


Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD)(Reference Keating, Owen and Pugh1) is the most common cause of chronic liver disease impacting more than 30% of adults worldwide, with vast global and regional variations in prevalence(Reference Keating, Owen and Pugh1). The Middle East and North Africa harbour the highest prevalence (42.6%)(Reference Kan, Zhang and Wang2,Reference Younossi, De Avila and Petta3) followed by East Asia and South Asia(Reference Kan, Zhang and Wang2). Western Europe has observed the fastest relative increase since 1990(Reference Kan, Zhang and Wang2) and low-middle income regions including sub-Saharan Africa and Latin America have also observed a steep rise in MASLD prevalence in the last decade, linked to shifts to increasingly obesogenic environments(Reference Xu, Li and Pi4). Disparities in prevalence and burden are likely linked to sociocultural determinants of health such as low socio-economic status, lower education, poor health literacy, environmental factors and systemic inequities related to race and ethnicity(Reference Abu-Rumaileh, Dhoop and Pace5). These factors can intersect, leading to poor diet quality, low physical activity (PA) and poorer sleep quality and duration. Moreover, individuals from lower socio-economic backgrounds and those from migrant populations face systemic healthcare barriers and experience a disproportionately higher burden of MASLD(Reference Lorek, Łupina and Bisaga6).
MASLD is underpinned by metabolic risk factors such as abdominal obesity, insulin resistance and cardiometabolic dysregulation(Reference Younossi, De Avila and Petta3). In all people living with MASLD, lifestyle therapy (diet, PA and sleep) is the cornerstone of management. Additional medical and pharmacotherapy strategies, including thyroid hormone receptor beta agonists and incretin-based treatments, and bariatric surgery provide further substantial benefit but are not readily available from a global perspective. Therefore, standalone and adjunct lifestyle management strategies that are accessible, culturally safe and culturally responsive are urgently needed to meet the substantial and increasing global population with MASLD.
Despite recommendations within MASLD clinical guidelines for provision of lifestyle management, most people do not have sufficient or sustainable access to evidence-based care. Country-specific strategies for MASLD management are sparse and generally focus on management in primary and tertiary care settings. Access to allied healthcare professionals (HCP) is not generally integrated into usual care and not readily available within mainstream healthcare despite the fact that behaviour change can be optimised with HCP support(Reference Dennis, Ball and Harris7). Moreover, global workforce limitations within healthcare and maldistribution need to be considered when designing accessible management strategies; balancing the large and growing proportion and geographical location (e.g. urban vs. regional vs. rural) of people impacted, with the need for prevention and management to mitigate disease progression and detrimental health outcomes(Reference Spillman, Backhouse and Cox8).
This review is to consider the current and emerging evidence for multidisciplinary lifestyle management (diet, PA and sleep) of MASLD in the context of providing accessible, scalable and culturally safe and responsive care, to better meet the diverse needs of people living with MASLD globally.
Lifestyle management of metabolic dysfunction-associated steatotic liver disease and associated sociocultural considerations
Lifestyle behaviours, including poor dietary habits, increased sedentary time, low levels of PA and smoking are the primary modifiable drivers of MASLD(Reference Kanwal, Neuschwander-Tetri and Loomba9). It is also established within similar chronic conditions that poor sleep (quality and quantity) can exacerbate poor diet, physical inactivity and adverse metabolic health outcomes.
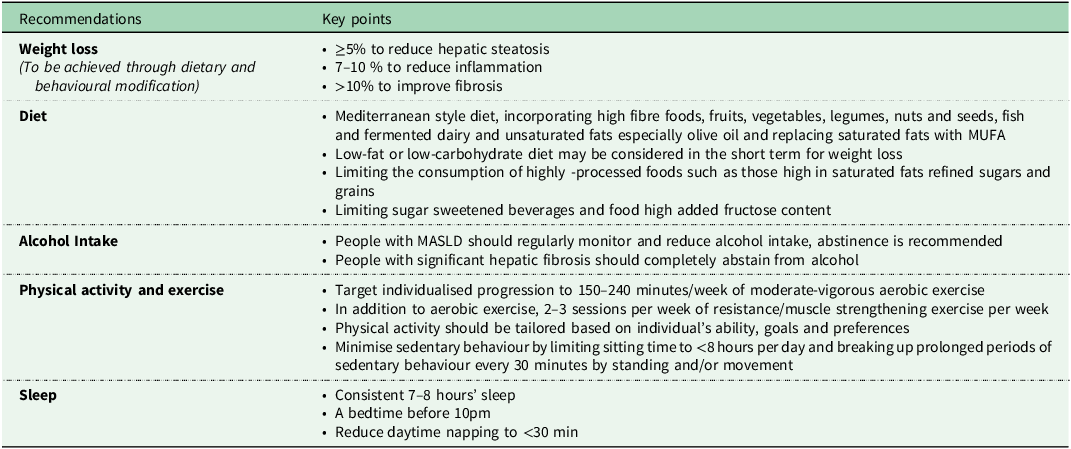
Key literature reinforces evidence-based lifestyle recommendations for MASLD (Table 1). Clinical practice guidelines consistently recommend first line therapy targeting weight loss of at least 5% to improve hepatic steatosis, while greater reductions of at least 7–10% are required to reduce hepatic inflammation and regress liver fibrosis(Reference Kanwal, Neuschwander-Tetri and Loomba9–Reference Thursz, Gual and Lackner11). MASLD has a bidirectional relationship with obesity and insulin resistance and there is ample evidence to support the notion that weight loss in individuals with MASLD leads to an improvement and/or resolution of hepatic steatosis, liver inflammation and fibrosis, improvement in cardiometabolic risk factors and enhanced insulin sensitivity(Reference Koutoukidis, Astbury and Tudor12,Reference Koutoukidis, Koshiaris and Henry13) .
A brief overview of lifestyle recommendations for MASLD management according to key international clinical practice guidelines

Table 1. Long description
The table outlines key lifestyle recommendations for managing Metabolic Associated Steatotic Liver Disease (MASLD). It includes four main categories: weight loss, diet, alcohol intake, physical activity, and sleep. The weight loss section advises achieving at least five percent weight reduction to improve hepatic steatosis, seven to ten percent to reduce inflammation, and over ten percent to improve fibrosis. The diet section recommends incorporating fiber, fruits, vegetables, legumes, nuts, and seeds, and replacing saturated fats with monounsaturated fats such as those found in the Mediterranean diet. It also suggests considering low-fat or low-carbohydrate diets for weight loss, limiting highly processed foods high in saturated fats and refined grains, and limiting foods and beverages with high added fructose content. The alcohol intake section advises regular monitoring and reduction of alcohol intake for people with MASLD and complete abstinence for those with significant hepatic fibrosis. The physical activity section recommends aiming for one hundred fifty to two hundred forty minutes per week of moderate-to-vigorous aerobic exercise, along with two to three sessions per week of resistance or muscle-strengthening exercise. It also advises tailoring physical activity based on individual ability, goals, and preferences, and minimizing sedentary behavior by limiting sitting time to less than eight hours per day and breaking up prolonged periods of sedentary behavior every thirty minutes by standing and or movement. The sleep section recommends consistent seven to eight hours of sleep, a bedtime before ten pm, and reducing daytime napping to less than thirty minutes.
Note: Recommendations are derived from the clinical practice guidelines for MASLD issued by the American Association for the Study of Liver Diseases (AASLD)(128), the European Association for the Study of the Liver (EASL)(Reference Sberna, Bouillet and Rouland129) and the Asian Pacific Association for the Study of the Liver (APASL)(Reference Shiha, Ibrahim and Helmy130).
Weight loss through dietary changes and PA is the primary management strategy for MASLD, however there are challenges in achieving and maintaining healthy lifestyle behaviours and sustaining weight loss. In-depth qualitative explorations have highlighted a need for more tailored recommendations, with participants expressing a desire for personalised guidance on diet and PA, as well as information on pharmacological and procedural weight loss options(Reference Tincopa, Wong and Fetters14,Reference Avery, Exley and McPherson15) .
It is important to note that individuals who utilise pharmacotherapies to achieve weight loss (e.g. GLP-1 analogues) or manage disease (e.g. Resmetirom), or those who undergo surgical interventions (e.g. bariatric surgery), should also be co-prescribed lifestyle intervention to improve diet, exercise and behaviours in the short- and longer-term and counteract potential side effects associated with weight loss (e.g. inadequate nutritional intake, muscle loss)(Reference Amini, Burkholder and Allencherril16). Furthermore, the enhanced combination of lifestyle behaviour changes improves long-term sustainability and health outcomes, self-management and patient empowerment, and overall, lifestyle interventions are a lower-cost solution with minimal adverse outcomes(Reference Zhang, Xi and Liu17,Reference Kwon, Choi and Jang18) .
Conversely there are a subgroup of individuals who are within what is considered the healthy BMI range who also experience MASLD. This is referred to as lean MASLD and evidence for optimal management in this subgroup is not well established. Although significant weight loss is not appropriate in lean MASLD, it is prudent that diet and structured exercise are still central to MASLD management.
Our recent co-design work with people living with MASLD has also highlighted their desire for tailored advice to improve sleep(Reference Sood, Roberts and Scott19). To facilitate improvements in lifestyle behaviours, individuals with MASLD require education about the hepatic and cardiovascular benefits of improving diet quality, PA and sleep, along with the enhanced benefits of energy restriction(Reference Kenneally, Sier and Moore20). Providing personalised lifestyle recommendations based on individual needs is essential for effective and sustainable intervention. Inadequate disease knowledge and misperceptions regarding the pathogenesis and consequences of MASLD have been associated with suboptimal dietary and PA behaviours, including substance misuse behaviours (smoking and/or alcoholism)(Reference Carrieri, Mourad and Marcellin21–Reference Zelber-Sagi, Bord and Dror-Lavi23). Awareness of MASLD remains low across the general population, as well as in high-risk groups, and those with established MASLD, often leading to reduced motivation to engage in recommended lifestyle modifications(Reference Tincopa, Wong and Fetters14,Reference Alqahtani, Paik and Biswas24,Reference Alemany-Pagès, Moura-Ramos and Araújo25) . A common misperception involves mixing disease aetiologies, with excessive alcohol consumption often considered as the primary cause of adverse hepatic outcomes and viewing poor diets or sedentary behaviours as negligible risk factors(Reference Morrill, Crocker and Hingle26). Healthcare settings should educate patients about the modifiable risk factors associated with MASLD and address common misconceptions, with strong emphasis on the fact that MASLD is a reversible condition, even in its advanced stages, through achievable lifestyle interventions. Patients should be guided towards reliable platforms that provide evidence-based information for disease management, particularly through online resources, healthcare consultations, or community-based programmes. Moreover, it is important to address barriers to adopting a healthy lifestyle in MASLD, that extend beyond conventional healthcare and management, including personalised approaches that target social-cultural factors including considerations surrounding beliefs, food practices and social norms within diverse Culturally and Linguistically Diverse(Reference Rinella, Neuschwander-Tetri and Siddiqui27) communities(Reference Kravchuk, Bychkov and Kozyk28).
Evidence-based diets and metabolic dysfunction-associated steatotic liver disease
There is consistent evidence that diet plays a central role in the management MASLD(Reference Hydes, Ravi and Loomba29,Reference Zelber-Sagi, Ratziu and Oren30) . International MASLD guidelines indicate that hypocaloric diets with a about 500–1000 kcal/day deficit including low-fat, low-carbohydrate or very low-carbohydrate ketogenic diets targeting weight loss significantly reduce liver fat, reduce inflammation and fibrosis and improve metabolic health. These diets encompass high-quality nutrients including unsaturated fatty acids and plant proteins(Reference Shan, Guo and Hu31). There is also a direct link between diets high in phytonutrients and reduced inflammation and oxidative stress, neutralising harmful free radicals and decreasing the production of pro-inflammatory molecules leading to improvements in the gut microbiota(Reference Roager, Vogt and Kristensen32). Nonetheless, discrepancies exist with defining optimal macronutrient composition with low-carbohydrate diets including energy from carbohydrates ranging from 8% to 45%, and low-fat diets ranging from 15% to 30% of energy from fat(Reference Roager, Vogt and Kristensen32). In cases where restrictive diets provide high animal protein and/or high saturated fat composition, they may not be sustainable and lead to adverse cardiometabolic risks, but there is limited evidence on their long-term safety benefits(Reference Zelber-Sagi, Grinshpan and Ivancovsky-Wajcman33).
Dietary patterns
Mediterranean diet (MedDiet) emphasises intake of vegetables, fruits, whole grains, legumes, nuts, olive oil and moderate fish consumption and is recommended as the optimal diet for MASLD management(34). MedDiet can elicit reduced liver fat independent of weight loss due to the anti-inflammatory and insulin-sensitising effects(Reference Ryan, Itsiopoulos and Thodis35). The high-quality, healthy MedDiet pattern emphasising non-refined cereals, fruits and vegetables, legumes, MUFA and n-3 fatty acids, polyphenols and carotenoids elicits hepatic and cardiovascular benefits in people with MASLD, particularly those within Mediterranean populations. More recently, it has been demonstrated that MedDiet can be adapted to diverse Western populations and still exhibit comparable benefits(Reference Romero-Gómez, Zelber-Sagi and Trenell36–Reference Papamiltiadous, Roberts and Nicoll39). It is plausible that when combined with energy restriction, the hepatic and cardiometabolic benefits are heightened. The MedDiet is a high-fat diet with 35–45% of energy coming from carbohydrates, 15–20% from protein and 35–45% from fats of which at least half are derived from MUFA. Alongside these hepatic benefits, individuals with the highest adherence to the MedDiet have a significantly lower relative risk (RR) of CVD events compared to those with the lowest adherence both in Med (RR 0.61, 95% CI: 0.46 to 0.79) and non-Med populations (RR 0.79, 95% CI: 0.70 to 0.89)(Reference Rosato, Temple and La Vecchia40). However, the use of foods native to Mediterranean regions may present economic and cultural barriers for adopting the MedDiet in non-Mediterranean regions. Tailored dietary modifications with cultural and personal preferences are achievable and may help promote long-term adherence and compliance(Reference George, Kucianski and Mayr41).
There is limited evidence for alternative diets in MASLD management. Intermittent fasting or time-restricted eating has recently gained attention due to the potential metabolic benefits, weight loss, improved insulin sensitivity and reduction in liver fat(Reference Yin, Li and Xiang42,Reference Hua, Yang and Li43) . A systematic review and meta-analysis of RCT conducted among individuals with MASLD, comparing intermittent fasting with either no intervention or alternative interventions, reported significantly greater reductions in body weight, BMI and liver enzyme levels in favour of intermittent fasting(Reference Yin, Li and Xiang42). However, evidence remains scarce for the long-term feasibility and safety of these dietary behaviours within the MASLD population. A Western dietary pattern, characterised by high intakes of ultra-processed foods, energy, refined grains, saturated and trans fats, red and processed meats, sugar-sweetened beverages and Na combined with low intakes of essential micronutrients, is associated with an approximately 50% increased likelihood of developing MASLD pathogenesis(Reference Berná and Romero-Gomez44,Reference Ullah, Rauf and Nabi45) .
Alcohol
There is heterogeneity in the findings regarding the impact of alcohol consumption on MASLD. Some studies have reported that low to moderate alcohol intake is associated with lower odds of MASLD and its more advanced forms metabolic dysfunction-associated steatohepatitis (MASH) and liver fibrosis compared to complete abstinence in the general population(Reference Weng and Dunn46). Conversely, other evidence suggests that any level of alcohol consumption may be harmful in individuals with established MASLD(Reference Jarvis, O’Keefe and Craig47). The purported protective effects of alcohol may be attributed to the presence of polyphenols, particularly in red wine, which possess cardioprotective and anticarcinogenic properties(Reference Arranz, Chiva-Blanch and Valderas-Martínez48). However, increased alcohol intake often coexists with underlying metabolic dysfunction, contributing to the development of metabolic dysfunction and alcohol-associated liver disease (MetALD). Individuals with MetALD tend to experience more severe disease progression and have a higher risk of mortality than those without excessive alcohol use(Reference Younossi, Stepanova and Ong49). Therefore, clinical guidelines recommend that individuals with MASLD should regularly monitor their alcohol consumption in line with recommendations and those with clinically significant fibrosis (stage F ≥ 2, on a scale from F0–F4, where F0 indicates no fibrosis and F4 indicates cirrhosis) are advised to abstain completely from alcohol(Reference Rinella, Neuschwander-Tetri and Siddiqui27).
Coffee
Regular coffee consumption, estimated at least three cups per day has been recommended in some clinical practice guidelines(Reference George, Lau and Kawaguchi10,Reference Thursz, Gual and Lackner11) , with observational evidence suggesting a lower RR of developing MASLD(Reference Hayat, Siddiqui and Okut50) and 33% lower odds of liver fibrosis progression among those with established MASLD(Reference Kositamongkol, Kanchanasurakit and Auttamalang51). There is also evidence to suggest that coffee consumption is associated with less risk of liver cirrhosis, liver-related death and liver cancer in observational studies(Reference van Dam, Hu and Willett52). Coffee contains antioxidants and bioactive compounds that may lower inflammation and improve metabolism and reduce liver disease risk. However, the benefits for liver health are primarily derived from observational studies, with limited evidence supporting benefits from clinical trials(Reference Linden-Torres, Zambrano-Galvan and Sahebkar53).
Barriers, enablers and sociocultural considerations for diet in metabolic dysfunction-associated steatotic liver disease
While the MedDiet is recommended as the gold standard for MASLD regression, several barriers have been reported for its adoption especially in non-Mediterranean regions and among individuals with MASLD(Reference Tincopa, Wong and Fetters14,Reference Avery, Exley and McPherson15) . These include lack of access to and affordability of healthy foods, limited nutritional knowledge and cooking skills, lack of convenience and an obesogenic environment and difficulty in translating MedDiet cuisine to multiethnic traditional cuisines(Reference Younossi, De Avila and Petta3,Reference Keating, Sabag and Hallsworth54) . Healthcare providers, particularly dietitians, should support individuals to understand and recognise the evidence-based nutrients and food components of MedDiet which elicit health benefits, and where appropriate, translate these components in a manner that aligns with cultural and personal preferences(Reference George, Kucianski and Mayr41,Reference Haigh, Bremner and Houghton55) . However, clinicians report limited training and inadequate time and resourcing to support behaviour change(Reference Mayr, Kelly and Macdonald56). Barriers to uptake of nutrition recommendations in Culturally and Linguistically Diverse (CALD) people includes language and cultural differences as well as low health literacy and socio-economic factors that include cost and time. Navigating the healthcare system(Reference Khatri and Assefa57) also presents as a challenge and this is exacerbated by food insecurity, lack of culturally safe and appropriate services and inadequate or confusing education around nutrition. This may include a lack of consideration of cultural differences including cultural norms surrounding food and mealtimes, family meal sharing practices that may differ from national guidelines, as well as lack of readily available culturally appropriate food and ingredients, particularly for individuals from CALD backgrounds who are adjusting to a different food environment.
Physical activity, structured exercise and metabolic dysfunction-associated steatotic liver disease
Exercise recommendations
Engaging in regular PA, including exercise (defined as planned and structured PA for the purpose of maintaining or improving health, wellbeing and/or performance), provides substantial hepatic and cardiometabolic benefits, independent of weight loss(Reference Keating, Hackett and George58,Reference Babu, Csader and Lok59) . General recommendations across societies recommend at least 150 minutes per week of moderate-intensity exercise, including both aerobic and resistance training(Reference Younossi, Zelber-Sagi and Lazarus60). Evidence supports that 150 to 240 minutes per week of at least moderate-intensity aerobic exercise can reduce hepatic steatosis by approximately 2–4% (absolute reduction), although reductions have also been observed with as little as 135 minutes per week(Reference Keating, Sabag and Hallsworth54). This level of structured exercise can also improve cardiorespiratory fitness, reduce central adiposity, improve health-related quality of life and cardiometabolic health(Reference Keating, Sabag and Hallsworth54). Emerging evidence suggests that aerobic exercise can also lead to improvements in surrogate markers of MASH resolution and histological severity. Exercise led to a about 5-fold greater likelihood of achieving a ≥ 30% reduction in MRI-measured liver fat than controls(Reference Cuthbertson, Keating and Pugh61), and better MASH Resolution Index scores than standard care (mean difference: −0.66, p = 0.046)(Reference Keating, Owen and Pugh1), independent of significant weight loss.
Regular progressive resistance training also offers benefits, such as improved insulin sensitivity, muscle strength and muscle mass, but its efficacy in reducing liver fat is less consistent compared to aerobic exercise. While there is limited evidence evaluating the efficacy of combined aerobic and resistance training for reducing hepatic steatosis in people with MASLD, this approach is likely the most practical for holistic health benefits so long as sufficient aerobic exercise is undertaken(Reference Keating, Sabag and Hallsworth54). However, resistance training should be prioritised in people actively undertaking weight loss via surgical or pharmacological approaches to minimise lean muscle mass losses and maintain or improve neuromuscular function, especially in those with co-existing sarcopenia, frailty and type 2 diabetes (T2D)(Reference Keating, Sabag and Hallsworth54). Sarcopenia is strongly associated with MASLD progression (adj OR 2.08 (95% CI 1.58, 2.74)] as well as MASLD-related mortality (adj OR 1.59 (95%CI 1.33, 1.91)(Reference Li, He and Sun62). These models typically accounted for key confounders such as age, sex and BMI, although covariates varied across studies. The combination of central obesity and sarcopenia (termed sarcopenic obesity) was associated with significantly worse metabolic profiles, advanced fibrosis and higher CVD risk(Reference Elsabaawy, Ragab and Abd-Elrazek63). While few studies have evaluated the efficacy of combined aerobic and resistance training for MASLD, comprehensive exercise programming should include both, tailored for individual needs, preferences and priorities. Resistance training prescription should target 8–10 multi-joint and large muscle group exercises, progression to 2–4 sets of 8–10 repetitions at moderate to high intensity (about 70–84% 1-repetition maximum) that can include body weight exercises, machine-based resistance exercises, hand weights or elastic band exercises, in line with recommendation for the management of T2D(Reference Hordern, Dunstan and Prins64).
Importantly, recommendations for structured exercise should include behavioural change strategies and be tailored to an individual’s capacity, cultural needs and personal preferences to promote sustained adherence(Reference Keating, Sabag and Hallsworth54). Emerging evidence from observational data suggests that concentrating the recommended levels of moderate-vigorous PA into 1–2 days per week (termed the ‘weekend warrior’ pattern) may protect from MASLD and all-cause mortality comparably to more traditional regular structured exercise patterns(Reference Zelber-Sagi, Paik and Ivancovsky-Wajcmen65). Moreover, epidemiological data indicated that any weekly frequency of moderate-vigorous PA reduced the risk of developing MASLD and facilitated MASLD resolution in over 200K adult men and women undertaking an occupational health screening programme in South Korea(Reference Sung, Ryu and Lee66). More frequent PA (≥5 days/week) was associated with a 16% reduction in MASLD incidence and a 40% increase in resolution of existing MASLD(Reference Sung, Ryu and Lee66). Other emerging intermittent PA approaches such as ‘exercise snacks’ and ‘vigorous intermittent lifestyle physical activity’, that involve brief (1–2 minute) vigorous-intensity efforts during regular daily activities may also provide sustainable solutions, although evidence in MASLD is lacking(Reference Keating, Chawla and De67). High levels of sedentary behaviour are an independent risk factor for MASLD, notably in people who do not undertake any vigorous PA(Reference Zhou, Li, Wang and Li68). Moreover, in those with MASLD and obesity, sedentary time is independently associated with increased levels of liver stiffness(Reference Bianco, Bonfiglio and Franco69). While there are no data to specifically inform sedentary behaviour intervention targets in MASLD, given these associations, it is prudent to recommend reducing sedentary behaviour in line with general guidelines as part of MASLD care (Table 1).
Barriers, enablers and sociocultural considerations for exercise in metabolic dysfunction-associated steatotic liver disease
Commonly reported barriers to the uptake and maintenance of PA in people with MASLD include lack of information about the benefits of exercise for MASLD and tailored exercise recommendations, fatigue, pain and low energy, co-morbidities and traditional barriers such as lack of time, cost of exercise programmes, limited access to equipment or facilities and competing work or family commitments(Reference Stine, Soriano and Schreibman70–Reference Keating, de Boer and Catsoulis74). Many of these barriers are augmented in CALD populations and those living in rural and remote communities who experience higher levels of obesity and related disease, linked with sociocultural determinants.
CALD communities may lack access to culturally safe exercise spaces, experience financial constraints and social isolation, all of which reduce PA participation(Reference Wang, Dowsey and Woodward-Kron75). A recent scoping review highlighted that perceptions of PA, acceptability and access are shaped by cultural identity and migration experiences(Reference Arefhosseini, Ebrahimi-Mameghani and Naeimi76). For example, some CALD groups may prioritise work and family obligations over personal health or may not view structured exercise as culturally appropriate. Migration often results in a decline in leisure-time PA, especially among women(Reference Zou, Kadri and Shao77). Acculturation challenges, such as adapting to new social norms and environments, can contribute to this decline. Moreover, cultural beliefs about body image, sex roles and traditional health practices may conflict with Western exercise norms. Environmental and logistical challenges, such as lack of culturally safe spaces, transport and cost can deprioritise PA and active care in CALD people with MASLD(Reference Arefhosseini, Ebrahimi-Mameghani and Naeimi76,Reference Caperchione, Kolt and Mummery78) . There is a dearth of literature evaluating the prevalence of MASLD in Indigenous peoples, and no studies have evaluated the barriers and enablers to, or efficacy of, exercise programmes for MASLD in this population(Reference Dick, Wheeler and Keating79). However, opportunities to improve the management of MASLD among Aboriginal and Torres Strait Islander peoples have been strongly advocated, guided by the Cultural Determinants of Health Framework(Reference Dick, Wheeler and Keating79).
Sleep and metabolic dysfunction-associated steatotic liver disease
Despite growing interest in the role of lifestyle factors in MASLD, the influence of sleep quality and duration remains underexplored. A recent review synthesising findings from five cross-sectional studies and one cohort study reported a 19% increased risk of MASLD among individuals with short sleep durations (<5–6 hours)(Reference Wijarnpreecha, Thongprayoon and Panjawatanan80). This association was corroborated by findings from a larger cohort study with a mean follow-up period of four years which found that short sleep duration was independently associated with an increased risk of incident MASLD(Reference Um, Chang and Jung81). There is also evidence that individuals diagnosed with MASLD exhibit significantly poorer sleep efficiency, more frequent daytime napping (>30 minutes), increased reliance on sleep medications and delayed sleep – wake timing compared to non-MASLD counterparts(Reference Zarean, Looha and Amini82,Reference Peng, Lin and Wang83) . While emerging evidence suggests that maintaining optimal sleep duration (7-8 hours) and limiting daytime naps may confer protective effects against MASLD, further investigation is warranted to elucidate the mechanistic pathways through which sleep influences inflammatory responses, appetite regulation via hormonal signalling, metabolic homeostasis and the downstream effects of fatigue on PA and dietary behaviours(Reference Wijarnpreecha, Thongprayoon and Panjawatanan80). Given the interrelationship between diet, exercise and sleep and the limited evidence to suggest potential benefits of improved sleep quality and quantity further research is warranted.
Barriers, enablers and sociocultural considerations for sleep in metabolic dysfunction-associated steatotic liver disease
Both language and cultural differences in terms of perception of sleep may result in underreporting or miscommunication about sleep issues which may limit access to management strategies that are in line with cultural needs. Furthermore, management strategies in terms of what is considered normal for sleep may vary and strategies that are aligned with Western culture may not be considered within the realms of cultural values of CALD individuals making them less effective and acceptable(Reference Glyn-Blanco, Lucchetti and Badanta84–Reference Alegría, Pescosolido and Williams86).
Lifestyle management summary
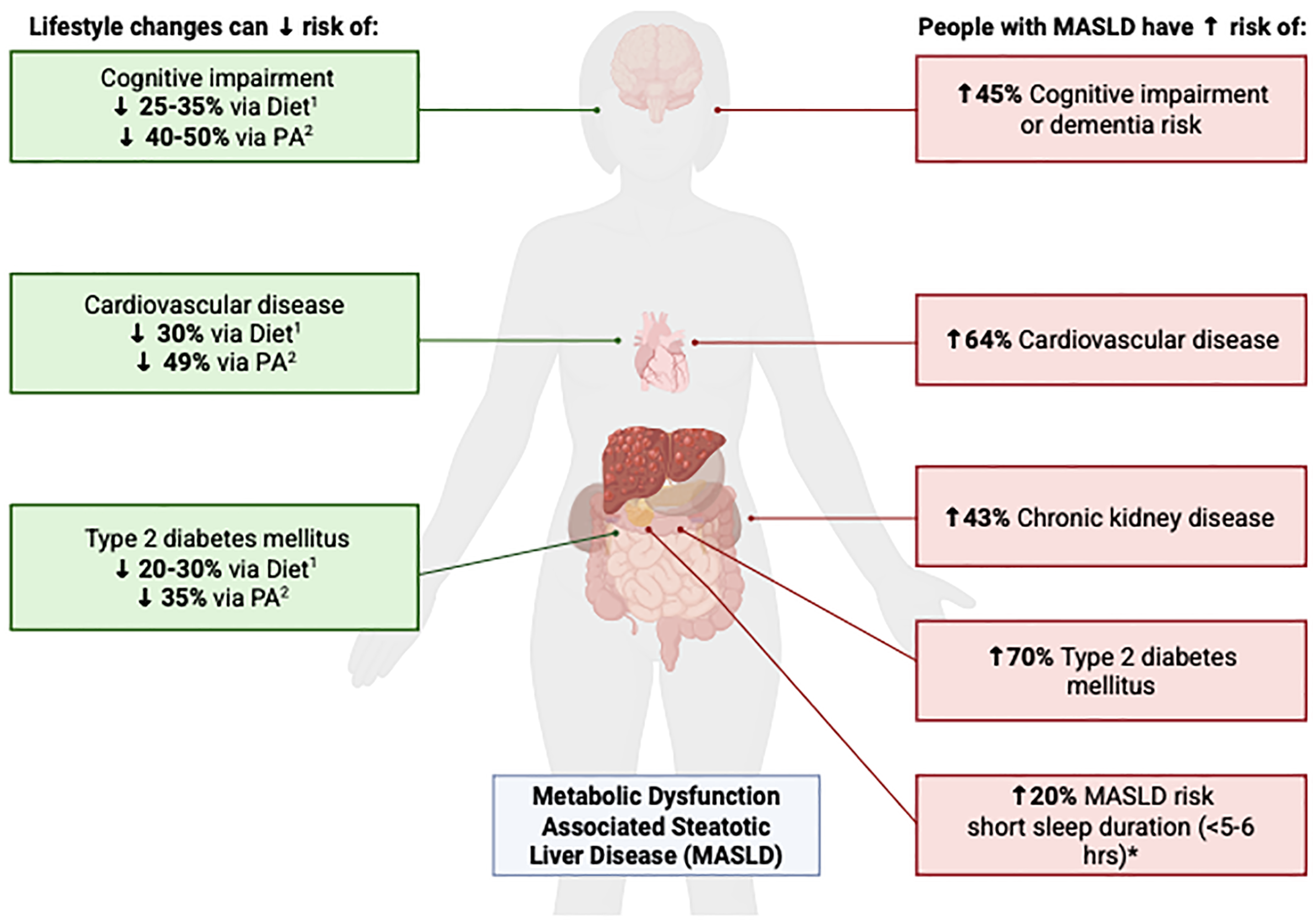
While lifestyle changes including diet, exercise and sleep independently show promising benefits for MASLD management both with and without weight loss, the synergistic effects of these lifestyle factors, targeted collectively using a multimodal approach, remain poorly understood. Integrated strategies are likely to lead to much greater and more sustainable improvements in metabolic health and quality of life compared to single modality interventions (Figure 1). From a 24hour behaviour perspective, time allocated to one behaviour inevitably affects the time available for others. As such, lifestyle interventions should account for the full spectrum of daily movement behaviours (i.e. PA, non-exercise activity thermogenesis (NEAT), sedentary time and sleep) alongside eating behaviours (including diet quality, quantity and timing) and substance related habits such as smoking and alcohol use. Although the interrelationships among these integrated lifestyle behaviours have not yet been established in MASLD (20), effective lifestyle management should remain mindful of each component and address them in a coordinated manner to optimise health outcomes(Reference Keating, Chawla and De67). Previous research has shown that the combination of holistic lifestyle factors may lead to enhanced health benefits and metabolic outcomes, as they address multiple risk factors simultaneously. The personalised approach helps to address individual’s needs and preferences, enhancing motivation and adherence, targeting the complex interplay between lifestyle behaviour and health outcomes and making it more sustainable(Reference Chan, Yu and Wong87). There is a paucity of evidence combining these approaches in MASLD and despite there being some evidence for multimodal approaches in associated chronic conditions these seldom embed approaches considering cultural appropriateness and safety.
Chronic disease risk in MASLD and risk reduction with diet and physical activity.

Figure 1. Long description
The diagram presents a human figure with various organs highlighted, including the brain, heart, liver, kidneys, and intestines. It shows how lifestyle changes, such as diet and physical activity, can reduce the risk of cognitive impairment, cardiovascular disease, and type 2 diabetes mellitus. The left side of the diagram indicates that diet can reduce cognitive impairment by twenty-five to thirty-five percentage, cardiovascular disease by thirty percentage, and type 2 diabetes mellitus by twenty to thirty percentage. Physical activity can reduce cognitive impairment by forty to fifty percentage, cardiovascular disease by forty-nine percentage, and type 2 diabetes mellitus by thirty-five percentage. The right side of the diagram highlights the increased risks for individuals with MASLD, including a forty-five percentage increase in cognitive impairment or dementia risk, a sixty-four percentage increase in cardiovascular disease, a forty-three percentage increase in chronic kidney disease, a seventy percentage increase in type 2 diabetes mellitus, and a twenty percentage increase in MASLD risk due to short sleep duration of less than five to six hours.
Sociocultural adaptations to enhance accessible and culturally responsive metabolic dysfunction-associated steatotic liver disease care
Culturally adapted evidence-based interventions are critically important for effective health-promotion programmes to address health disparities in culturally diverse populations. Research has shown culturally tailored approaches that consider language, religion and social norms can significantly improve participant engagement, adherence and health outcomes(Reference Livingstone, Love and Mathers88). However, to achieve successful cultural adaptation of interventions, it is essential to understand and prioritise the needs, values and preferences of the target group. Additionally, improving health literacy in CALD groups is an important step in supporting individuals to access and critically appraise health-related information that in turn would likely enhance adherence to lifestyle behaviours. Achieving the enhanced delivery of healthcare management and support to CALD communities starts with building trust with the target population and undertaking meaningful collaboration during the design, development, implementation and evaluation phases of lifestyle interventions(Reference Abdelbasset, Tantawy and Kamel89). Thus, co-design approaches are recognised as best practice for ensuring cultural relevance, improving acceptability and enhancing overall impact of lifestyle/health interventions(Reference Anderson, Gall, Butler and Ngampromwongse90,Reference Lederman, Moors-Mailei and Peacock91) . There are multiple ways to achieve effective cultural adaptation by tailoring interventions to suit the target audience.
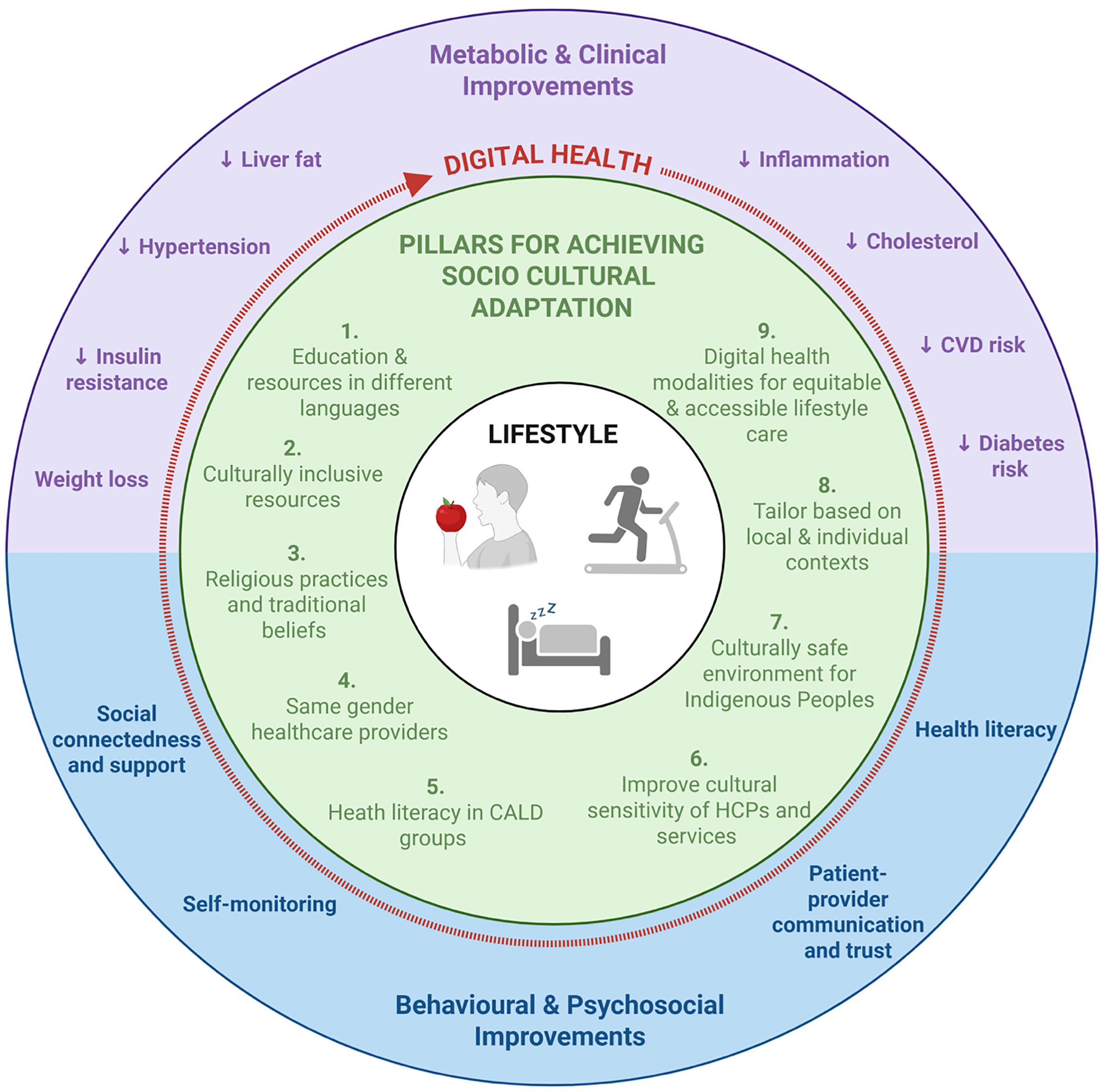
Nine pillars to achieve enhanced delivery of lifestyle interventions that are more culturally inclusive include (Figure 2):
The nine pillars for achieving socio cultural adaptations to enhance accessible and culturally responsive MASLD care with digital health indicated as an enabler and evidence surrounding the potential improvements in metabolic and clinical and behavioural and psychosocial outcomes.

Figure 2. Long description
The diagram presents nine pillars for achieving socio-cultural adaptation to enhance accessible and culturally responsive care for metabolic dysfunction-associated steatotic liver disease (MASLD) using digital health as an enabler. The pillars include education and resources in different languages, culturally inclusive resources, religious practices and traditional beliefs, same-gender healthcare providers, health literacy in culturally and linguistically diverse (CALD) groups, improving cultural sensitivity of healthcare providers and services, culturally safe environments for Indigenous Peoples, tailoring based on local and individual contexts, and digital health modalities for equitable and accessible lifestyle care. The diagram also highlights potential improvements in metabolic and clinical outcomes such as reduced liver fat, inflammation, cholesterol, cardiovascular disease risk, and diabetes risk, as well as behavioral and psychosocial improvements including weight loss, insulin resistance, hypertension, social connectedness and support, self-monitoring, health literacy, and patient-provider communication and trust.
-
1. Education and resources in different languages
Provision of counselling and educational materials in multiple languages, targeted to the communities they are intended to serve, has been shown to reduce communication barriers and support informed decision making. Research highlights that health materials/resources in different languages improve participant engagement, comprehension and retention of health advice, specifically in diverse or migrant populations(Reference Khatri and Assefa57). Translation is not a linear process and often requires many steps including forward and backwards translation techniques followed by reviews by the target populations to ensure information is not ‘lost in translation’ and is culturally appropriate. Despite the challenges and cost associated with providing multilingual resources the provision of this information is critical. In a scoping review, multilingual health resources in lifestyle intervention programmes for prevention of chronic diseases was associated with higher attendance and adherence, as well as increased knowledge of diseases and healthcare among non-English speaking study participants(Reference Joo and Liu92). In addition, translated education resources/materials either in hardcopy or online that take into consideration cultural aspects as well as language translation are more effective than translation alone in promoting behaviour change in participants(Reference Andrulis and Brach93). Another review on behavioural weight loss interventions in African American women including culturally adapted strategies such as culturally reflective images, languages, beliefs, values and social norms around food and body images, reported more engaged participants and improvements in weight and diet-related outcomes(Reference Kong, Tussing-Humphreys and Odoms-Young94).
-
2. Culturally inclusive resources
To increase the equity and accessibility of health and lifestyle care, healthcare providers should conduct a local needs analysis to understand the cultural composition and specific barriers, use multilingual and visual resources to improve communication and engagement and partner and build trust with community leaders and multicultural health services to co-design culturally aware and sensitive programmes.
-
3. Religious practices and traditional/cultural behaviours and beliefs
It is critical to ensure cultural safety by respecting sex norms, religious practices and traditional health beliefs. The consideration of cultural and religious practices, such as fasting periods (e.g. Ramadan, Christianity) and Vegetarianism in religions such as Hinduism and Buddhism are just as important to increase adherence and improve personalised nutrition management during interventions. Respecting these practices can help individuals follow tailored medical nutrition advice. Islamic Ramadan fasting involves abstaining from food and drink from dawn to sunset for 29-30 days. Food is consumed typically just before sunrise (Suhoor), and the fast is broken at sunset (Iftar). The median duration of fasting usually lasts between 14 to 15 hours, depending on geographical location, with some regions reaching up to 20 hours. No food, drinks including water, or substances are to be consumed during the fasting period. Ramadan fasting has been linked to benefit metabolic health in healthy individuals and also people with T2D(Reference Aydın, Kul and Karadağ95). Studies note that improvements in metabolic markers including enhanced insulin sensitivity, reduction in body weight and improved fat metabolism as these practices may effect circadian and sleep patterns(Reference Kul, Savaş and Öztürk96). Evidence suggests favourable lipid profiles and reduced inflammation in individuals with T2D with Ramadan fasting(Reference Trabelsi, Ammar and Boujelbane97). Dietary advice should align with traditional Ramadan eating patterns, emphasising nutrient-dense meals at sunset and before dawn, while also highlighting the importance of adequate hydration during non-fasting hours.
Another common type of fasting involves Christian Orthodox fasting which is a long-term dietary practice that involves abstaining from meat, dairy and eggs for approximately 180–200 days annually with increased consumption of fruits, vegetables, whole grains and fish and seafood(Reference Sarri, Kafatos and Higgins98). Christian Orthodox fasting has been closely linked with the Mediterranean lifestyle/diet and associated with improved lipid profiles, reduced body weight and blood pressure and improvements in metabolic health outcomes(Reference Koufakis, Karras and Antonopoulou99). Although concerns about nutrient deficiencies are reported specifically with vitamin B12, vitamin D and Ca. Lifestyle and dietary interventions should provide practical guidance on nutrient-rich, plant-based meal planning during the fasting times and recognise the nature of fasting (what they are abstaining from) to support health goals during and outside of fasting periods(Reference Koufakis, Karras and Antonopoulou99).
-
4. Same-sex healthcare providers
Literature supports the provision of same-sex healthcare providers, meaning the healthcare provider is the same sex as the patient, as a key factor in improving patient comfort, and cultural and or religious appropriateness, particularly within Indigenous populations. Studies have shown that Indigenous patients often face significant health inequalities leading to lower life expectancy and higher rates of chronic diseases(Reference Li100). Indigenous people often feel uncomfortable with healthcare providers who do not share the same sex or cultural background. Strengthening the cultural barriers by adopting respectful practices such as same-sex healthcare providers may help reduce inequities(Reference Lowell101). This practice is associated with open communication and higher satisfaction of care. These practices have been shown to emphasise respect for patients’ cultural identities, including reducing barriers to accessing healthcare and improvement engagement(Reference Mobula, Okoye and Boulware102). Including same-sex healthcare options aligns culturally responsive and patient-centre care to enhance health outcomes(Reference Mobula, Okoye and Boulware102).
-
5. Improving health literacy in CALD groups
A more complex set of skills, known as health literacy, is among one of the key determinants for successful lifestyle modifications(Reference Farley103) Health literacy is defined as “the individual’s capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions”(Reference Sørensen, Van den Broucke and Fullam104). Comprehensive health literacy extends beyond the skills of being able to read and comprehend health information, to also include the skills and resources needed to appraise information, access health services and engage with healthcare providers(Reference Beauchamp, Talevski and Nicholls105). Health literacy levels are often lower in CALD groups compared with the general population(Reference Khatri and Assefa57,Reference Tørris and Nortvedt106) This may stem from language barriers, limited access to culturally appropriate health information, differences in health beliefs and socio-economic factors (93). Low health literacy is associated with low awareness of disease risk factors and prevention strategies, difficulty navigating the complex healthcare system, evaluating the reliability of health information and adhering to medical advice(Reference Adams, Appleton and Hill107,Reference Jayasinghe, Harris and Parker108) . Collectively, these factors directly and indirectly contribute to poor MASLD management associated with adverse health outcomes(Reference Figueroa, Castañeda and McLean109–Reference Al Hussein Al Awamlh, Moses and Whitman111). Translating health information/materials to multiple languages, using infographics and avoiding jargon medical terms could aid in understanding the health-related information (98). Providing interpreters, bilingual staff and patient navigators facilitates navigating the healthcare system(Reference Mistry, Harris and Li112).Training health professionals in cultural competencies to support people with diverse backgrounds. Making reliable health information digitally accessible in various languages to people with various literacy levels would help increasing the health literacy in CALD groups.
-
6. Enhance cultural safety and cultural responsiveness of healthcare professionals and services
Training HCP, including dietitians and exercise professionals, in cultural responsiveness and inclusive communication strategies is essential to improving equitable access to care. Current considerations surrounding cultural safety include addressing the need for more enhanced effort, but there remains substantial variation in both the delivery and level of competence among clinicians and graduates(Reference McMillan113). Structural disadvantages within the healthcare system due to racism, dispossession from country and dislocation from family and kinship, as well as limited numbers of multilingual or Indigenous health professionals, and insufficient multilingual resources continue to impede cultural safety and restrict culturally responsive care(Reference Khatri and Assefa57).
-
7. Cultural safety when working in partnership with Indigenous peoples
Genuine and meaningful partnerships with Indigenous-led services as well as supporting organisations such as in health and education, will empower culturally safe and culturally responsive care. These partnerships will extend the reach and impact of community engagement initiatives and address barriers to participation. Centring the inclusion of Indigenous Community Health Workers, HCP and Liaison Officers, creating a non-judgemental space, offering culturally safe resources, using plain language and avoiding medical jargon is also important(Reference Elvidge, Taylor and Harvey114). Additionally, culturally safe clinic and environmental activation is fundamental whereby the consultation space must be culturally welcoming (e.g. artwork displayed prominently).
HCP should practice deep listening and privilege the voices of family/community/Elders through storey telling, ensuring the client and their community are central to decisions (e.g. respect diverse ways of expressing health concerns). The importance of practitioners considering and reflecting on one’s own personal biases as HCP, cultural assumptions and power through multiple levels will recognise the long history of atrocities and genocide enacted on Indigenous peoples through healthcare. A holistic approach to health which involves physical, social, emotional and spiritual aspects should be upheld in line with strengths-based Cultural Determinants of Health. HCP should be reflexive, seek feedback and continue to learn more about culturally safe and culturally responsive health for Indigenous peoples.
-
8. Personalised and local contexts
Consistent with the principles of optimal, evidence-based dietary patterns that elicit enhanced health benefits such as the MedDiet, personalised dietary models can be tailored to replicate components and key features of the diets including nutrients, foods, as well as cuisine, biodiversity and sustainability(Reference George, Kucianski and Mayr41). This adaptation can be achieved in line with an individual’s social and cultural preferences, needs, their food environment and financial resources, but often requires the support of a dietitian or HCP with significant expertise in diet and disease. Tailoring of the MedDiet and culturally appropriate substitutions from other traditional diets while maintaining core cultural foods has been shown to be feasible to enhance inclusivity, however these approaches to adaptation are seldom applied in interventions and less so in practice(Reference Bourne, Gill and Cooley115).
-
9. Leveraging digital health modalities to enhance equitable and accessible lifestyle care
Those from CALD and those who face language barriers may experience even greater challenges engaging with lifestyle programmes(Reference Hallsworth, McPherson and Anstee116). In the digital era, web-based lifestyle interventions have emerged as scalable, accessible and personalised tools for the management of MASLD. Digital innovation may enable more equitable care to high-priority populations including CALD, regional and remote communities, Aboriginal and Torres Strait Islander peoples and low socio-economic groups. Importantly, digital health innovations can be tailored to meet specific needs of CALD groups through language translation, cultural adaptations to diet through recipes and cooking practices, improving health literacy and flexibility(Reference Naderbagi, Loblay and Zahed117). This cultural adaptability can help enhance engagement, adherence reducing health disparities in all chronic diseases as well as MASLD(Reference Katz, Mszar and Grimshaw118). Digital interventions can help overcome barriers to accessing multidisciplinary healthcare teams, particularly in resource-limited settings such as rural, regional and remote communities and among individuals with special needs. On-demand platforms and mobile applications enhance convenience and access and provide interactive features along with tailored recommendations that support user engagement and increase motivation to lifestyle changes(Reference Avery, Smith and Livingston119). Digital health interventions/platforms can therefore improve accessibility by overcoming geographical barriers, enabling language translation and reducing participant burden for travel and time. There are also more broad reaching benefits that digital health supports such as self-paced learning in the comfort of one’s own home or chosed environment, overcoming time zone barriers and enabling real-time tracking, data collection, reminders and nudging(Reference Borges do Nascimento, Abdulazeem and Vasanthan120). Digital health interventions can also provide lifestyle counselling including education and support through websites, internet-based, mobile applications, SMS or videos have been increasingly popular for weight management(Reference Lyzwinski121,Reference Levine, Savarimuthu and Squires122) . Conversely the poor quality of internet connection especially in rural and remote locations, potential disconnect with HCP, lack of literacy surrounding technology and social isolation present barriers for digital health(Reference Maita, Maniaci and Haider123). However to date the limited evidence specifically in people with MASLD, comparing digital lifestyle interventions with traditional lifestyle approaches reported significant improvements in liver enzyme levels and body composition parameters, including weight loss, highlights that further investigation is warranted(Reference Zafar, Sohail and Saad124).
Achieving culturally inclusive lifestyle management efficiently
A substantial body of established interventions are already available for the management of chronic conditions, including CVD and T2D. Embedding cultural considerations need not entail the development of novel interventions or strategies. Rather, an efficient and methodologically robust approach is to employ evidence-based frameworks to adapt existing interventions, thereby preserving their demonstrated efficacy while enhancing cultural relevance, acceptability and implementation fidelity across diverse populations(Reference Movsisyan, Arnold and Copeland125,Reference Thier, Martinez and Alresheed126) . These frameworks commonly follow a structured process and engage stakeholders to guide decisions on what to adapt, when and how(Reference Movsisyan, Arnold and Copeland125). Adaptions may target the intervention content, delivery method or the broader context, while cultural adaptation specifically aims to preserve the intervention’s relevance across different populations. Previous studies have applied adaptation frameworks to guide intervention modifications. For example, Goode et al(Reference Goode, Owen and Reeves127) adapted a telephone-delivered PA and dietary behaviour change intervention into community practice which highlighted the importance of adapting delivery methods and materials to local resources and involve the community to respond to real-time barriers ensuring to meet the needs(Reference Goode, Owen and Reeves127). Research indicates effective adaptation of interventions relies on partnerships/collaborations between community and researchers to make evidence-based and culturally appropriate changes. However, their application for lifestyle interventions is limited and there is an opportunity to enhance cultural responsiveness of the many existing lifestyle interventions available for chronic disease management and particularly in MASLD where lifestyle is the most critical and in many countries, the only, evidence-based strategy available(Reference Sørensen, Van den Broucke and Fullam104).
Conclusion: the future of lifestyle management for metabolic dysfunction-associated steatotic liver disease
Given the global rising burden of MASLD and association with other metabolic conditions, the importance of scalable multimodal lifestyle interventions has become crucial for improving outcomes and preventing disease progression at the population level(Reference Kravchuk, Bychkov and Kozyk28). A holistic, multimodal and individually tailored lifestyle approach – encompassing dietary modification, PA, sleep and behaviour change strategies calibrated to individual capacity and preferences – should be provided to people with MASLD. Central to the effectiveness and scalability of such care is the systematic incorporation of cultural adaptation, ensuring that goals, messages and delivery modalities align with patients’ cultural values, preferences, health beliefs and social contexts. In parallel, increasing awareness, educating those with established disease, enhancing patient – provider communication and guaranteeing equitable access to evidence-based information should be embedded within healthcare systems. By integrating culturally adapted interventions across these domains, health services are more likely to achieve sustained engagement, improve clinical outcomes and reduce the global clinical and economic burden associated with MASLD. Future research should consider co-designed approaches and to evaluate effectiveness and implementation of accessible, personalised, digitalised interventions which are multimodal (e.g. include both diet and exercise) and culturally responsive that best meet the diverse needs and preferences of people with and/or at risk of MASLD.
Acknowledgements
The authors acknowledge the Traditional Custodians of the land and waters which they share. The authors pay respect to Elders past, present and emerging. This review was prepared by non-Indigenous scholars (ESG, SS, AS, SC, SKR, RMD, S-YT, DS and JG SEK) and a Ngarabal scholar. KW wrote the section about Indigenous peoples and cultural practices and recommendations.
Author contributions
ESG, SS, AS and SEK contributed to the conceptualisation and structure of the review. ESG, SS, AS and SEK drafted the initial manuscript. ESG and SS created the figures and tables. ESG supervised the review. All authors contributed to reviewing, editing and writing the final manuscript.
Financial support
Shelley E Keating is supported by an NHMRC Investigator Grant (2042446)
JG is supported by the Robert W. Storr Bequest to the Sydney Medical Foundation, University of Sydney; Investigator and MRFF grants (APP2032407; NCRI000183; APP2016215; APP 2010795; APP1196492)
SC is supported by a Monash Partners and Equity Trustees STAR Fellowship Program 2025
Competing interests
The author(s) declare none.

 Open access
Open access