


Military veterans, defined as ex-serving members of the Armed Forces, are a population with unique health needs(Reference Oster, Morello and Venning1). Upon entry to service, initial medical screening ensures military recruits have higher overall health and fitness levels than the general population. However, the training and retention standards required for military readiness(Reference Haibach, Haibach and Hall2), coupled with the demands of military life, can lead to chronic physical and mental health issues(Reference Ross, Prguda and Setchell3). For example, exposure to physical and psychological trauma is associated with an increased risk of depression, anxiety, post-traumatic stress disorder(Reference Ross, Prguda and Setchell3) and chronic pain for veterans. Upon transition from service to civilian life, veterans often experience a significant decline in health, characterised by complex and persistent healthcare needs and requirements(Reference Haibach, Haibach and Hall2,Reference Ross, Prguda and Setchell3) , and challenges relating to employment and injuries obtained during their military service(Reference Dexter4). In addition, life outside service requires adaptation(Reference Lake and Armstrong5), with lifestyle factors, such as diet, exercise and sleep patterns, often changing dramatically(Reference Ligotti6,Reference Fisher, Ledford and Wollney7) . Access to appropriate care, opioid misuse and elevated suicide rates within veteran populations further exacerbate these challenges, necessitating innovative solutions(Reference Ross, Prguda and Setchell3,Reference Sayre, Neely and Simons8,Reference Carroll, Kearney and Miller9) for veteran health.
Diet quality and eating habits are known to play an important role in overall health and well-being, with poor diets shown to negatively impact health, functional independence and disease risk(Reference Browne, Morey and Beckham10,Reference Lee11) . A recent international review of dietary intake in active military personnel found high consumption of added sugars, trans fats and processed meat among defence members(Reference Bayes, Burch and Lauche12). Consumption of these foods has been linked to a number of diseases, including obesity(13), CVD and diabetes(Reference Bonaccio, Di Castelnuovo and Costanzo14). Emerging evidence in Nutritional Psychiatry also underscores the critical role of diet in mental health(Reference Bayes, Schloss and Sibbritt15–Reference Lee, Orr and Marx17). Research conducted with US veterans demonstrates that healthy eating is associated with reduced symptoms of major depressive disorder and suicide ideation(Reference Oakey-Frost, Trachik and Ganulin18). Similarly, a cross-sectional study from Iran showed a strong relationship between high scores on the Alternative Healthy Eating Index and decreased odds of developing depression and anxiety(Reference Hoerster, Wilson and Nelson19). Given the unique stressors of military life and the elevated risk of mental health conditions in veterans, understanding nutritional intake and diet quality as a modifiable lifestyle factor to promote health is paramount.
Nutrient reference values (NRV) are required to assess the adequacy and safety of nutrient intakes for population groups. They indicate the daily amount of nutrients (energy, macro-nutrients, vitamins and minerals) as a benchmark estimate for broad population-level health. Various sets of reference values have been developed, expanded and updated for international, regional or national use(Reference Lewis and Dwyer20). NRV also provide a scientific basis for baseline standards and regulations to improve public health, optimise and preserve healthy functioning relevant to age and sex. Some countries have not established their own nutrient intake recommendations; instead, they have adopted and modified those from other international sources appropriate to their situation(Reference Lewis and Dwyer20). NRV can also differ in estimates of various nutrients, relative to age, sex and health requirements (e.g. pregnancy and lactation). The WHO and the FAO of the UN have published comprehensive global recommended nutrient intakes(21).
To date, there has been no clear systemic evaluation and application of NRV for veteran populations. This is crucial for identifying specific nutritional profiles of adequate and inadequate intakes to promote dietary and health interventions that are effective, policies that are well-informed and future research that addresses critical areas such as potential deficiencies or excesses that may contribute to the development of chronic disease and mental health disorders. Therefore, we sought to identify dietary components where veteran populations exhibit the greatest variation from recommended nutrient intake and synthesise reported impacts on health outcomes. This systematic review of results is intended to guide the development of targeted dietary interventions and educational materials for policymakers and veteran health organisations.
Our primary aim is to synthesise the dietary intake, composition and diet quality of military populations and compare intakes relative to NRV for individual nutrients. Our secondary aim is to assess the frequency of food consumption (e.g. number of servings of vegetables consumed per day) and identify nutrient excesses or deficiencies compared to the daily recommended values and other health-related and co-occurring conditions reported such as BMI, health behaviours (i.e. smoking) and mental health.
Methods
Data source and search strategies
A protocol was developed according to the Preferred Reporting Items For Systematic Reviews And Meta-Analysis Protocols (PRISMA-P) 2020 statement(Reference Page, McKenzie and Bossuyt22) (online Supplementary Material). The review was registered with the International Prospective Register of Systematic Reviews, PROSPERO (Registration ID: CRD42024500252).
A literature search was conducted by the lead researcher (JB) in conjunction with librarians in the following databases: CINAHL, MedLine, Scopus (Elsevier), PubMed and AMED. A combination of Medical Subject Headings (MeSH) and free terms was used with Boolean operators integrated for advanced searches. The search used a combination of two search strings: the first one using terms for diet and nutrition and the second one using terms for military veterans. The full search strings for all databases are provided in the online Supplementary Material. The following key search terms are an example of the search in PubMed, with the terms adapted for each database:
(Diet [MeSH] OR Diet, Food, and Nutrition [MeSH] OR Diet Quality OR Diet Intake OR Nutrition Assessment [MeSH] OR Nutrients [MeSH] Nutrient Intake OR Nutritional Status OR Nutrition OR Dietary Intake OR Food Access) AND (Veterans [Mesh] OR Veterans Health [Mesh] OR Veterans Wellbeing OR Veteran Lifestyle).
Screening of grey literature such as government reports/websites and clinical practice guidelines was also performed, along with hand-searching the reference list of the included articles. Studies identified through database searching were exported and stored in EndNote X9(23). Articles were then imported into Covidence(24) where they were screened by title and abstract first and later assessed as full text by JB and ML. The initial database search was performed by JB and final full-text articles reviewed by ML, until inclusion consensus was reached.
Inclusion and exclusion criteria
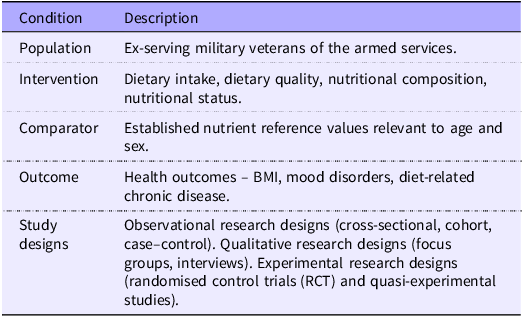
Original research published up to 19 January 2024, which assessed usual dietary intake, quality or composition, or nutritional status in military veterans, was included in the review. An additional time-span-specific search was conducted on 17 March 2025 to assess for any additional articles published since the original search date. Studies which met all PICOS criteria were included (Table 1). All research designs were deemed eligible, including observational research designs (cross-sectional, cohort and case–control) and qualitative research designs (focus groups, interviews, etc). Experimental research designs (randomised control trials (RCT) and quasi-experimental studies) were included only when dietary intake or nutrition status data were reported at baseline or for the control group.
PICOS criteria for inclusion and exclusion of studies

Articles were excluded from the review if they constituted literature reviews, were duplicate studies, conference proceedings, commentaries, abstracts, short communications and letters to the editor or reported findings from animal model research, in vivo and in vitro research.
Risk of bias assessment
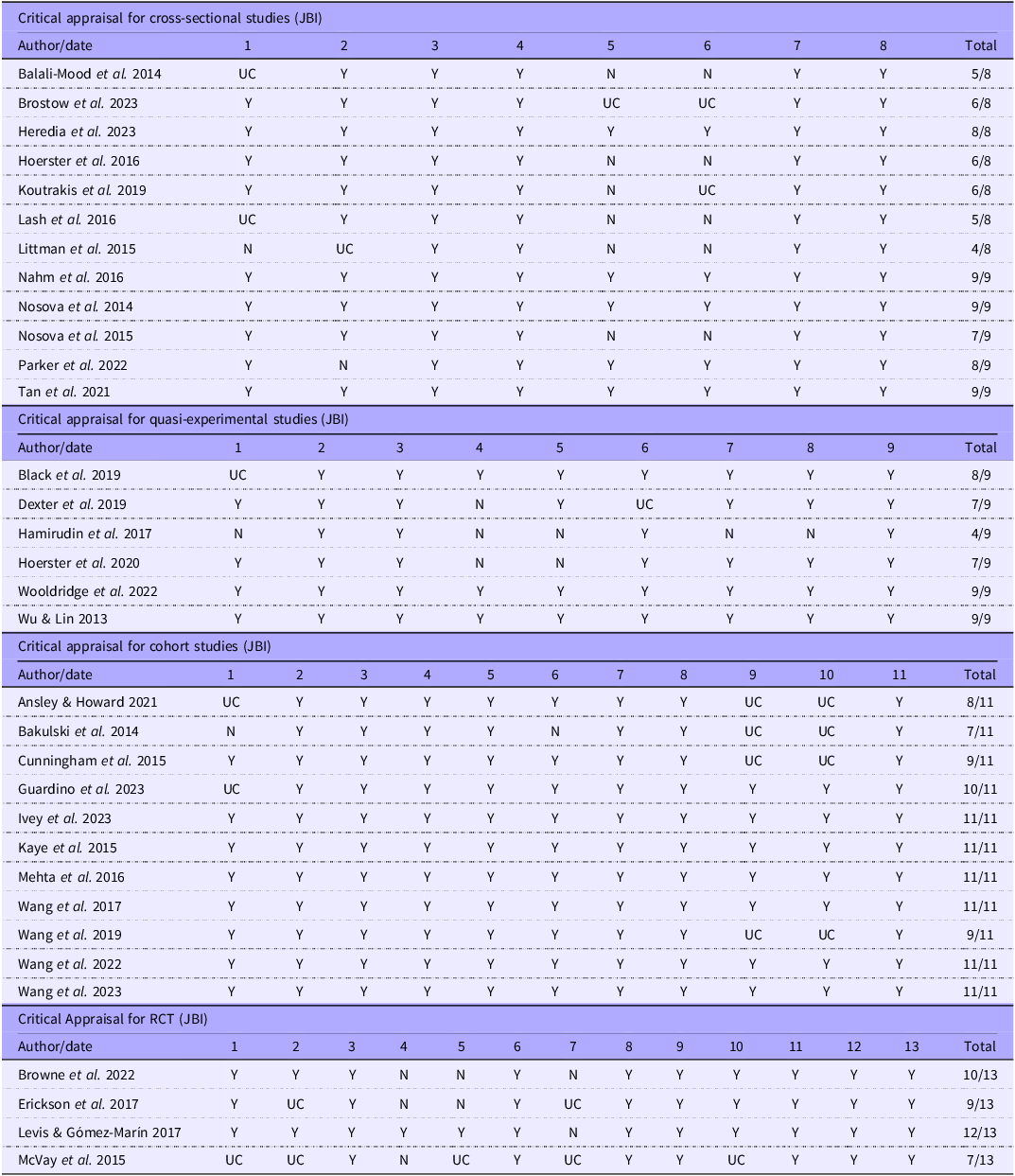
Each paper was critically appraised for methodological consistency using the Joanna Briggs Institute (JBI) critical appraisal checklists(Reference Tufanaru, Munn and Aromataris25) for cross-sectional, cohort, RCT and quasi-experimental studies. The checklist for cross-sectional studies includes eight questions which evaluate inclusion and exclusion criteria, study setting, measurement reliability, confounding factors and statistical analysis. A score of 0–3 was considered as high risk of bias, a score of 4–5 was considered as medium risk of bias and a score of 6–8 was considered as low risk of bias. The checklist for quasi-experimental studies includes nine questions which assess the clarity of ‘cause’ and ‘effect’ variables, comparisons/control group similarity, measurement reliability, follow-up and statistical analysis. A score of 1–3 was considered as high risk of bias, a score of 4–6 was considered as medium risk of bias and a score of 7–9 was considered as low risk of bias. The checklist for cohort studies includes eleven questions which evaluate similarity between groups, measurement reliability, confounding factors, follow-up and statistical analysis. A score of 0–3 was considered as high risk of bias, a score of 4–7 was considered as medium risk of bias and a score of 8–11 was considered as low risk of bias. The checklist for RCT includes thirteen questions which evaluate randomisation method, blinding, measurement reliability, follow-up and statistical analysis. A score of 0–4 was considered as high risk of bias, a score of 5–9 was considered as medium risk of bias and a score of 10–13 was considered as low risk of bias. Risk of bias was assessed by JB and reviewed by ML, and disagreements were resolved through discussion. Table 2 displays the results from the critical appraisal.
Joanna Briggs Institute risk of bias critical appraisal results

Y, yes; N, no; UC, unclear/can’t tell; N/A, not applicable.
Data extraction
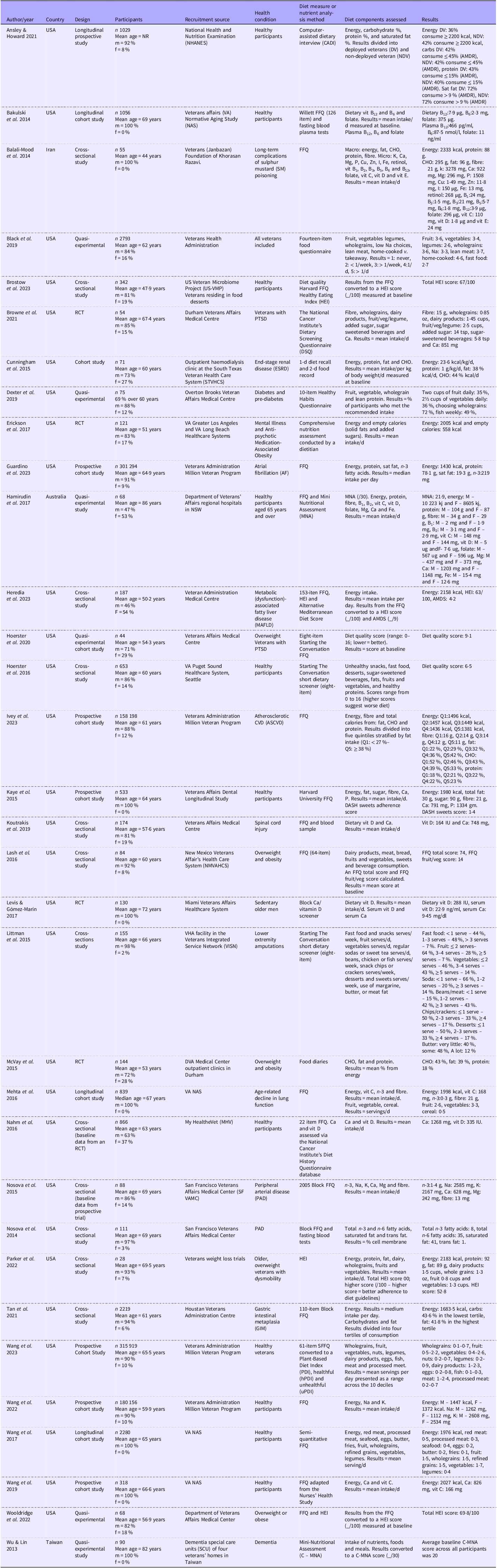
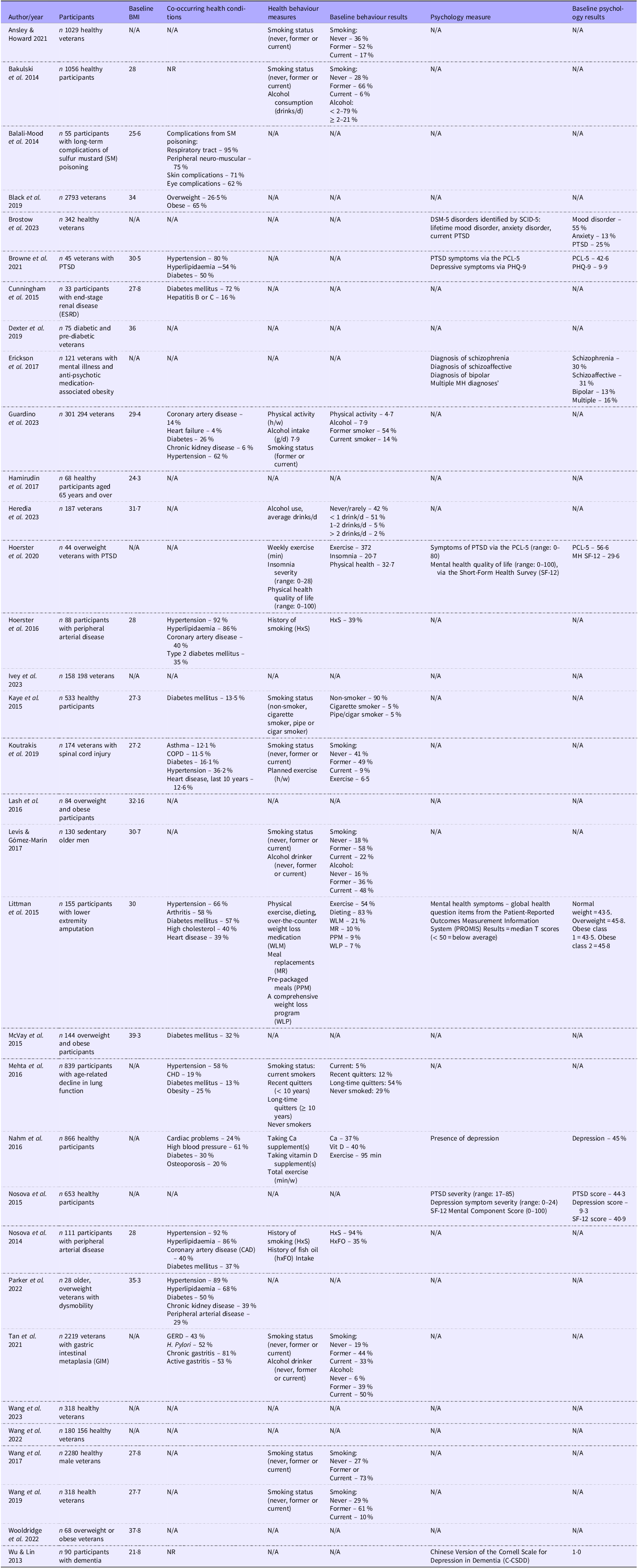
Predetermined data extraction included the following components: (i) general review information (title, authors and year of publication), (ii) methods of the study (study design, number of participants, location, setting and recruitment sources), (iii) participants (age, sex, health condition if applicable and co-morbidities); (iv) diet measure or nutrition analysis measure and (v) data and results. The extracted data from the final articles are summarised in Table 3. Additional secondary outcomes were also extracted. These included (i) BMI, (ii) co-occurring health conditions, (iii) health behaviours (behaviour measurement tools and results) and (iv) mental health (mental health measurement tools and results). The extracted secondary outcomes are summarised in Table 4. The first author (JB) extracted data from the final cohort of studies, including age, sex, service type, country of study origin, year of publication, study design and any baseline and post-treatment outcome data related to nutritional intake (means, mean differences and standard deviations). The second author (ML) checked the data extraction, and the third author reviewed (TB).
Study characteristics data extraction table

NR, not reported; m, male; F, female; AMDR, Aacceptable Macronutrient Distribution Range, CHO, carbohydrate; RCT, randomised control trial; PTSD, post-traumatic stress disorder; AMDS, Alternate Mediterranean Diet Score; DASH, Dietary Approaches to Stop Hypertension; IU, International Units.
*HEI scores: > 80 = good diet, scores 51–80 = fair diet, requires improvement, and scores < 51 = a poor diet.
Participants’ health characteristics

N/A, not applicable; NR, not reported; DSM-5, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; SCID-5, Structured Clinical Interview for DSM-5; PTSD, post-traumatic stress disorder; PCL-5, Posttraumatic Stress Disorder Checklist; MH, mental health; COPD, chronic obstructive pulmonary disease, GERD, gastroesophageal reflux disease.
Analysis
A critical two-step process was undertaken. First, diet and health data were extracted from the articles and presented in Table 3 and Table 4. Second, a direct synthesis and appraisal/comparison of the extracted data were assessed against the NRV for their age, sex and country and/or diet quality scores where available. The decision to use country-specific NRV was made to ensure that veterans’ intakes were evaluated against the most geographically relevant standards established by their own national health authorities. A comparison table of the different NRV used can be found in the online Supplementary Material. National NRV often account for regional differences in soil mineral content, food fortification policies and population-specific health risks. To maintain consistency where national guidelines were unavailable, international standards from the WHO were applied. These key analytical findings are presented in Table 5.
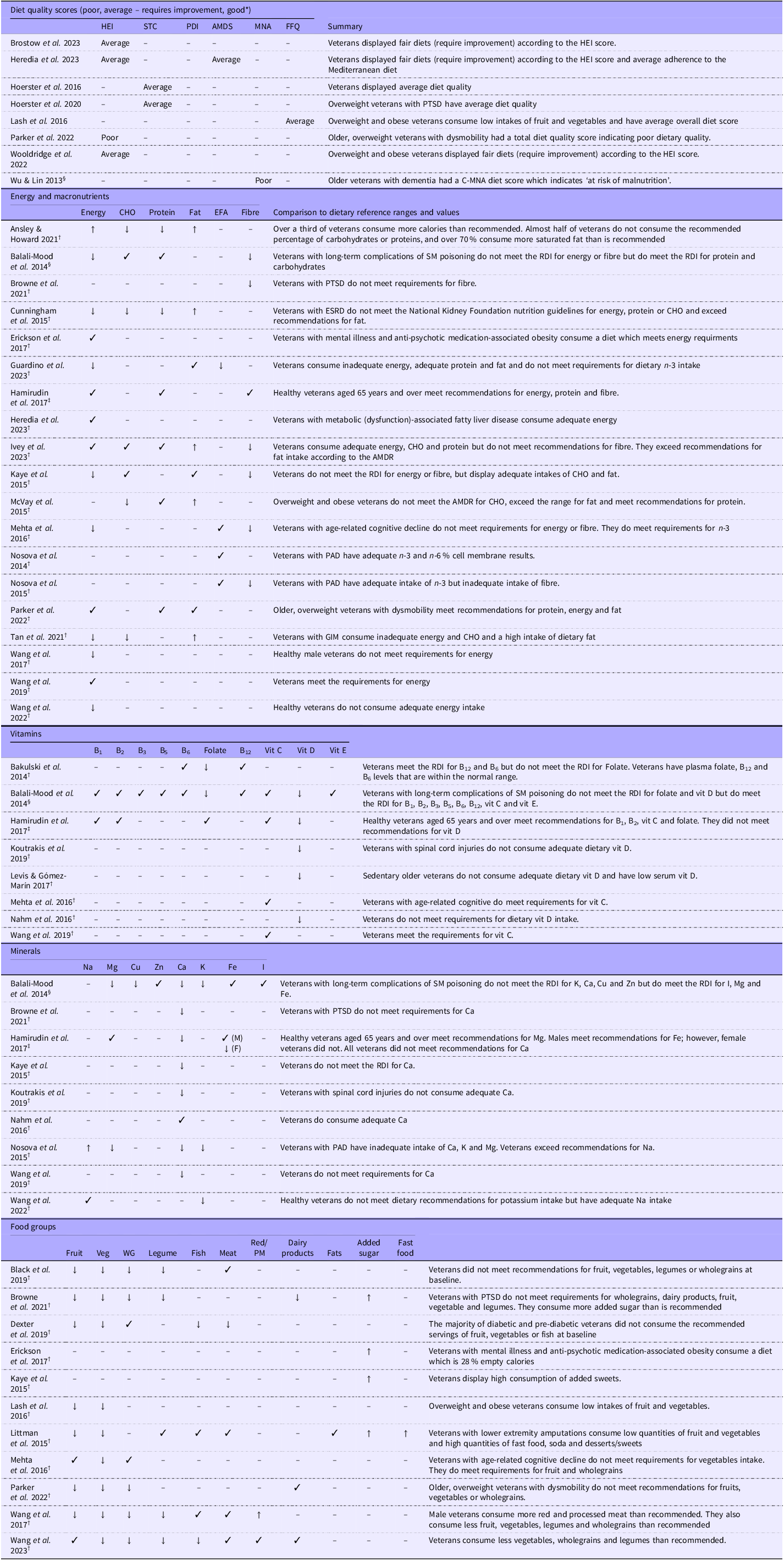
Reported dietary quality and nutrient reference range analysis and comparison

HEI, Healthy Eating Index; PDI, Plant-Based Diet Index; AMDS, Alternate Mediterranean Diet Score; MNA, Mini-Nutritional Assessment; PTSD, post-traumatic stress disorder; M, male; F, female; CHO, carbohydrate; EFA, essential fatty acids; SM, sulfur mustard; ESRD, end-stage renal disease; AMDR, Acceptable Macronutrient Distribution Range; PAD, peripheral artery disease; GIM, gastric intestinal metaplasia; WG, wholegrains; PM, processed meat; NRV, nutrient reference values.
*Diet quality scores divided into: poor, average/fair – requires improvement, or good – based on the criteria for each tool.
↓ = Does not meet dietary reference ranges (for the population age/sex).
✓ = Does meet dietary reference ranges (for the population age/sex).
↑ = Exceeds recommended dietary intake (for the population age/sex).
– = Not assessed.
NRV sources.
†Studies conducted in the USA (n 30) compared against USDA Dietary Guidelines.
‡Studies conducted in Australia (n 1) compared against NHMRC NRV.
§Studies conducted in Iran (n 1) and Taiwan (n 1) compared against WHO guidelines.
Results
Identification of studies/study selection
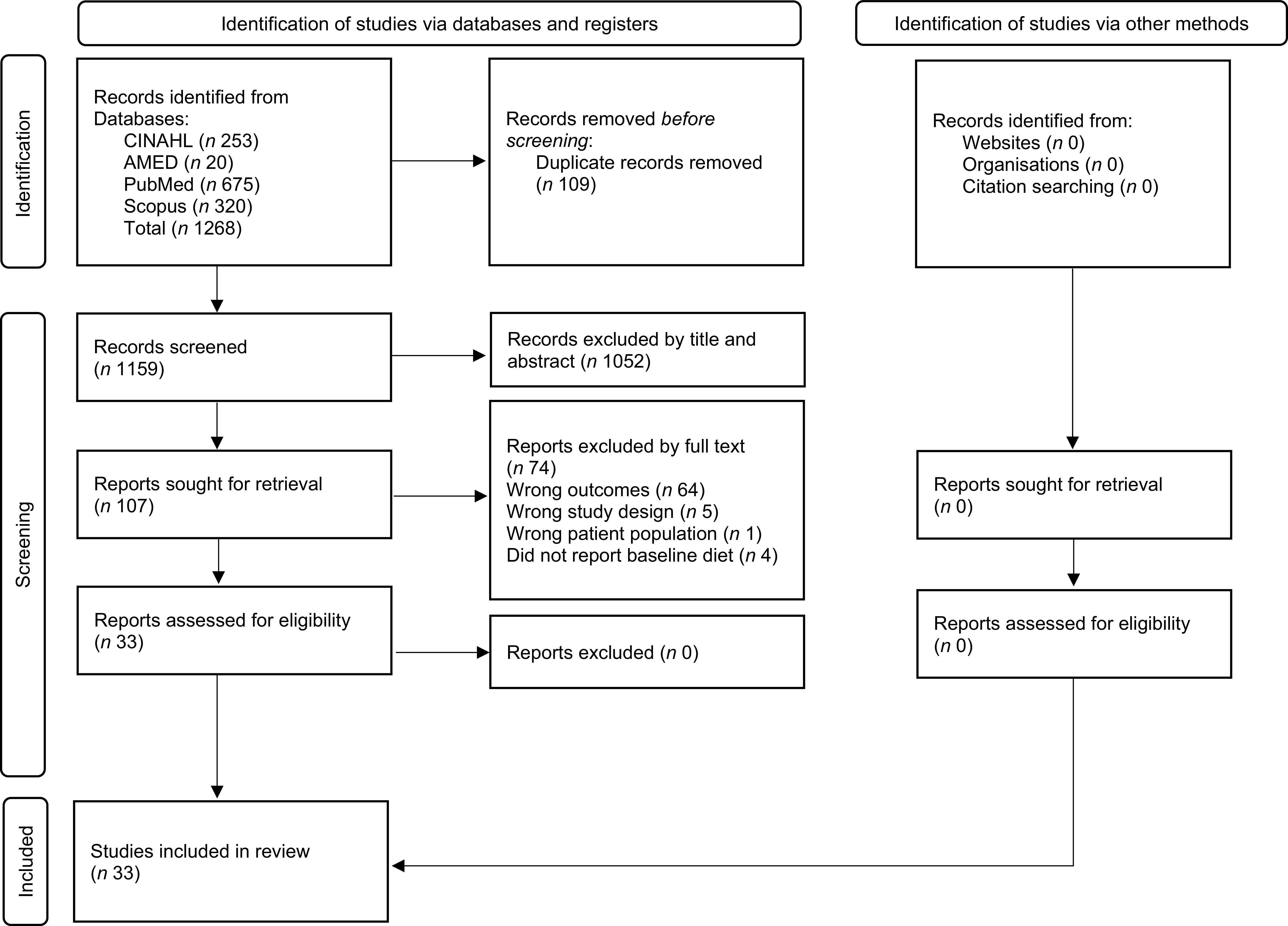
The initial search identified 1268 papers; see Figure 1. After the removal of 109 duplicates, articles were screened by title and abstract. A total of 107 articles were then screened by full text, resulting in thirty-three articles which met the full inclusion criteria. The list of articles excluded at the full text stage, along with reasons for exclusion, can be found in the online Supplementary Material.
Prisma flow diagram.

Critical appraisal results
Table 2 displays the risk of bias score for each included article. For the cross-sectional studies (n 12), the majority had a low risk of bias (n 9)(Reference Hoerster, Wilson and Nelson19,Reference Nosova, Chong and Alley26–Reference Heredia, Thrift and Ramsey33) or a medium risk of bias (n 3)(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34–Reference Nahm, Charters and Yoo36), with no studies displaying a possible high risk of bias. The main issues observed included a lack of clarity in defining the sample inclusion criteria, inadequate identification of potential confounding factors and the absence of reported strategies to address these confounding factors. None of the cohort studies (n 11) had a high risk of bias, one had a medium risk of bias(Reference Cunningham, Verkaik and Gross37) and ten had a low risk of bias(Reference Bakulski, Park and Weisskopf38–Reference Wang, Li and Nguyen47). Issues identified in the cohort studies was the lack of information regarding reasons for loss to follow-up. Additionally, strategies to address incomplete follow-up data were not reported. For the four RCT, one had a medium risk of bias(Reference Erickson, Kwan and Gelberg48) and three had a low risk of bias(Reference Browne, Morey and Beckham10,Reference McVay, Jeffreys, King and Olsen49,Reference Levis and Gómez-Marín50) . For the quasi-experimental studies (n 6), one study had a medium risk of bias(Reference Black, LaCroix and Hoerster51) and five had a low risk of bias(Reference Wu and Lin52–Reference Wooldridge, Blanco and Dochat56). The risk of bias analysis indicated a generally low risk of bias within the included studies. This suggests a relatively high level of confidence in the overall findings.
Study and participant characteristics
The majority of studies were cross-sectional (n 12) and cohort-designed studies (n 11). A smaller number of RCT (n 4) and quasi-experimental studies (n 6) were also included. The number of participants in each study ranged from 28 to 315 919 participants, with a total of 654 323 participants in the studies reviewed. The ratios of male to female veterans are reported in Table 2, with most studies (31/33) having more male than female participants. Eight studies included only male participants(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Bakulski, Park and Weisskopf38–Reference Wang, Kim and Tucker42,Reference Levis and Gómez-Marín50,Reference Wu and Lin52) . The studies were predominately conducted in the USA (n 30), with the remaining studies conducted in Taiwan(Reference Wu and Lin52), Iran(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34) and Australia(Reference Hamirudin, Walton and Charlton53). This geographical concentration in the USA means the majority of data reflects the North American food environment and veteran healthcare system. The mean age of veterans was reported by thirty out of thirty-three studies and ranged from 44 to 82 years. The combined mean age of participants across studies was 63 years. One study reported the median age of participants, which was 67 years(Reference Mehta, Cassidy and Litonjua40), and one study reported the percentage of participants over 60 years, which was 69 %(Reference Dexter, Pope and Erickson54). One study did not report the mean or median age of the sample(Reference Ansley and Howard43).
Diet measurement
Standard dietary assessment methods, including FFQ, were used in twenty-nine of the studies. For the remaining four studies, one study used a 1-d diet recall and 2-d food record(Reference Cunningham, Verkaik and Gross37), one study used food diaries(Reference McVay, Jeffreys, King and Olsen49), one study used a comprehensive nutrition assessment conducted by a dietitian(Reference Erickson, Kwan and Gelberg48) and one study used a computer-assisted dietary interview(Reference Ansley and Howard43). Three of the studies also used blood tests to assess nutrient status(Reference Nosova, Chong and Alley26,Reference Koutrakis, Goldstein and Walia29,Reference Bakulski, Park and Weisskopf38) . Multiple nutrients were assessed across the included articles including energy (KJ) and macronutrients (fats, protein and carbohydrates), fibre, essential fatty acids and various micronutrients (vitamins and minerals). The most common micronutrients assessed included vitamins A, C, D and K, folate, Na, Ca, Mg, K, Se, Fe and Zn. Four studies also assessed added sugar consumption.
Diet quality scores
Nine studies calculated a diet quality score(Reference Hoerster, Wilson and Nelson19,Reference Parker, Perez and Phipps31–Reference Heredia, Thrift and Ramsey33,Reference Lash, Smith and Rinehart35,Reference Wu and Lin52,Reference Hoerster, Tanksley and Simpson55,Reference Wooldridge, Blanco and Dochat56) . The Healthy Eating Index (HEI) was used in four of the studies(Reference Parker, Perez and Phipps31–Reference Heredia, Thrift and Ramsey33,Reference Wooldridge, Blanco and Dochat56) , the Starting The Conversation short dietary screener diet quality score was used in two of the studies(Reference Hoerster, Wilson and Nelson19,Reference Hoerster, Tanksley and Simpson55) , the Mini Nutritional Assessment was used in two of the studies(Reference Wu and Lin52,Reference Hamirudin, Walton and Charlton53) and an FFQ diet score was used in one study(Reference Lash, Smith and Rinehart35). In all nine studies, the results indicated poor to fair diet quality(Reference Hoerster, Wilson and Nelson19,Reference Parker, Perez and Phipps31–Reference Heredia, Thrift and Ramsey33,Reference Lash, Smith and Rinehart35,Reference Wu and Lin52,Reference Hoerster, Tanksley and Simpson55,Reference Wooldridge, Blanco and Dochat56)
Synthesis and analysis of diet results
The following section provides the synthesis and analysis from the diet data extracted from the studies included in this review. Nutrient adequacy and inadequacy were calculated considering reference ranges for age and sex.
Energy and macronutrients
Fifteen of the studies assessed daily energy intake (kJ). Seven studies assessed carbohydrate intake, eight studies assessed protein intake and seven studies assessed fat intake. Four studies assessed essential fatty acids and seven studies assessed fibre. These results are presented in Table 5.
Synthesis and analysis
Energy – the recommended energy requirements were not met in eight of these studies(Reference Tan, Mallepally and Ho30,Reference Cunningham, Verkaik and Gross37,Reference Kaye, Heaton and Sohn39–Reference Wang, Ding and Tucker41,Reference Wang, Li and Nguyen44–Reference Ivey, Nguyen and Li46) , while six studies reported adequate intake(Reference Parker, Perez and Phipps31,Reference Heredia, Thrift and Ramsey33,Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Wang, Kim and Tucker42,Reference Erickson, Kwan and Gelberg48,Reference Hamirudin, Walton and Charlton53) , and one study indicated an overconsumption(Reference Ansley and Howard43). Carbohydrates – three studies reported adequate(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Kaye, Heaton and Sohn39,Reference Ivey, Nguyen and Li46) intake and four indicating inadequate intake(Reference Tan, Mallepally and Ho30,Reference Cunningham, Verkaik and Gross37,Reference Ansley and Howard43,Reference McVay, Jeffreys, King and Olsen49) . Protein – the majority (n 6) demonstrated adequate intake(Reference Parker, Perez and Phipps31,Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Guardino, Li and Nguyen45,Reference Ivey, Nguyen and Li46,Reference McVay, Jeffreys, King and Olsen49,Reference Hamirudin, Walton and Charlton53) and only two studies demonstrated inadequate intake(Reference Cunningham, Verkaik and Gross37,Reference Ansley and Howard43) . Fat – only two studies demonstrated inadequate intake(Reference Parker, Perez and Phipps31,Reference Kaye, Heaton and Sohn39) and five indicated consumption which exceeds recommendations(Reference Parker, Perez and Phipps31,Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Cunningham, Verkaik and Gross37,Reference Ivey, Nguyen and Li46,Reference McVay, Jeffreys, King and Olsen49) . Essential fatty acids – one study demonstrated suboptimal intake(Reference Guardino, Li and Nguyen45) and three reported adequate intake(Reference Nosova, Chong and Alley26,Reference Nosova, Bartel and Chong28,Reference Mehta, Cassidy and Litonjua40) . Fibre – six studies indicated inadequate intake(Reference Browne, Morey and Beckham10,Reference Nosova, Bartel and Chong28,Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Kaye, Heaton and Sohn39,Reference Mehta, Cassidy and Litonjua40,Reference Ivey, Nguyen and Li46) and only one indicated adequate intake(Reference Hamirudin, Walton and Charlton53).
Vitamins
Several vitamins were assessed in the different studies, including B1, B2, B3, B5, B12, C, D, E and folate. B1 and B2 were assessed in two studies(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Hamirudin, Walton and Charlton53) , B3 and B5 were assessed in one study(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34) and B6 and B12 were assessed in two studies(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Bakulski, Park and Weisskopf38) . Four studies assessed vitamin C(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Mehta, Cassidy and Litonjua40,Reference Wang, Kim and Tucker42,Reference Hamirudin, Walton and Charlton53) . Vitamin D was assessed in five studies(Reference Koutrakis, Goldstein and Walia29,Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Nahm, Charters and Yoo36,Reference Levis and Gómez-Marín50,Reference Hamirudin, Walton and Charlton53) . Intake of vitamin E was assessed in one study(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34). Three studies assessed folate(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Bakulski, Park and Weisskopf38,Reference Hamirudin, Walton and Charlton53) .
Synthesis and analysis
B1 – both studies displayed adequate intake(Reference Parker, Perez and Phipps31,Reference Levis and Gómez-Marín50) . B2 – both studies displayed adequate intake(Reference Parker, Perez and Phipps31,Reference Levis and Gómez-Marín50) . B3 – the one study which assessed this nutrient displayed adequate intake(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34). B5 – the one study which assessed this nutrient displayed adequate intake(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34). B6 – both studies demonstrated adequate intake(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Bakulski, Park and Weisskopf38) . B12 – both studies demonstrated adequate intake(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Bakulski, Park and Weisskopf38) . Vitamin C – all four studies, including those from the USA, Iran and Australia, displayed adequate intake(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Mehta, Cassidy and Litonjua40,Reference Wang, Kim and Tucker42,Reference Hamirudin, Walton and Charlton53) . Vitamin D – all five studies, including those from the USA, Iran and Australia, displayed inadequate intake(Reference Koutrakis, Goldstein and Walia29,Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Nahm, Charters and Yoo36,Reference Levis and Gómez-Marín50,Reference Hamirudin, Walton and Charlton53) . Vitamin E – the one study which assessed this nutrient displayed adequate intake(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34). Folate – two studies, one from the USA and one from Iran, displayed inadequate intake(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Bakulski, Park and Weisskopf38) , and one study from Australia displayed adequate intake(Reference Hamirudin, Walton and Charlton53).
Minerals
Several different minerals were assessed in the studies, including Na, Mg, Zn, Ca and potassium. Na was assessed in two studies(Reference Nosova, Bartel and Chong28,Reference Wang, Li and Nguyen44) , three studies assessed Mg intake(Reference Nosova, Bartel and Chong28,Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Hamirudin, Walton and Charlton53) , Zn was assessed in one study(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34), Ca was assessed in eight studies(Reference Browne, Morey and Beckham10,Reference Nosova, Bartel and Chong28,Reference Koutrakis, Goldstein and Walia29,Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Nahm, Charters and Yoo36,Reference Kaye, Heaton and Sohn39,Reference Wang, Kim and Tucker42,Reference Hamirudin, Walton and Charlton53) and three studies assessed K intake(Reference Nosova, Bartel and Chong28,Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Wang, Li and Nguyen44) .
Synthesis and analysis
Na – one study displayed adequate intake(Reference Wang, Li and Nguyen44), and the other displayed intake which exceeds recommendations(Reference Nosova, Bartel and Chong28). Mg – two studies (from Iran and the USA) indicated inadequate intake(Reference Nosova, Bartel and Chong28,Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34) , and one study (from Australia) indicated adequate intake(Reference Hamirudin, Walton and Charlton53). Zn – the one study which assessed this nutrient displayed inadequate intake(Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34). Ca – seven studies displayed inadequate intake(Reference Browne, Morey and Beckham10,Reference Nosova, Bartel and Chong28,Reference Koutrakis, Goldstein and Walia29,Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Kaye, Heaton and Sohn39,Reference Wang, Kim and Tucker42,Reference Hamirudin, Walton and Charlton53) and one displayed adequate intake(Reference Nahm, Charters and Yoo36). Potassium – all studies demonstrated inadequate intake(Reference Nosova, Bartel and Chong28,Reference Balali-Mood, Zilaee and Ghayour-Mobarhan34,Reference Wang, Li and Nguyen44) .
Food groups
Several studies reported daily serves of food groups such as fruits, vegetables, wholegrains, fish, meat, dairy products, fats, added sugars and fast food.
Synthesis and analysis
Fruit consumption did not meet recommendation in seven studies(Reference Browne, Morey and Beckham10,Reference Littman, McFarland and Thompson27,Reference Parker, Perez and Phipps31,Reference Lash, Smith and Rinehart35,Reference Wang, Ding and Tucker41,Reference Black, LaCroix and Hoerster51,Reference Dexter, Pope and Erickson54) and was adequate in only two studies(Reference Mehta, Cassidy and Litonjua40,Reference Wang, Li and Nguyen47) . For vegetables, all nine studies displayed inadequate intakes which do not meet the recommended guidelines in their respective countries(Reference Browne, Morey and Beckham10,Reference Littman, McFarland and Thompson27,Reference Parker, Perez and Phipps31,Reference Lash, Smith and Rinehart35,Reference Mehta, Cassidy and Litonjua40,Reference Wang, Ding and Tucker41,Reference Wang, Li and Nguyen47,Reference Black, LaCroix and Hoerster51,Reference Dexter, Pope and Erickson54) . Wholegrains – five studies displayed inadequate intake(Reference Browne, Morey and Beckham10,Reference Parker, Perez and Phipps31,Reference Wang, Ding and Tucker41,Reference Wang, Li and Nguyen47,Reference Black, LaCroix and Hoerster51) , with only two displaying adequate intake(Reference Mehta, Cassidy and Litonjua40,Reference Dexter, Pope and Erickson54) . Legumes – four studies displayed inadequate intake(Reference Browne, Morey and Beckham10,Reference Wang, Ding and Tucker41,Reference Wang, Li and Nguyen47,Reference Black, LaCroix and Hoerster51) , with only one study displaying adequate intake(Reference Littman, McFarland and Thompson27). Fish – two studies displayed inadequate intake(Reference Wang, Li and Nguyen47,Reference Dexter, Pope and Erickson54) , and two studies demonstrated adequate intake(Reference Littman, McFarland and Thompson27,Reference Wang, Ding and Tucker41) . Red and processed meat – one study displayed intakes which exceeded recommendations(Reference Wang, Ding and Tucker41), while another was within recommended limits(Reference Wang, Li and Nguyen47). Four studies assessed added sugars, with all finding an increased consumption(Reference Browne, Morey and Beckham10,Reference Littman, McFarland and Thompson27,Reference Kaye, Heaton and Sohn39,Reference Erickson, Kwan and Gelberg48) .
Health status
Information on co-occurring health conditions, health behaviours and mental health was also collected for many of the included studies. This includes BMI, co-occurring health conditions, smoking status, alcohol consumption, exercise and mental health status. These findings are displayed in Table 3. The majority of the included studies (n 22) collected data on the BMI of the participants, which ranged from 24·3 to 39·3. Four of the studies only recruited veterans who were overweight or obese(Reference Parker, Perez and Phipps31,Reference Lash, Smith and Rinehart35,Reference McVay, Jeffreys, King and Olsen49,Reference Wooldridge, Blanco and Dochat56) , with the participants in these studies having a combined average BMI of 36·14. For the other eighteen studies, the average BMI across the studies was 27·1. Three studies assessed mental health outcomes in healthy veterans (without post-traumatic stress disorder)(Reference Hoerster, Wilson and Nelson19,Reference Brostow, Donovan and Penzenik32,Reference Nahm, Charters and Yoo36) and found a high prevalence of mood disorders, with depression prevalence rates ranging from 45 to 55 % of the participants(Reference Brostow, Donovan and Penzenik32,Reference Nahm, Charters and Yoo36) , and low mental health quality of life scores being reported(Reference Hoerster, Wilson and Nelson19).
Discussion
This is the first systematic literature review to examine and assess the dietary intake of military veterans. The overall quality of the evidence was high, with a low risk of bias. The primary aim of this review was to systematically synthesise the dietary intake of veterans and compare these intakes to established NRV for individual nutrients. By doing so, specific nutrient profiles have been highlighted and the mechanisms of effect these nutrients have on health might be considered in future research. For example, inadequate intakes of fibre, folate, vitamin D, Ca and potassium are related to various immune, inflammatory and mental health symptoms(Reference Khiroya, Sekyere and McEwen57). In addition, this review also examined overall diet quality scores, with all nine studies reporting poor to fair diet quality. This was also reflected in the studies which assessed the frequency of food consumption, such as the number of servings of certain food groups consumed per day. We found that low intakes of vegetables, wholegrains and legumes were found among veterans. These findings are particularly significant as they underscore the potential nutritional deficiencies that may affect the overall health and well-being of veterans. Encouraging the consumption of wholegrains (e.g. oats and brown rice) and legumes (e.g. lentils and chickpeas) is essential for addressing both fibre and micronutrient gaps(Reference Miller58) identified in this population. This comprehensive analysis is intended to highlight areas for future research and clinical applications, providing a foundation for targeted dietary interventions and educational initiatives.
Across the studies, dietary components assessed frequently in veteran population were total energy intake, macronutrients (carbohydrates, protein and fats) and fibre, with many of the micronutrients, such as Na, only assessed in a small number of studies. Given the large public health focus on Na intake, particularly the negative health effects of Na overconsumption(Reference Hunter, Dhaun and Bailey59), it is notable that this has not been thoroughly examined in veteran populations. Excess Na consumption has been correlated with life expectancy and all-cause mortality worldwide(Reference Messerli, Hofstetter and Syrogiannouli60), with a recent systematic literature review and meta-analysis finding a significant linear relationship between dietary Na intake and CVD risk(Reference Wang, Yeh and Shih61). The review found the risk of CVD increased by up to 6 % for every 1 g increase in dietary Na intake(Reference Wang, Yeh and Shih61). Given that excess Na consumption is directly correlated with all-cause mortality globally, the lack of thorough examination in veteran populations represents a critical gap in morbidity tracking.
Other nutrients of interest include vitamin D, which was assessed in five studies, with all reported levels indicating suboptimal dietary intake. Vitamin D is crucial for health, particularly bone health, immune and cardiovascular health, and ageing(Reference Izzo, Carrizzo and Izzo62). Given the ageing population of veterans worldwide and the average age of 63 years across the participant pool in this study, vitamin D deficiencies often emerge in late adulthood. When coupled with the suboptimal intake of Ca and potassium noted in the included studies, these are essential nutrients linked with osteoporosis risk(Reference Muñoz-Garach, García-Fontana and Muñoz-Torres63) and other health conditions, including mental health conditions such as depression. To improve these markers, veterans should be encouraged to increase their intake of dairy products or Ca-fortified products for Ca(Reference Bourassa, Abrams and Belizán64), and fatty fish or fortified foods for vitamin D(Reference Bruins65).
Suboptimal nutrition also impacts the neuroendocrine system and has been implicated in the underlying pathology of depressive disorders(Reference Kris-Etherton, Petersen and Hibbeln66). For example, folate, a group of water-soluble compounds, plays a central role in numerous central nervous system functions(Reference Liwinski and Lang67). Individuals with depression often display low levels of serum and erythrocyte folate(Reference Liwinski and Lang67), suggesting a critical biochemical pathway through which folate is associated with depression. To address this, clinicians might encourage increased consumption of folate-rich foods such as legumes and green leafy vegetables(Reference Singh68). Given the high prevalence of mental health disorders among military veterans(Reference Carroll, Kearney and Miller9), understanding the critical and known role of nutrition in psychological health provides an opportunity to address deficiencies and deliver needed health awareness of core nutritional needs underpinning health.
The most appropriate and effective methods for assessing dietary intake is often a controversial topic in nutritional science(Reference Ravelli and Schoeller69). The majority of studies included in this review used FFQ, diet recalls or food diaries. While these methods are often cost-effective and time-efficient methodological choices, they come with several limitations, including recall bias, social desirability bias and measurement error(Reference Bailey70). It has been argued that blood tests to assess nutrient status is a more accurate and objective measure(Reference Landberg, Karra and Hoobler71). However, these can be invasive and costly and require increased participant burden, potentially affecting recruitment. Furthermore, many specific nutrients are not commonly assessed via blood tests and yield unreliable results(Reference Picó, Serra and Rodríguez72) due to issues pertaining to bioavailability(Reference Fiorentini, Cappadone and Farruggia73). More consistent use of dietary measures alongside routine blood tests of nutritional status and other physiological markers of health (i.e. cholesterol, blood sugars and liver function) are required to get a comprehensive assessment of dietary behaviours and nutritional status. Additionally, these findings underscore the importance of routine dietary assessments in future research, ensuring that nutritional adequacy remains a cornerstone of veteran health initiatives.
This review also aimed to synthesise common co-occurring health conditions, health behaviours and mental health reported in veteran populations. Numerous studies (n 18) assessed BMI, which is commonly used to screen for weight and, in some instance, act as a proxy marker of health for macro-nutritional status, whether undernutrition, normal range or overnutrition(Reference Wu, Li and Vermund74). The BMI as a measurement tool has received much criticism recently due to several limitations in its appropriateness as a useful marker of overall health(Reference Gutin75,Reference Bray76) . For example, BMI does not measure body fat distribution or recognise more harmful abdominal fat, or account for muscular weight or bone structure(Reference Wu, Li and Vermund74). Despite these well-documented limitations, the BMI remains a simple, inexpensive clinical screening tool for health status, which may explain its frequent use in the studies included in this review. The BMI is also important for neurocognitive and mental health outcomes, and despite the association between BMI, nutrition and physical health, there are few studies that measured general mental well-being as an integrated picture of health. This is particularly noteworthy given the mental health and suicide crisis facing veterans globally(Reference MacKenzie and Wegner77), and the bidirectional link between diet and mental health(Reference Grajek, Krupa-Kotara and Białek-Dratwa78); therefore, other measures, in addition to BMI, should be routinely considered in order to provide an integrative picture of health status.
Although the overall quality of the articles included in this review was high, there are several limitations which need to be acknowledged. The geographic scope of the included studies, primarily from the USA, indicates a lack of research on this topic globally, which is surprising as military service is still part of national service requirements in many parts of the world(Reference Jonsson, Salo and Lillemäe79). The inclusion of single studies from Australia, Iran and Taiwan provides a preliminary global perspective, but the heavy weighting towards US data significantly limits the heterogeneity of these findings. While the findings appear consistent across these dissimilar countries, the specific dietary drivers likely vary. Caution is therefore required when applying these primarily US-based conclusions to veteran populations in non-Western or different economic contexts. This limits the generalisability of the findings presented in this review as the results may not translate across countries and cultures, particularly regarding cross-cultural food and dietary habits within veteran populations. Additionally, only articles published in English within the past 10 years were included in this review which may have resulted in relevant articles published in languages other than English not being included. This may have affected the results and interpretations drawn.
A limitation of this review is the inherent variation in outcomes that may arise from using multiple country-based NRV. While this approach maximises regional relevance, it introduces minor discrepancies in the threshold for ‘adequacy’ across studies. Future research may benefit from applying a single standardised set of values to assess global trends, though this would sacrifice local specificity. However, the strength of the applied analysis of interpreting and comparing the diet data from each article against the relevant NRV allows for broad interpretations to be made. However, this method does not consider an individual’s specific nutritional requirements, health and lifestyle energy requirements, and therefore the analysis may over- or underestimate the range of inadequate intakes.
The analysis and synthesis of dietary intake through comparison with NRV and diet quality scores were a crucial component of this review and highlight critical nutritional gaps that can adversely impact veterans’ health. By evaluating veterans’ dietary intakes against population NRV, this review provides initial insights into nutritional inadequacies at a population-specific level. This provides a crucial first step for developing targeted nutritional interventions and policies tailored to veterans’ unique health challenges. By systematically identifying these gaps, the review offers a unique perspective on the intersection of nutrition and veteran health, emphasising the need for tailored dietary strategies to improve both physical and mental health outcomes. This foundational work may assist in informing policymakers, clinicians and future research aimed at addressing these critical nutritional needs, ultimately enhancing the quality of life for military veterans.
Additionally, future research should consider using common dietary measures such as FFQ alongside routine blood tests of nutritional status and other physiological markers of health (i.e. cholesterol, blood sugars and liver function) in order for a comprehensive assessment of dietary intake and nutritional status. This review has critically appraised existing evidence related to the nutritional intake of military veterans. By highlighting common and important nutrients and foods that are likely to be inadequate, policymakers, clinicians and organisations who support the physical and mental health of veterans can make informed, targeted approaches to address vitamin and mineral intake, including supplementation or behavioural change to improve the physical and mental health outcomes of military veterans.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526107120
Acknowledgements
This research did not receive any funding.
J. B., M. L. and T. B. contributed to the design of the research question and development of the search terms and contributed to the review protocol. J. B. conducted the initial database search with the final articles reviewed by M. L., J. B. and M. L. conducted the ROB analysis. J. B. and M. L. extracted and analysed the data. J. B. drafted the manuscript with reviews and edits by M. L. and T. B. J. B. has primary responsibility for the final content. All authors have read and approved the final manuscript.
The authors have no conflicts of interest to declare.



 Open access
Open access