.
Regarding dietary factors, there has unfortunately been a tendency over recent decades towards a lower consumption of milk and dairy products(Reference Kearney19–Reference Nicklas21), which is a well-recognised factor in declining iodine status, especially among pregnant women.
Recently, Kelliher et al., in a study of 1059 pregnant women in Ireland, confirmed that inadequate iodine status during pregnancy persists even in Western settings. They also found that use of an ICS and a higher educational level in their cohort were associated with higher levels of urinary iodine during pregnancy. Interestingly, the winter season was also associated with a higher urinary iodine, in that study: indeed, it is well known that during winter the milk iodine content is higher, as a result of iodine-fortified feed, than during summer, when cows are pasture fed(Reference Kelliher, Kiely and Browne22). These data also highlight the role of milk in reaching an adequate iodine status in pregnancy.
The American Thyroid Association recommends that women living in the USA take a daily supplement of 150 μg of iodine during pregnancy(Reference Alexander, Pearce and Brent23). In support of this, our data show that regular use of an ICS is one of the two major determinants of adequate iodine status during pregnancy.
The chief message for women living in mild iodine-deficient areas is that they need both regular use of an ICS and an iodine-rich diet to guarantee adequate iodine status during pregnancy. However, given the difficulty of controlling or modifying dietary habits, pregnant women should be advised to regularly take an ICS. Gynaecologists in the Veneto region should take these data into account when deciding which types of supplements to recommend to pregnant women in this area, while at the same time stressing the importance of a diet with an adequate iodine content. Pregnant women on a vegan or vegetarian diet should take particular note of this message as they may need higher iodine supplementation than is generally recommended. Our findings also suggest that, as validated in other specifically designed studies, Tg may play a role in monitoring iodine status – both at the individual and population levels – alongside classical parameters such as median UIC and thyroid goitre prevalence.
Tg has previously been found to be a valuable biomarker of iodine status during pregnancy(Reference Eltom, Elnagar and Elbagir10–Reference Stinca, Andersson and Weibel12). In the present study, where most of the women began taking supplements at the beginning of pregnancy, data collected in the third trimester show that women with adequate iodine status (UIC ≥ 150 μg/g) and taking an ICS had significantly lower Tg values. Multiple regression analysis revealed that Tg was independently and uniquely influenced by iodine status. However, these data need further confirmation, because, although the correlations reached statistical significance, they were relatively weak, as indicated by the β values. All these data corroborate the value of Tg as a proxy of (long-term) iodine intake. In a multicentric study on around 600 pregnant women at different trimesters, Stinca et al concluded that a dried blood spot Tg value of around 10 μg/l indicated iodine sufficiency(Reference Stinca, Andersson and Weibel12). Interestingly, this dried blood spot-Tg value is similar to the serum Tg cut-off value for iodine sufficiency identified in the present study (≤ 10·61 μg/l). Although dried blood spot-Tg remains the most important method for evaluating Tg status in remote areas of the world, serum Tg may be a reliable additional method for evaluating individual iodine status in pregnant women residing in high-income countries, as it can be analysed in most laboratories. Nonetheless, this information should be interpreted with caution because, in our study, the level of accuracy associated with this cut-off was low, as indicated by the AUC, which was consistent with limited diagnostic accuracy.
Moreover, Tg levels may be elevated due to factors unrelated to iodine deficiency, such as increased thyroid volume, for instance in multinodular goitre, or may be falsely low in the presence of Tg autoantibodies (TgAb) associated with thyroid autoimmunity(Reference Giovanella, D’Aurizio and Algeciras-Schimnich24,Reference Moreno-Reyes, Fuentes Peña and Nuñez25) . These limitations should be considered when using Tg as a marker of iodine sufficiency, both at the individual and population levels.
In a cohort of mildly to moderately iodine-deficient women in the UK, Tg was a better functional marker of iodine status than TSH(Reference Bath, Pop and Furmidge-Owen26). Our study confirms these findings, as we found no association between urinary iodine levels and TSH. These data are not unexpected: thyroid-stimulating hormone (TSH) values are not commonly used to evaluate the iodine status of adults and SACs, since they overlap with widely differing levels of iodine intake(9). This seems to be also true for pregnant women, at least those living in areas of mild to moderate iodine deficiency(Reference Bath, Pop and Furmidge-Owen26), and our data provide further confirmation of this. Nor are thyroid hormones used as iodine status indicators, as T3 and T4 levels in iodine-deficient populations are often within the normal range, at least in the absence of severe deficiency(Reference Rohner, Zimmermann and Jooste27).
Indeed, we did not find any correlation between urinary iodine and FT3 and FT4 status, as expected. This may have to do with strict homeostatic regulation, which cannot be influenced by mild iodine deficiency, especially when a spot urine sample is taken as a surrogate. Furthermore, laboratory FT4 and FT3 values measured in the second part of pregnancy are imprecise and unreliable due to a series of changes that take place during this period, which may explain the different results compared with those reported in other studies evaluating thyroid hormones in early gestation(Reference Abel, Korevaar and Erlund28). Given all this, the positive correlation we found between Tg and FT3 values is particularly interesting. It is well known that the physiological responses to low iodine intake include preferential synthesis and release of T3 over T4 to reduce the iodine residue(Reference Rohner, Zimmermann and Jooste27). In our series, FT3 was higher, although within normal ranges, in pregnant women with Tg values consistent with iodine deficiency. All these data suggest that Tg is able to capture the compensatory mechanism that is typical of long-term iodine deficiency.
Regarding the effects of iodine on the offspring, it is well known that moderate to severe iodine deficiency during pregnancy has serious consequences for newborns’ outcomes and development(Reference Zimmermann29). However, it not clear whether mild to moderate iodine deficiency has a similar influence. Many studies have reported reduced birth weight(Reference Alvarez-Pedrerol, Guxens and Mendez30,Reference Charoenratana, Leelapat and Traisrisilp31) . The Avon Longitudinal Study of Parents and Children (ALSPAC), which included 3140 pregnancies in an area of mild-to-moderate iodine deficiency, found no significant association between maternal iodine status and either pregnancy or neonatal loss, nor with other adverse obstetric outcomes(Reference Torlinska, Bath and Janjua32). Abel et al. carried out a very large study of more than 70 000 pregnancies and found an association between daily iodine intake (evaluated from FFQ and ICS use) and birth weight, but not between UIC and weight(Reference Abel, Caspersen and Sengpiel33). In our study, we also found no association between urinary iodine levels and neonatal outcomes, but it is worth noting that there was a negative correlation between neonatal weight and length and Tg. The use of an ICS during pregnancy was associated with a lower rate of preterm delivery, in line with Abel et al.’s finding that a higher iodine intake and ICS use in pregnancy was associated with a lower likelihood of preterm delivery(Reference Abel, Caspersen and Sengpiel33), as well as with Lopes-Pereira et al.’s finding of a lower rate of adverse obstetric outcomes, including preterm delivery, in women taking supplements(Reference Lopes-Pereira, Quialheiro and Costa34). It is also interesting that women with preterm delivery tended to have higher Tg values, although the association was not statistically significant (P = 0·07), and, again, there was no association with urinary iodine. Multivariable analysis confirmed that Tg was associated with preterm delivery and birth weight and height. So, Tg, being a proxy of long-term intake, could better reflect the consequences of mild to moderate iodine deficiency during pregnancy than urinary iodine concentration, as previously suggested(Reference Katko, Gazso and Hircsu35). Nonetheless, the β coefficient and the OR show that the observed correlations, although statistically significant, were rather weak, and therefore call for caution and the need for confirmation in larger cohorts and prospective studies. Moreover, as also indicated by the β coefficients, the absolute changes in weight and height associated with Tg were small, limiting the clinical significance of these findings, although they remain informative for understanding the role of Tg as a marker of iodine status.
The possible role of Tg as an individual marker of iodine status merits further investigation. Indeed, the fact that it reflects iodine intake in the preceding weeks and months makes it particularly promising for this purpose. Different RCT carried out in areas of mild to moderate iodine deficiency have documented a progressive fall in Tg after long-term iodine supplementation(Reference Censi, Watutantrige-Fernando and Groccia6,Reference Ma, Venn and Manning36,Reference Chong, Shi and Shan37) . However, a validation study in which multiple urinary iodine measurements were taken prior to the Tg evaluations would be needed to definitively test this hypothesis. Our findings provide the first published evidence that Tg can predict neonatal parameters and pregnancy outcomes. If further studies show that Tg may be used as an individual marker of iodine status in pregnancy, its intrinsic properties (i.e. its ability to respond to the slightest variation in TSH, which changes in relation to iodine status) and its relationship with parameters of maternal and newborn outcomes may be used in individual pregnancies to adjust the amount of supplementary iodine in order to prevent deficiencies or excesses of iodine intake, both of which are detrimental to the wellbeing of the fetus.
When pregnancies are analysed in mild to moderate iodine areas, it seems that, along with mild iodine deficiency, mother-related factors, such as maternal weight and education, also have a large impact on pregnancy outcomes. A higher level of education is a protective factor, presumably because it is related to more informed behaviour during pregnancy, and possibly better access to medical consultations. Maternal weight is one of the mother-related factors that can influence neonatal weight and the frequency of SGA(Reference Moreira and Méio38). In this regard, however, we should point out that as the principal focus of our study was on iodine status, we were unable to comprehensively evaluate the many factors potentially influencing the complex pathogenesis of SGA; we can only state that mild to moderate iodine deficiency does not play a role.
Our study highlights the association between Tg and iodine status in the third trimester of pregnancy, as well as the potential link between Tg and certain neonatal outcomes influenced by iodine status. These findings may serve as the basis for future studies specifically designed to explore this link, which could impact both iodine supplementation strategies during pregnancy and the assessment of individual iodine sufficiency. It may be especially useful and cost-effective in assessing iodine status in certain populations, as it offers several advantages over classical methods based on median urinary concentrations. It is relatively easy to sample (potentially also from a capillary blood sample), reflects long-term iodine status and could be highly valuable if confirmed as a reliable proxy for individual iodine status.
Our study has several limitations that should be taken into account when interpreting the findings: (1) the data on iodine status in pregnancy were limited to the third trimester, while the first weeks of pregnancy are the most important periods in fetal development. Although Tg reflects long-term iodine status, measuring it in the third trimester may not accurately capture iodine status during early pregnancy. (2) Food intake frequency is problematic as a means of evaluating the actual amount of dietary iodine intake. The questionnaire investigated the weekly consumption frequency rather than the quantity consumed, which may represent a limitation in accurately assessing intake. The fact that it was not a validated questionnaire for assessing iodine intake may have been a further limitation. However, this is the same questionnaire we have been using for many years in all our previous studies and population surveys(Reference Censi, Watutantrige-Fernando and Groccia6,Reference Censi, Manso and Barollo13,Reference Watutantrige Fernando, Cavedon and Nacamulli18) . (3) Some missing data on urinary iodine and Tg may have affected the accuracy of the analysis. (4) TgAb were not assessed in this study, so a possible interference with Tg measurements cannot be ruled out. (5) The most crucial limitation concerns the absence of follow-up data on the impact on the women of the iodine deficiency encountered, as well as on the neurological development of their offspring, the most important goal of iodine prophylaxis in pregnancy.
In conclusion, in areas of mild to moderate iodine deficiency, specific ICS supplementation is needed during pregnancy to attain iodine adequacy. Mild to moderate iodine deficiency also seems to play a role in fetal growth and pregnancy outcomes. Tg may be a possible proxy of iodine adequacy in the third trimester of pregnancy, a reliable marker of thyroid function and a factor associated with maternal and neonatal outcomes during pregnancy.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526106989
Acknowledgements
We thank Tessa Say for text editing. In memoriam Maria Elisa Marisa Girelli, one of the first scholars in Italy to evaluate the role of milk in influencing iodine status.
This research received funds from PRIN 2022 PNRR Next Generation EU, Project P20228RP2Z ‘The relevance of iodine in human nutrition: filling the gap from the farm to the fork’.
S. C.: original draft (lead), writing – review (lead), editing (equal), data elaboration (equal). G. M.: original draft (equal), writing – review (equal), data collection (lead). G. A.: original draft (supporting), writing – review (equal), data collection (equal), data elaboration (lead). E. R.: writing – review and editing (supporting), data collection (supporting). C. C.: writing – review and editing (supporting), data collection (supporting). I. P.: writing – review and editing (supporting), data collection (supporting). J. M.: writing – review and editing (supporting), data collection (equal). D. B.: writing – review and editing (supporting); methodology (equal). I. M-B.: writing – review and editing (supporting); methodology (equal). L. B.: writing – review and editing (supporting), data collection (supporting). S. B.: writing – review and editing (supporting), data collection (supporting). L. M.: writing – review and editing (supporting), data collection (supporting). M. C.: writing – review and editing (supporting), data collection (supporting). A. A.: writing – review and editing (supporting), data collection (supporting). C. M.: original draft (equal), writing – review (equal), editing (lead), methodology (lead).
The authors have no competing financial interests to disclose.



 Open access
Open access