
Understanding how people make decisions to engage in presenteeism, defined as working while sick, is essential for advancing theory and informing practice in this field yet also an underdeveloped area. Research has identified a range of factors that impact upon presenteeism (see Lohaus & Habermann, Reference Lohaus and Habermann2019, for a review), along with a range of consequences of this behavior, but has neglected to unwrap the decision-making process via which these factors interact to give rise to presenteeism. Whilst little is known about how individuals make the decision to enact presenteeism, three notable contributions in the field provide a foundation from which to start. First, Johns (Reference Johns2010) outlined that the decision process is triggered initially by a health event and is then influenced by individual and contextual factors or considerations. Second, Lohaus and Haberman (Reference Lohaus and Habermann2019) integrated the literature regarding antecedents and consequences of presenteeism into a framework outlining the “content of a decision-integrated model of presenteeism” (p. 53). Third, Cooper and Lu (Reference Cooper and Lu2016) adopted social cognitive theory to explain how an individual’s perceptions of their social environment may influence presenteeism behavior.
This chapter extends these foundations to propose a process model of presenteeism decision-making, encapsulating both sickness absenteeism and sickness presenteeism since both are potential outcomes of the same decision (Halbesleben et al., Reference Halbesleben, Whitman and Crawford2014; Hansen & Andersen, Reference Hansen and Andersen2008; Patton & Johns, Reference Patton and Johns2012). We draw upon the literatures relating to decision-making, sickness presenteeism, health behavior, and organizational behavior to outline the key decision-making principles and process steps likely to shape presenteeism decisions and therefore behavior.
The Importance of Understanding Presenteeism Decision-Making
A focus on understanding decision-making for presenteeism is timely for a number of reasons. First, definitions of presenteeism have evolved from simply attending work while ill (e.g., Aronsson & Gustafsson, Reference Aronsson and Gustafsson2005; Bergström et al., Reference Bergström, Bodin, Hagberg, Aronsson and Josephson2009; Cooper & Lu, Reference Cooper and Lu2016; Dew et al., Reference Dew, Keefe and Small2005; Hansen & Andersen, Reference Hansen and Andersen2009) to acknowledge presenteeism as a purposeful and adaptive behavior aimed at balancing conflicting health and work demands (Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020). Viewing presenteeism as a purposeful and adaptive behavior implies an intention on the part of the presentee, who considers the options and consequences of their behavioral choices. As such, it becomes evident how understanding the decision process related to intentions and goals, weighing alternative options, enacting a chosen behavior, and even reviewing whether that behavior was appropriate or successful is essential to our understanding of presenteeism and work-related health and wellbeing.
A second fundamental development in our understanding of presenteeism is the notion that presenteeism is not inherently detrimental to health but has a range of potentially positive consequences (e.g., Johns, Reference Johns2010; Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020; Karanika-Murray & Cooper, Reference Karanika-Murray, Cooper, Cooper and Lu2018; Lohaus, Habermann et al., Reference Lohaus, Habermann, Kertoubi and Röser2021; Whysall et al., Reference Whysall, Bowden and Hewitt2018). Ill health and work are not mutually exclusive. Instead, it is the appropriateness of the choice between sickness absence and presenteeism and/or among various adjustment options, taking into account the nature of the illness and the work demands (including any adjustments that can be made to the work tasks and/or work environment), which determines whether presenteeism will be beneficial or detrimental to health (Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020). In certain circumstances, taking sick leave could be beneficial for health (Bergström et al., Reference Bergström, Bodin, Hagberg, Aronsson and Josephson2009), yet under other circumstances, sickness presenteeism may provide a rehabilitative and restorative function (Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020; Whysall et al., Reference Whysall, Bowden and Hewitt2018). Indeed, the concept of vocational rehabilitation is based upon the understanding that when an employee’s health condition permits, they should be supported to remain in or to (re-)enter work as soon as possible (Waddell & Burton, Reference Waddell and Burton2006). This positions presenteeism as a sustainable option and a means of facilitating a gradual return to full working capacity, if the work environment is supportive and adequate resources are provided to aid adaptation and maximize positive consequences (Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020).
Third, there have been calls for a person-centered approach to understanding presenteeism behavior that can help to illuminate the variety of experiences, circumstances, and outcomes of presenteeism (Ruhle et al., Reference Ruhle, Breitsohl, Aboagye, Baba, Biron, Correia-Leal, Dietz, Ferreira, Gerich, Johns, Karanika-Murray, Lohaus, Løkke, Lopes, Martinez, Miraglia, Muschalla, Poethke, Sarwat, Schade, Steidelmüller, Vinberg, Whysall and Yang2019). Thus, leveraging the potential for presenteeism as an adaptive behavior that can help to balance and adjust to health and work demands and aid return to full working capacity require a better understanding of the decision-making process that underlies the presentees’ intentions and behavior. The question becomes not what factors are associated with presenteeism but how individuals make the decision to adapt and potentially also benefit from presenteeism.
Finally, presenteeism has always been more difficult to detect than sickness absenteeism, since the most common ailments accounting for presenteeism are not necessarily visible (e.g., Aronsson et al., Reference Aronsson, Gustafsson and Dallner2000). However, the widespread shift to home-working due to the Covid-19 global pandemic has further blurred the line between work and home, and in doing so, emphasizes the importance of definitions of presenteeism that avoid reference to presenteeism as attending work while sick. An individual does not have to attend a physical workplace to engage in presenteeism; they simply have to undertake work activities while sick, regardless of location. Remote working makes it more challenging for managers to spot and intervene when an imbalance between work demands and health needs arises, making presenteeism more likely (Ruhle et al., Reference Ruhle and Süß2020). Uncertainty as to whether we will ever return to pre-Covid levels of office working places even greater importance on developing ways to manage presenteeism more effectively, which hinges upon understanding the decision-making process through which presenteeism arises.
The Importance of Understanding the Process of Presenteeism Decision-Making
Understanding of any phenomenon must answer both the what and, most importantly, how questions. Knowledge regarding the what of presenteeism is relatively more advanced, with numerous factors which impact on presenteeism having been identified (see Lohaus & Haberman, Reference Lohaus and Habermann2019), but we know little about how a choice to engage in sickness presenteeism is made or revised. Whilst categorical (or descriptive) theories aim to categorize the inputs for the end behavior and explain its variance, process theories formulate the range of inputs and its mediators into sequential steps (McGuire, Reference McGuire1983). In relation to presenteeism, Lohaus and Haberman (Reference Lohaus and Habermann2019) describe these as content and process theories. Content models have their place but do not explain the psychological mechanisms and processes that can give rise to specific behaviors. Thus, a process approach would usefully augment existing knowledge by helping to explain the how and why of presenteeism behavior, also offering high practical value for supporting effective decision-making, maximizing benefits while minimizing negative impact of presenteeism on health or performance.
Current Understanding of Presenteeism Decision-Making
We put a decision-making lens on existing presenteeism literature to ask: what do we know about how people make the decision to abstain from work or continue to work when they are feeling unwell? We partition the current relevant knowledge into broad questions pertaining to the presenteeism decision: decision triggers, influences, consequences, and mechanisms, latterly integrating insights from the decision-making literature to build a more comprehensive understanding of the decision-making process for presenteeism.
Triggers of the Presenteeism Decision
Notable in the presenteeism literature is the idea that a health event triggers the need to decide between continuing to work in the face of compromised health or taking sickness absence (e.g., Aronsson & Gustafsson, Reference Aronsson and Gustafsson2005; Johns, Reference Johns2010). Work attendance with 100% productivity is “interrupted by a ‘health event’ that is either acute (e.g., the flu), episodic (e.g., migraine), or chronic (e.g., the onset of diabetes)” (Johns, Reference Johns2010, p. 531). Thus, the initial choice between absenteeism or presenteeism is determined by the nature and severity of the health event. In extreme medical cases, absence may be unavoidable regardless of the circumstances, whereas with less extreme medical conditions, contextual factors will be more salient and influential. For instance, Johns (Reference Johns2010) highlights that suffering from a sore throat may require absenteeism for a singer but allow presenteeism for a pianist. However, the model does not extend to explanation of how this decision is made, how individuals explore options, choose between alternatives, or review their decisions to adjust their behavior.
Central in the presenteeism literature is the notion that presenteeism and absenteeism are two potential outcomes of the same decision (Johns, Reference Johns2010). However, rather than one being a direct substitution for the other (as in substitution hypothesis; Caverley et al., Reference Caverley, Cunningham and MacGregor2007), evidence suggests that the two tend to be highly correlated (Leineweber et al., Reference Leineweber, Westerlund, Hagberg, Svedberg and Alexanderson2012; Whysall et al., Reference Whysall, Bowden and Hewitt2018) and even complementary (Gosselin et al., Reference Gosselin, Lemyre and Corneil2013). Critically, we suggest that the range of attendance behaviors and possible work adjustments in the face of ill-health imply that a binary choice is too simplistic. There a range of different types of presenteeism behavior, as illustrated in the health-performance framework (Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020), depending on what adjustments can be made around or to the job, as job crafting theory suggests (Tims & Bakker, Reference Tims and Bakker2010), but also on the level of discretionary effort applied by each individual to their work whilst sick. This could range from attending to one’s full range of tasks and maintaining 100% productivity, to being notionally “working” (irrespective of location) yet minimally productive. Furthermore, we previously acknowledged how increased home working blurs the line between work and home. In addition, we argue, it blurs the line between sickness absence and presenteeism. If an individual has officially taken sickness absence yet attends work during this time (e.g., checks their emails or attends to an urgent request), this immediately becomes presenteeism. To understand the complex evaluative processes involved, it is important to understand the stages and nuances of this decision process.
Influences on Presenteeism as Inputs for Decision-Making
A starting point to understanding how presenteeism decisions are made is to identify the influences on evaluation of decision options and the expected consequences. The dynamic model of presenteeism (Johns, Reference Johns2010) lists work context-related factors (e.g., high job demands, low job security, strict absence policy) and person-related factors (e.g., work attitudes, health locus of control, personality, perceived absence legitimacy) as key influences on the choice between absenteeism and presenteeism behavior, to which Miraglia and Johns’s (Reference Miraglia and Johns2016) meta-analysis added mediating factors. Lohaus and Habermann (Reference Lohaus and Habermann2019) comprehensively integrated the literature on these numerable influences into environmental (e.g., cultural norms, economic climate), organizational (e.g., absence policy, organizational support), job-related (e.g., role demands, adjustment latitude), and person-related (e.g., health, engagement). Macro-level influences (or environmental influences, as per Lohaus & Habermann, Reference Lohaus and Habermann2019) have received much less attention yet include economic circumstances such as recession (since absence rates are generally lower during recession), national unemployment rates (during which presenteeism rates tend to increase; Aronsson et al., Reference Aronsson, Gustafsson and Dallner2000; Markham, Reference Markham1985), cultural differences (such as the Confucius culture in which values of working long hours and working intensively are deep-rooted; Cooper & Lu, Reference Cooper and Lu2016), or dominant political systems (absenteeism rates differ between communist and capitalist countries; Patton & Johns, Reference Patton and Johns2012). Macro factors shape the fundamental values, beliefs, and attitudes that underlie our work behavior and are therefore essential to presenteeism decision-making. Indeed, more distal influences on behavior are viewed as essential considerations within sickness absence research (Kristensen, Reference Kristensen1991) and may be more salient for decision-making than we assume, as they define how important work centrality is for the individual (Addae et al., Reference Addae, Johns and Boies2013).
It is important to understand not only the relative salience of each group of influences but also how they may interact to influence decision outcomes. It has been argued that work-related factors can be more important than personal factors in presenteeism decision-making (Hansen & Andersen, Reference Hansen and Andersen2008). For example, whilst individual differences are likely to exist regarding perceived absence legitimacy, this is also likely to differ according to sick pay provisions, size of employer, and nature of work (Irvine, Reference Irvine2011). Similarly, larger organizations tend to provide more generous sick pay and may be perceived as able to carry the burden of their absence more readily than smaller organizations. In addition, work and environment-related factors and personal factors are likely to operate synergistically and bidirectionally, as opposed to independently of each other (Cooper & Lu, Reference Cooper and Lu2016; Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020). For example, high neuroticism may mean that others’ opinions have a stronger influence on one’s decisions, or that we evaluate the environment more pessimistically (Cooper & Lu, Reference Cooper and Lu2016).
Consequences of Presenteeism as Outputs of Decision-Making
The decision to attend work when one is feeling unwell can have a range of consequences for the individual, their work team(s), and the organization. Lohaus and Habermann (Reference Lohaus and Habermann2019) made a useful distinction between organizational vs. individual consequences, separately for presenteeism and absenteeism decisions. Most documented have been the negative consequences of presenteeism as a deleterious behavior due to its potentially high costs in terms of health and performance, to the extent that presenteeism research has been criticized for falling short in failing to acknowledge the benefits of presenteeism (Lohaus & Habermann, Reference Lohaus and Habermann2019). Recently, there has been an increasing focus on potentially positive outcomes (e.g. Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020; Lohaus & Habermann, Reference Lohaus and Habermann2019; Lohaus et al., Reference Lohaus, Habermann, Kertoubi and Röser2021; Whysall et al., Reference Whysall, Bowden and Hewitt2018) and a “neutralization” of presenteeism as a work behavior that is not necessarily inherently positive or negative, instead seeking to understand the function of the behavior for the presentee (Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020). Consequently, the health-performance framework of presenteeism (Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020) identifies two key considerations for the presentee in view of their impaired health: to support their health and to attend to work commitments. Together, these considerations give rise to four types of presenteeism, each associated with different patterns of behavior and outcomes in terms of whether and how health and/or performance are impacted (functional, dysfunction, overcommitted, and therapeutic). Although the health-performance framework does not explicate how possible options and consequences are considered in presenteeism decision-making, it acknowledges that presenteeism involves a decision, driven by the need to balance health and performance.
Additionally, it is important to recognize that presenteeism behavior may have both intended and unintended consequences; presentees may have well-articulated goals and expectations (e.g., manage work demands in the immediate term) but experience unexpected or unforeseen consequences from their behavior (e.g., reduced ability to recover and longer-term sickness absence). Unintended consequences relate to both health and performance/productivity (Bergström et al., Reference Bergström, Bodin, Hagberg, Aronsson and Josephson2009), such as future sickness absenteeism or prolonged periods of rehabilitation (Bergström et al., Reference Bergström, Bodin, Hagberg, Aronsson and Josephson2009) or even a cycle of ill health (Johns, Reference Johns2010). Unintended consequences may be both direct or indirect (e.g., impact on coworker or supervisor work or attributions of the presentee), as well as difficult to quantify or even identify. For example, a presentee may decide to work whilst experiencing influenza or other virus symptoms in order to maintain job security or financial stability, but for their colleagues, being present at work with an infectious illness may be perceived as irresponsible. Conversely, if a decision to take sickness absence is perceived as demoting a lack of commitment and receives backlash or disapproval from one’s colleagues or manager, the individual may be more likely to opt for presenteeism in future.
Mechanisms That Can Explain How Decisions to Enact Presenteeism Are Reached
Between inputs and outputs, influences and consequences, there is the black box of presenteeism decision-making. Through what process is the decision to enact presenteeism or sickness absenteeism is reached?
A Rational Evaluation Process
Classical decision theory, the most notable example of which is expected utility theory (EUT, 1947, 2007), treats decision-making as a rational, analytic process. It posits that decision-makers evaluate all possible options in terms of perceived value or benefit, subsequently selecting the option that offers the highest expected utility, defined as its perceived value weighted by the probability that it will occur (Mongin, Reference Mongin, Davis, Hands and Maki1997). Under EUT, therefore, all decisions are viewed as rational, based on a comprehensive analysis of all potential options in terms of expected value and likelihood, from which the optimal option is selected. Similar principles are echoed in health behavior theories such as the health belief model, for example, which holds assessment of expected costs and benefits as core to health-related behavioral outcomes (Janz & Becker, Reference Janz and Becker1984). Applied to presenteeism, the immediate question this raises is one of value or benefit (or, indeed, costs) in relation to what or, indeed, whom. Value in terms of the individual’s job and financial security, potential future career progression, or work productivity? Or value in terms of the individual’s own health and wellbeing? However, such theories overlook the influence of personal factors, which, as discussed above, appear to influence presenteeism (Lohaus & Habermann, Reference Lohaus and Habermann2019; Miraglia & Johns, Reference Miraglia and Johns2016). In terms of dispositional factors such as personality or work-related values, for instance, it can be seen how an individual high in conscientiousness or with a strong work ethic would be likely to place a stronger weighting on the productivity benefits of presenteeism above the potential health benefits through absenteeism.
Psychological Influences, Motives, Biases, and Heuristics
Consequently, it is important to draw upon theories which acknowledge the influence of psychological factors such as an individual’s values, preferences, and beliefs about their abilities, such as Vroom’s (Reference Vroom1964) expectancy theory and the work of Tversky and Kahneman (Reference Tversky and Kahneman1974; Kahneman & Tversky, Reference Kahneman and Tversky1979). Vroom acknowledged that decisions arise from an evaluation of the anticipated consequences, but not in an entirely rational or objective way. Subjectivity is introduced in the individual’s evaluation on three key dimensions: expectancy, instrumentality, and valence. Expectancy relates to the likelihood that the effort will lead to the intended goals. In presenteeism terms, this could relate to assessment of the likelihood that if one attempts to work, they will be able to do an acceptable job and/or be perceived positively by their colleagues and/or line manager, for instance. This judgment is typically influenced by personal factors such as self-confidence (or self-efficacy, as referenced in social cognitive theory and applied to presenteeism by Cooper & Lu, Reference Cooper and Lu2016) and contextual factors such as the degree of control over their work tasks and/or environment. The second judgment is one of instrumentality, belief that the desired reward will be received if the performance expectations are met. In the context of presenteeism, this could include the belief that a strong attendance record is likely to lead to promotion or pay benefits or, conversely, that taking sickness absence will enhance recovery. Again, this judgment will be influenced by both personal factors (such as health locus of control) and contextual factors (such as organizational policies for pay increases and promotion). The third judgment is valence, the extent to which the individual values the reward/benefits and therefore introduces the influence of individual differences in goals, values, and preferences. Indeed, goals have been neglected in presenteeism research (Cooper & Lu, Reference Cooper and Lu2016), yet both expectancy theory and theories such as social cognitive theory (Bandura, Reference Bandura1986, 1997, 2001) highlight the important influences of personal goals in shaping behavior.
In terms of values and motives, it has been suggested that there are two motives which underlie presenteeism decision-making: approach and avoidance (or push and pull) motives (Cooper & Lu, Reference Cooper and Lu2016; Lu et al., Reference Lu, Lin and Cooper2013, Reference Lu, Peng, Lin and Cooper2014; Miraglia & Johns, Reference Miraglia and Johns2016). Employees with approach motives will be more likely to choose presenteeism over absenteeism driven by the desire to “abide by one’s work values and beliefs of achievement and loyalty to the profession and interested parties” (Cooper & Lu, Reference Cooper and Lu2016, p. 223). In contrast, employees with avoidance motives may engage in presenteeism to avoid potential social disapproval and financial loss as a consequence of taking sick leave. An important question is whether there is any systematic difference between approach or avoidance motives in terms of outcomes; for example, whether an avoidance motive is more likely to lead to dysfunctional presenteeism and thereby be detrimental to health, or an approach motive to functional presenteeism which is restorative to health.
Viewed in relation to decision-making theory, it is also reasonable to assume that avoidance motives may disproportionately guide behavior. Tversky and Kahneman (Reference Tversky and Kahneman1974; Kahneman & Tversky, Reference Kahneman and Tversky1979) demonstrated that decision-making often violates the rules of rational decision-making in specific, systematic ways known as heuristics and cognitive biases (Kahneman et al., 1982; Kahneman & Tversky, Reference Tversky and Kahneman1973; Tversky & Kahneman, Reference Tversky and Kahneman1974). Kahneman and Tversky (Reference Kahneman and Tversky1979) proposed prospect theory, which, like EUT, recognizes the evaluation of perceived value and weighting of likelihood as the foundation of decision-making but also acknowledges the influence of certain psychological features introducing a level of subjectivity and irrationality into decision-making. A key example is loss aversion: an exaggerated aversion to potential losses in comparison to equivalent potential gains and an overweighting of low probabilities and underweighting of high probabilities (Tversky & Kahneman, Reference Tversky and Kahneman1981). Expectancy and prospect theory, therefore, illustrate the ways in which work context-related factors (e.g., high job demands, low job security, strict absence policy) and person-related factors (e.g., work attitudes, health locus of control, personality, perceived absence legitimacy) outlined in Johns’s (Reference Johns2010) dynamic model of presenteeism and Lohaus and Haberman’s (Reference Lohaus and Habermann2019) decision-making content framework may interact to influence the evaluation of options.
The Influence of Context
Tversky and Kahneman not only highlighted the influence of psychological factors on the evaluation of options but also demonstrated the influence of psychological and contextual factors on the options that are included for consideration in the first place. They demonstrated that decision options are framed by both intrinsic forces relating to the decision-maker such as temperament, emotional state and beliefs, and extrinsic influences such as the way decision options are presented (Tversky & Kahneman, Reference Tversky and Kahneman1981). Certain contexts are known to “prime” associated knowledge structures (schemas) to influence decision outcomes, similarly to the principles outlined in recognition-primed decision making (Klein, Reference Klein, Klein, Orasanu, Calderwood and Zsambok1993). In these situations, decisions are made not as a result of different decision options being evaluated against one another; instead, previously established associations are automatically activated and acted upon (e.g., Cohen-Hatton et al., Reference Cohen-Hatton, Butler and Honey2015; Doya, 2008).
The mechanics behind framing effects can be explained by dual-process theories, such as Wason and Evans’s (Reference Wason and Evans1975) and Evans’s (Reference Evans1984) dual process theory of reasoning distinguishing between heuristic processes and analytic processes, and Kahneman’s (Reference Kahneman2003, Reference Kahneman2012) distinction between system 1 (intuition) and systems 2 (reasoning) thinking. Wason and Evans identified heuristic processes as the means by which individuals select which information is relevant to the current situation, automatically filtering out irrelevant information. Kahneman (Reference Kahneman2003, Reference Kahneman2012) built on this with his distinction between intuition and reasoning, whereby intuition (or system 1) is rapid and automatic, often influenced strongly by emotional states, and based on ingrained habits that are resistant to change. When experiencing psychological stress, decision-makers seek to resolve the decision as quickly as possible, increasing the likelihood of suboptimal decision-making (e.g., Janis & Mann, Reference Janis and Mann1976). Indeed, the framing effect has been found to be associated specifically with amygdala activity, also inferring a key role for an emotional system in mediating decision biases (De Martino et al., Reference De Martino, Kumaran, Seymour and Dolan2006). Thus, with presenteeism, high levels of stress or strong emotional states may increase the likelihood that certain options are automatically filtered out of consideration and, as a result, suboptimal decisions.
Following the heuristic process, analytic processes are then employed to make judgments about the situation based on the information deemed relevant (Evans, Reference Evans1984). Kahneman described this as reasoning (or system 2) thinking, considered to be slower, subject to more considered judgments and conscious evaluation. Generally, individuals adopt system 1 for making simple and quick decisions, and system 2 is for more complex decision-making. It is via system 2-driven reasoning processes, for example, that presenteeism decisions may become influenced by consideration of social norms and expectations.
The Role of Social Norms
Cultural and social norms are likely to have a strong influence on presenteeism decisions, since the coevolution process has
endowed us with preferences that go beyond the self-regarding concerns emphasised in traditional economic and biological theories, and embrace such other-regarding values as a taste for cooperation, fairness, and retribution; the capacity to empathize; and the ability to value such constitutive behaviors as honesty, hard work, toleration of diversity, and loyalty to one’s reference group.
Social and cultural norms typically influence behavior through conformity effects, as a result of which individuals accept the dominant cultural practices, which may then become internalized through social learning (Gintis, Reference Gintis2007). Indeed, research has shown that leaders’ presenteeism has a positive effect on employee presenteeism (Dietz et al., Reference Dietz, Zacher, Scheel, Otto and Rigotti2020).
The influence of perceived societal norms is also acknowledged in the theory of planned behavior (TPB; Ajzen, Reference Ajzen1988, Reference Ajzen, Kuhl and Beckmann1985), perhaps the most widely researched model of health behavior, which outlines the key determinants of health-related behavior as: attitudes towards the behavior (involving beliefs about and evaluations of outcomes), perceived behavioral control (influenced by internal and external factors), and subjective norms (beliefs about significant others’ attitudes towards the behavior, and motivation to comply with others). Together these influences combine to trigger a behavioral intention – in other words, a decision to act in a particular way; which may or may not translate into action, depending on the level of control, influenced by available resources, opportunities, and perceived barriers.
Social norms critical to presenteeism decision-making relate to the attendance culture of an organization (Ruhle & Süß, Reference Ruhle, Breitsohl, Aboagye, Baba, Biron, Correia-Leal, Dietz, Ferreira, Gerich, Johns, Karanika-Murray, Lohaus, Løkke, Lopes, Martinez, Miraglia, Muschalla, Poethke, Sarwat, Schade, Steidelmüller, Vinberg, Whysall and Yang2019), which integrates both absence culture, the beliefs and practices that influence absence frequency and duration (Martocchio, Reference Martocchio1994), and presenteeism culture, the perceptions of attending work while ill (Dew et al., Reference Dew, Keefe and Small2005). As emphasized by Ruhle and Süß, an integrated view of presenteeism and absenteeism norms is essential since the two behaviors are “not merely opposites but related phenomena and may be influenced by (and influence) a common attendance culture” (Ruhle & Süß, Reference Ruhle, Breitsohl, Aboagye, Baba, Biron, Correia-Leal, Dietz, Ferreira, Gerich, Johns, Karanika-Murray, Lohaus, Løkke, Lopes, Martinez, Miraglia, Muschalla, Poethke, Sarwat, Schade, Steidelmüller, Vinberg, Whysall and Yang2019, p. 242). The key variable shaping attendance culture is perceived legitimacy, of both sickness absence and presenteeism. A culture characterized by strong perceived legitimacy of sickness absence gives rise to a health-focused culture, whereas perceived legitimacy of sickness presenteeism gives rise to a “presentistic” culture, and one which perceived legitimacy in both behaviors denotes an individual decision culture (Ruhle & Süß, Reference Ruhle, Breitsohl, Aboagye, Baba, Biron, Correia-Leal, Dietz, Ferreira, Gerich, Johns, Karanika-Murray, Lohaus, Løkke, Lopes, Martinez, Miraglia, Muschalla, Poethke, Sarwat, Schade, Steidelmüller, Vinberg, Whysall and Yang2019). The key question, however, is how culture influences the decision process. Ruhle and Süß (Reference Ruhle, Breitsohl, Aboagye, Baba, Biron, Correia-Leal, Dietz, Ferreira, Gerich, Johns, Karanika-Murray, Lohaus, Løkke, Lopes, Martinez, Miraglia, Muschalla, Poethke, Sarwat, Schade, Steidelmüller, Vinberg, Whysall and Yang2019) articulate two potential mechanisms: firstly, by indicating to individuals the type of attendance behavior that is considered legitimate in that particular context (Xie & Johns, Reference Xie and Johns2000), and secondly, in moderating the relationship between attitudes and attendance behavior (Nicholson & Johns, Reference Nicholson and Johns1985). Absence culture, the beliefs and practices that influence absence frequency and duration (Martocchio, Reference Martocchio1994), describes a collective process in an organization and/or its subunits (e.g., groups, departments) that impacts the individuals’ patterns of absence (Nicholson & Johns, Reference Nicholson and Johns1985). Presenteeism culture describes the perceptions of attending work while ill (Dew et al., Reference Dew, Keefe and Small2005; Simpson, Reference Simpson1998).
Applying social cognitive theory (Bandura, Reference Bandura1986) to presenteeism behavior, Cooper and Lu (Reference Cooper and Lu2016) highlighted how individual-level constructs such as self-efficacy, outcome expectations, and goal representations are influenced, over time, through exposure to other people and events in their social context. This exposure differentially reinforces certain options above others, and through repeated exposure, people revise their self-efficacy beliefs, outcome expectations, and possibly even their goals. More recently, Miraglia and Johns’s (Reference Miraglia and Johns2021) multilevel model of the social relational dynamics that impact on absenteeism linked the range of work and nonwork social influences via six paths. These six paths and related theories explain how these social factors operate, encompassing normative influence, social exchange, job resources, work attitudes, emotions, and ethics. As such, it posits the presenteeism decision in its important broader socio-psychological context.
The Role of Feedback
Considering presenteeism behavior as driven by the need to balance health status and work demands (Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020), it is important to acknowledge that the decision to be present or absent will also be ongoing and revised as health status and work demands change. Indeed, Busemeyer and Townsend (Reference Busemeyer and Townsend1993) and Busemeyer and Johnson (Reference Busemeyer, Johnson, Koehler and Harvey2004) criticized the absence of attention to the deliberation process in decision-making theories, which involves indecisiveness, vacillation, inconsistency, lengthy deliberation, and distress. In response, they put forward decision field theory aimed at understanding the motivational and cognitive mechanisms that guide the deliberation process involved in decisions under uncertainty. Specifically, they highlighted that earlier theories do not account for why preferences may waver over time, nor do they explain why deliberation may be drawn out or how long it may last. Decision field theory (Busemeyer & Johnson, Reference Busemeyer, Johnson, Koehler and Harvey2004; Busemeyer & Townsend, Reference Busemeyer and Townsend1993) emphasizes the dynamic nature of decision-making process, stating that deliberate decision-making involves switching focus between alternatives, considering the consequences of each alternative over a period of time. As each possible consequence is brought to mind, it triggers different affective reactions, which are evaluated and compared in terms of desirability.
The consequences of presenteeism, in terms of both health consequences and experienced gains and losses in relation to one’s goals, are likely to be an important source of feedback and to impact on both the current and subsequent presenteeism decisions (Cooper & Lu, Reference Cooper and Lu2016; Johns, Reference Johns2010). For example, if an employee had a negative experience of taking sickness absence in the past, perhaps due to negative managerial attitudes, it may be more likely that they will opt to engage in presenteeism in the future. Indeed, the dynamic model of presenteeism (Johns, Reference Johns2010) includes an important feedback loop that is created by the impact of the consequences of choosing between presenteeism or absenteeism on the original health event. Feedback is likely to create a learning loop during and/or after the presenteeism episode: was my decision to attend work appropriate, did I achieve/am I achieving what I was hoping to achieve, how did the decision affect my health, and do I need to revise my decision? In keeping with values-driven decision-making theory (e.g., Kahneman & Tversky, Reference Kahneman and Tversky1979; Tversky & Kahneman, Reference Tversky and Kahneman1974; Vroom, Reference Vroom1964), we propose that the impact of these different consequences – namely, on the individual in terms of their health or productivity, on colleagues/managers and their attitudes towards the individual, and on the organization in terms of results – will be differentially weighted according to the individual’s own goals and values. For instance, an individual who values a good work–life balance would be expected to place more weight on feedback in terms of the impact on their health, compared to an individual who is driven by ambition and a desire for promotion, who would be expected to place more weight on feedback in relation to their manager’s or other senior colleagues’ reactions.
Busemeyer and Johnson (Reference Busemeyer, Johnson, Koehler and Harvey2004) contend that these comparisons of consequences are accumulated over time to form a preference state. Once the feeling of the desirability of action passes a threshold, this action is chosen. As a result, the threshold is a key parameter controlling the decision speed and quality trade-off; if the threshold is set low, only a weak preference is required to reach a choice, whereas if it is set to a very high threshold, a strong preference is required to make a decision. In this case, deliberation takes longer, but the decision is based on a more thoughtful evaluation of all the consequences (Busemeyer & Johnson, Reference Busemeyer, Johnson, Koehler and Harvey2004). Echoing the highly interactive influence of individual and contextual influences on decision-making, Busemeyer and Johnson also acknowledge that impulsive individuals may tend to use lower thresholds, while perspicacious individuals may tend to use higher thresholds.
A Conceptual Model of the Decision-Making Process for Presenteeism
In the following section, we integrate and consolidate existing presenteeism research and decision-making theory, as outlined above, into a process model of presenteeism decision-making. We hope that this will provide a launchpad from which we can then test and refine our understanding of this critical process and transfer these insights into practice to support individuals to make better decisions and managers to support the employees. From our analysis of the available literature, we discern four potential stages of the decision-making process of presenteeism: (1) a trigger that necessitates the decision (what happened? how severely am I affected?), (2) perceived available options (what could I do? what is possible?), (3) evaluation of options in terms of perceived benefits/risks and potential consequences (what should I do?), and (4) seeking feedback and evaluating the decision (was this the right decision? did I achieve my aims?) (see Figure 7.1).
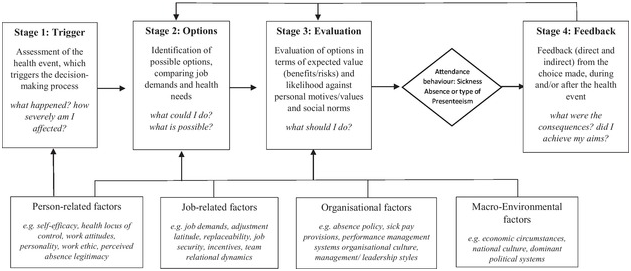
Figure 7.1 The decision-making process of presenteeism
Stage 1: Trigger
Stage 1 concerns a self-assessment of the health event, which comprises the trigger for the decision-making process, focused narrowly around the question of illness severity (Johns, Reference Johns2010). Given the subjectivity of health and illness (e.g., Johns, Reference Johns2010; Van Hooft, Reference Van Hooft1997), personal factors are likely to influence each individual’s appraisal of the severity of their health condition (e.g., pain thresholds, Jensen et al., Reference Jensen, Rasmussen, Pedersen and Olesen1993; genetics, Diatchenko et al., Reference Diatchenko, Slade, Nackley, Bhalang, Sigurdsson, Belfer, Goldman, Xu, Shabalina, Shagin, Max, Makarov and Maixner2005; locus of control, Crisson & Keefe, Reference Crisson and Keefe1988). Consequently, similar to Busemeyer and Johnson’s (Reference Busemeyer, Johnson, Koehler and Harvey2004) concept of decision thresholds, there may be a threshold at which a health condition is automatically deemed to necessitate sickness absence, without deliberation. For some individuals and/or some health conditions, the threshold for deliberation may be very low, with very few health events automatically warranting sickness absence, whereas for others it may be high. Furthermore, given the that rapid and automatic processing is strongly influenced by emotional states (e.g. Kahneman, Reference Kahneman2012), this threshold may also change situationally, for instance when individuals are experiencing stress or anger. Thus, if the health event is considered sufficiently serious that that absenteeism is immediately deemed the only option, then this behavior is selected without evaluation of the options.
Stage 2: Options
Stage 2 concerns the identification of perceived available response options. We know that identification of possible options is likely to be influenced by framing effects and other heuristics such as priming and availability bias (Tversky & Kahneman, Reference Tversky and Kahneman1973, Reference Tversky and Kahneman1981), which in turn are influenced by individual and situational factors. In some national or organizational cultures, for instance, sickness absence may not even be considered an option in relation to only mild health events. This stage reflects the “editing” stage of French and colleagues’ two-stage editing and evaluation making theory (French et al., Reference French, Maule and Papamichail2009), involving constructing a decision frame, influenced by personal values and normative or situational influences. Conversely, if an employer has recently run a health promotion campaign highlighting the importance of managing work–life balance, this may prime sickness absence as a feasible option.
Whilst automatic filtering of options via framing reflects what Kahneman referred to as intuitive, system 1 thinking, it is likely that the identification of options also involves more deliberate and considered cognitive processes associated with system 2 thinking. We propose that “options” here refer not only to a binary choice between absenteeism and presenteeism but also to different types of presenteeism: the range of options between full and partial productivity (e.g., attending to a limited range of tasks only, working but performing a poor job, or working reduced hours), which can be created through attempts to adjust work tasks to accommodate health limitations or capacities (health-performance framework of presenteeism; Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020). Consequently, identification of options is likely to include considerations relating to how the health condition affects work capacity: what tasks am I able to carry out with my symptoms? and how can I adapt the tasks (both the associated demands and/or resources) until my health improves? This necessitates a more nuanced judgment, weighing up the symptoms (mental, physical, severe, less mild, etc.) against work-related variables such job demands (Demerouti et al., Reference Demerouti, Le Blanc, Bakker, Schaufeli and Hox2009; Kivimäki et al., Reference Kivimäki, Head, Ferrie, Hemingway, Shipley, Vahtera and Marmot2005), ease of replacement (Aronsson & Gustafsson, Reference Aronsson and Gustafsson2005; Biron et al., Reference Biron, Brun, Ivers and Cooper2006; Dew et al., Reference Dew, Keefe and Small2005; Widera, et al., Reference Widera, Chang and Chen2010), and adjustment latitude (Krohne & Magnussen, Reference Krohne and Magnussen2011). Indeed, these considerations echo the two-stage appraisal process captured within the cognitive-mediational theory of stress (Lazarus, Reference Lazarus1993), which proposes that after evaluating a potential threat (i.e., primary appraisal, akin to stage 1 in this process) we then determine what resources we have at our disposal to manage a situation (i.e., secondary appraisal, stage 2 in this process). Once an individual has identified what they deem to be possible, we propose the decision process moves on to consider what is desirable, in relation both to their own goals and social norms and expectations.
Stage 3: Evaluation
Stage 3 is the evaluation of the options in terms of expected value and likelihood and is therefore focused less on what is possible and more on the individual’s own wants and motivations, in addition to organizational factors and social norms and what they believe they “should” do. It reflects the second stage in French et al.’s (Reference French, Maule and Papamichail2009) decision-making process. Whilst editing involves constructing a decision frame, evaluation involves weighing the “framed” options against the individual’s goals and objectives and anticipated outcomes. Consequently, this evaluation is likely to be influenced by the push and pull (Miraglia & Johns, Reference Miraglia and Johns2016) or approach and avoidance motives (Cooper & Lu, Reference Cooper and Lu2016; Lu et al., Reference Lu, Lin and Cooper2013, Reference Lu, Peng, Lin and Cooper2014) of presenteeism. Low job satisfaction, for example, may lead individuals to place more weight on the benefits of sickness absence in terms of their own health and wellbeing than on productivity or work commitment from presenteeism when feeling dissatisfied with work.
It involves a series of judgments involving cognitive evaluation of expected value and likelihood, influenced by a range of factors identified in presenteeism research, from micro through to macro levels, which can be categorized into four main groups: personal, job-related, organizational, and environmental. Personal factors encompass factors such as work attitudes, self-efficacy (Cooper & Lu, Reference Cooper and Lu2016), perceived absence legitimacy, personality (Cooper & Lu, Reference Cooper and Lu2016; Johns, Reference Johns2010), affective wellbeing such as depression (Burton et al., Reference Burton, Pransky, Conti, Chen and Edington2004; McTernan et al., Reference McTernan, Dollard and LaMontagne2013), stress, and past absenteeism/presenteeism experience (Matinez & Ferreira, Reference Martinez and Ferreira2012). Job-related variables include factors such as role demands, time pressure, and adjustment latitude, in addition to interpersonal factors such as supervisor support and work–family conflict (Lohaus & Habermann, Reference Lohaus and Habermann2019). Organizational factors include factors such as absence policy (Chatterji & Tilley, Reference Chatterji and Tilley2002; Irvine, Reference Irvine2011), reward systems, workplace norms (Dew et al., Reference Dew, Keefe and Small2005; McKevitt & Morgan, Reference McKevitt and Morgan1997), and job security (Aronsson & Gustafsson, Reference Aronsson and Gustafsson2005; Prater & Smith, Reference Prater and Smith2011; Widera et al., Reference Widera, Chang and Chen2010). Finally, environmental factors include influences of macro factors such as national culture (Cooper & Lu, Reference Cooper and Lu2016) and economic climate (Kristensen, Reference Kristensen1991).
Further research is needed to tease out the complex nature via which these factors influence the evaluation of options, but it is clear that some are antecedents (e.g., stress, depression) while others are likely to be moderators and/or mediators (e.g., self-efficacy, work attitudes, organizational commitment). Furthermore, it is feasible that some factors may act as an antecedent in one circumstance but a moderator in another, depending on the health condition. For instance, stress could be the trigger for presenteeism/absenteeism in some circumstances, or a moderator in another where the main trigger is another (e.g., physical) health condition, but the impact of stress reduces the threshold at which an individual deems absenteeism to be necessary. Equally, as already discussed, macro factors may have a stronger influence than we might assume. For example, individuals with high job security may still choose to go to work when they are experiencing ill health because cultural norms encourage working through illness. Furthermore, because many of these influencing variables are situational or context-specific, these judgments may vary between individuals and within individuals for different ill-health spells.
Following decision field theory (Busemeyer & Townsend, Reference Busemeyer and Townsend1993; Busemeyer & Johnson, Reference Busemeyer, Johnson, Koehler and Harvey2004), evaluation of each option in terms of desired and expected outcomes may involve switching between alternatives, considering the consequences of each alternative over a period of time. Given the importance of social norms, consequences (both positive and negative) will be evaluated with regard to one’s self and in terms of others’ interests. For example, sickness absence would give me time to rest and may speed my recovery; however, this may result in additional workload for my colleagues which may cause animosity, which is then compared against the individual’s motives and goals.
Arguably, this is the stage where decision-making theory has most to offer, with a number of theories offering insights into how such judgments are influenced. Prospect theory (Kahneman & Tversky, Reference Kahneman and Tversky1979), for instance, suggests that people are likely to choose certain gains over the probability of losses if the difference between gains and losses is relatively small (risk aversion), whilst if facing certain losses, they will choose the probability of losses over the certain losses (risk seeking). In addition, expectancy theory helps us to understand how anticipated outcomes might combine with an individual’s goals and objectives to form the judgments which lead to determination of the final choice. In simplistic terms, for instance, employees who value financial stability or favorable relationships with colleagues and supervisors as desired outcomes are likely to choose presenteeism. However, given those desired outcomes, this may potentially become dysfunctional presenteeism (Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020), depending on the health condition and nature of the work demands. In contrast, individuals who place recovery as the primary desired outcome may enact absenteeism, in order to provide rest in order to recover from their illnesses, if their stage 2 assessment concluded that their work demands were insufficiently adaptable. The individual-desired outcomes differentiate the courses of action, informed by personal values. It is important to note that macro-level influences such as national culture and work climate norms also influence outcomes, whether this is directly through internalization of these values or indirectly through conformity. For example, individuals who work within countries or even organizations where long working hours and commitment to work (above all) are valued highly are more likely to select presenteeism, as a responsible act towards their employer and their colleagues (Cooper & Lu, Reference Cooper and Lu2016; Ruhle et al., Reference Ruhle, Breitsohl, Aboagye, Baba, Biron, Correia-Leal, Dietz, Ferreira, Gerich, Johns, Karanika-Murray, Lohaus, Løkke, Lopes, Martinez, Miraglia, Muschalla, Poethke, Sarwat, Schade, Steidelmüller, Vinberg, Whysall and Yang2019).
Comparisons of likely consequences will reach a preference state once the desirability of action passes a threshold (Busemeyer & Johnson, Reference Busemeyer, Johnson, Koehler and Harvey2004), and consequently this action is chosen. As discussed, given the range of potential options resulting from different levels of role/work adaptability, the discretionary amount of employee effort exerted, or even time spent working during any given working day, there are a range of different types of presenteeism (as characterized in the health-performance framework of presenteeism; Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020) that may be enacted. Thus, this is not a simple binary decision between absenteeism and presenteeism, but one between sickness absence without any work engagement (bearing in mind that some individuals may still undertake some work duties, such as checking emails, despite officially having taken sickness absence, thereby enacting presenteeism whilst on sick leave) and a range of sickness presenteeism behaviors, from working while ill yet maintaining full productivity, to working at limited capacity and/or on limited duties/hours, to being physically present but completely unproductive.
Stage 4: Feedback
Stage 4 is characterized by an evaluation of the efficacy of the choice made, which depending on the duration of illness may take place during illness and/or after the health event has subsided: did I make the right decision? and/or do I need to reconsider my decision? As discussed, feedback plays an important role in effective decision-making, in terms of evaluating the appropriateness of the selected option for the situation, assessing the extent to which the intended outcomes were achieved, and identifying links between actions and consequences. Feedback is essential in order to adapt behavior (Hardman, Reference Hardman2009) to external demands and changing circumstances, helping the individual to learn through this process and reinforce (positive feedback) or inhibit (negative feedback) specific decisions in the future (Verharen et al., Reference Verharen, Adan and Vanderschuren2019). This is consistent with evidence that people make decisions based on their past experience in similar situations (Verharen et al., Reference Verharen, Adan and Vanderschuren2019), with reinforced behaviors being most likely to be repeated while punished behaviors would be ceased. Evaluating the trade-offs between resources, demands, and expected outcomes is an essential part of the feedback mechanism for presenteeism. Intended and unintended consequences (at both the individual and organizational level, Lohaus & Habermann, Reference Lohaus and Habermann2019) will feed into the decision-making process in different ways, consciously and prospectively or unconsciously and retrospectively. Critically, feedback may help to adjust dysfunctional behavior towards more functional presenteeism. It is possible that through self and/or others’ feedback, individuals reconsider their health capacities and work tasks and through this process move between the quadrants described in the health-performance framework (Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020) .
Directions for Further Research
As described at the outset, with this process model, we hope to help build the foundations and empirical work that will enrich our understanding of presenteeism behavior, support evidence-based practice, and offer directions for further research. Consequently, we offer an initial integration of presenteeism research and decision-making theory, which requires empirical testing and subsequent honing to validate and refine the clustering of the key elements of the decision-making process into the stages outlined.
First, further research is needed to understand which and how the range of inputs identified in presenteeism research (i.e., from micro through to macro levels, and as four main groups of personal, interpersonal, organizational, and environmental factors) impact on each of the stages of decision-making. For example, how do different factors inform judgments around expected value and likelihood in the evaluation of options? Or how does the interaction between work demands and health condition shape the importance placed on different consequences?
In addition, we feel that future research would advantageously be directed towards exploring the extent to which instinctive (system 1) and more analytical thinking (system 2) (Kahneman, Reference Kahneman2012) influences the decision-making process, at which stage(s), and to what effect. For instance, the influence of heuristics on the framing of alternatives is particularly important. Specifically, the influence of deep-rooted assumptions or attributions held by individuals regarding the reciprocal relationship between work and health (for instance, an implicit belief that work is detrimental to health), which is likely to influence whether both options are even given due consideration in certain circumstances.
Furthermore, we also recognize that these modes of thinking are likely to combine personal preferences, attitudes, and values, on the one hand, against what the individual believes that they should do according to formal and informal rules, norms, and expectations. Thus, although the presenteeism behavior is preceded by a decision-making process and although presenteeism is a voluntary behavior (Karanika-Murray et al., Reference Karanika-Murray, Pontes, Griffiths and Biron2015), external pressures such as punitive attendance policies or an attendance culture of the workplace may make this choice “imposed”. Further research, therefore, should explore the interaction between internal (individual) and external (e.g., organizational or cultural) influences on the presenteeism decision-making process.
Finally, as the health-performance framework of presenteeism (Karanika-Murray & Biron, Reference Karanika-Murray and Biron2020) suggests, depending on whether the concern is weighted more towards supporting health or supporting performance, different types of presenteeism may emerge. The essential choice between prioritizing health or performance may be a most immediate concern that has implications for both recovery and performance. Consequently, further research should explore the decision-making process in relation not only to presenteeism–absenteeism, but also at the more nuanced level of functional, dysfunction, and therapeutic types of presenteeism and how these evolve until the presentee is ready to engage with work at full capacity.
Conclusions
The question of how individuals make decisions to attend or not to attend work when they are experiencing ill health is critical to effective management of employee health and productivity, providing the basis for understanding when and how one might intervene to help maximize those decisions. Thus, we hope that this model of the absenteeism–presenteeism decision-making process will help to build upon the limited amount of conceptual work in the field and help not only to explain but also to optimize the decision-making process. Greater understanding of the decision-making process regarding presenteeism is of not only high practical value, empowering better interventions to promote health in the workplace, but also of theoretical significance. By integrating presenteeism research with decision-making theory, we provide the foundations of a process model that outlines how the decision to enact presenteeism may unfold, incorporating the factors and correlates influencing this decision and evaluation of alternatives and consequences. Consequently, in outlining this conceptual model, we hope to enrich understanding of the decision-making process of presenteeism, as well as inspire future empirical research to test these propositions. Ultimately, these will help to promote work-related health and wellbeing, facilitate a more positive work experience for employees, and, by optimizing the health-productivity trade-off, promote organizational productivity.

