
Introduction
The following exercise is a case study of a girl (‘Rachel’) with cleft palate who was studied by Howard (Reference Howard1993). Rachel has grossly impaired speech and a severely reduced phonological system. Yet, she retains a high level of intelligibility. Her speech disorder has only been minimally responsive to prolonged therapy. The case study is presented in five sections: primer on cleft lip and palate; speech, language and hearing in cleft lip and palate; client history; focus on phonological analysis – part 1; and focus on phonological analysis – part 2.
Primer on cleft lip and palate
Cleft lip and palate is a congenital malformation of the upper lip and gum and hard and soft palates. A cleft of the lip can be complete, extending through the lip and into the nose, or incomplete, involving a variable degree of notching of the lip. A cleft lip may be unilateral or bilateral as is shown in Figure 1.1. A cleft of the palate may also be complete or incomplete. In a complete palatal cleft, the cleft extends the full length of the palate. In an incomplete palatal cleft, the cleft may involve just the uvula and soft palate. A palatal cleft may also be submucous (see Case study 2 for further discussion). Several methods of classifying cleft lip and palate have been proposed. A system that continues to be used in many cleft centres is the one proposed by Kernahan and Stark (Reference Kernahan and Stark1958). This system recognises the embryological division of the primary and secondary palates at the incisive foramen. If a palatal cleft occurs in front of the incisive foramen, it is called a primary palate or prepalate cleft. If a palatal cleft occurs behind the incisive foramen, it is called a secondary palate or simply palate cleft. Primary palate clefts may be unilateral (left or right), bilateral or median. Figure 1.2 shows different types of palatal clefts.
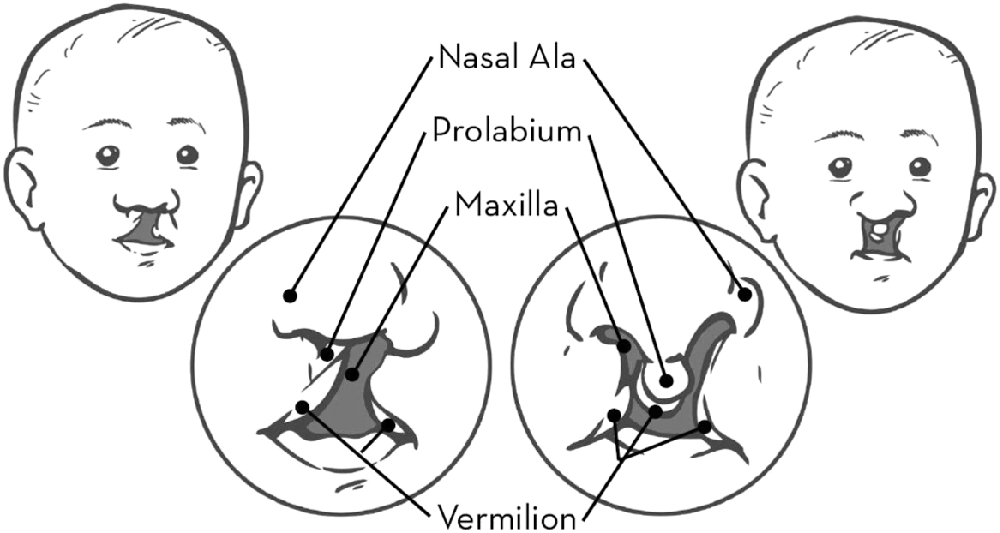
Figure 1.1 Unilateral and bilateral cleft lip and nose.
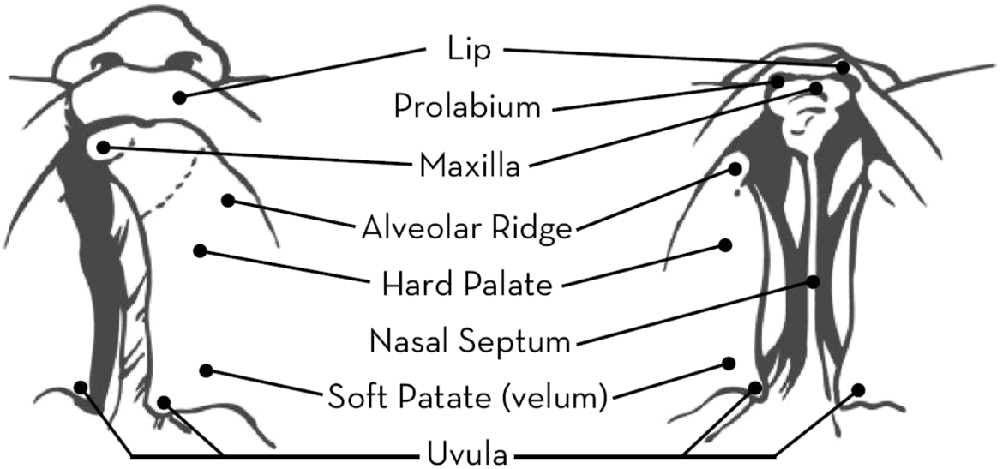
Figure 1.2 Unilateral and bilateral cleft palate.
Some forms of cleft are more common than others. Cleft lip and palate is the most common diagnosis, accounting for 46% of cases. Isolated cleft palate and isolated cleft lip account for 33% and 21% of cases, respectively. Unilateral clefts are nine times as common as bilateral clefts. They also occur twice as frequently on the left side than on the right (Hopper et al., Reference Hopper, Cutting, Grayson and Thorne2007). The epidemiology of cleft lip and palate has been extensively investigated. Matthews et al. (Reference Matthews, Oddone-Paolucci and Harrop2015) examined the epidemiology of cleft lip and palate in Canada between 1998 and 2007. The mean birth prevalence was 0.82 per 1,000 live births for cleft lip with or without cleft palate, and 0.58 per 1,000 live births for cleft palate. Cleft lip with or without cleft palate was significantly higher in boys, with a boy to girl ratio of 1.75:1. Cleft palate was significantly greater in girls, with a boy to girl ratio in 2007 of 0.59:1. The incidence of oral clefts varies among different ethnicities. Saad et al. (Reference Saad, Parina, Tokin, Chang and Gosman2014) found that the incidence of any cleft disease was highest in the white (non-Hispanic) population in the state of California at 16.2. Lower incidence rates were reported in the Hispanic population (12.26), Asian/Pacific Islanders (11.57), the African American population (8.9) and the Native American population (8.15).
The exact causes of cleft lip and palate are still unknown. What is clear is that genetic factors and environmental teratogens increase the likelihood that a child will develop a cleft. Several genes have been implicated in the aetiology of orofacial clefts (Simioni et al., Reference Simioni, Araujo, Monlleo, Maurer-Morelli and Gil-da-Silva-Lopes2015). Cleft lip and palate is also a clinical feature of many genetic syndromes. The most common syndrome associated with cleft lip and palate is van der Woude syndrome. Isolated cleft palate is most commonly associated with microdeletions of chromosome 21, resulting in velocardiofacial, DiGeorge, or conotruncal anomaly syndromes (Hopper et al., Reference Hopper, Cutting, Grayson and Thorne2007). Several teratogens and other environmental factors have been implicated in the aetiology of cleft lip and palate. Reduced folic acid levels, alcohol consumption, active and passive smoking, and antiepileptic drugs (e.g. topiramate) have all been associated with non-syndromic cleft lip and palate (Bezerra et al., Reference Bezerra, Oliveira, Soares, Cardoso, Ururahy, Neto, Lima-Neto, Luchessi, Silbiger, Fajardo, Oliveira, Almeida, Hirata, Rezende and Hirata2015; Margulis et al., Reference Margulis, Mitchell, Gilboa, Werler, Mittleman, Glynn and Hernandez-Diaz2012; Sabbagh et al., Reference Sabbagh, Hassan, Innes, Elkodary, Little and Mossey2015).
Unit 1.1 Primer on cleft lip and palate
(1) Respond with true or false to each of the following statements about cleft lip and palate:
Cleft lip and palate is an embryological malformation that arises in the first trimester of pregnancy.
Cleft lip and palate is a clinical feature of Pierre Robin syndrome.
An isolated cleft palate is more common in boys than in girls.
Cleft lip and palate is a clinical feature of Down's syndrome.
A bilateral cleft lip results in isolation of the prolabium.
(2) A cleft of the palate can be submucous in nature. Describe this type of cleft.
(3) Why do you think it is important for speech-language pathologists to know if a child has a syndromic cleft of the palate?
(4) There is considerable discussion about the optimal timing of surgical repair of a cleft of the palate. What two factors are central to the debate about the merits and disadvantages of early versus late palatal surgery?
(5) On account of its embryological significance, the incisive foramen is an important anatomical landmark in the classification of cleft lip and palate. Which of the following statements is true of the incisive foramen?
The incisive foramen is located in the maxilla bone.
The incisive foramen transmits blood vessels between the nasal cavities.
The incisive foramen transmits blood vessels and nerves between the nasal and oral cavities.
The incisive foramen is located in the midline of the palate posterior to the central incisors.
Speech, language and hearing in cleft lip and palate
Speech-language pathologists and audiologists must assess and treat the speech, language and hearing impairments that occur in cleft lip and palate. The primary speech defect is hypernasal speech related to velopharyngeal incompetence, although abnormal dentition and the presence of fistulae can also have phonetic consequences during speech production. Phonetic anomalies may have an adverse impact on a child's developing sound system (i.e. phonology). For example, the child who adopts a backed pattern of articulation in an effort to achieve closure and a build-up of air pressure in the vocal tract may eventually adopt backing as an organising principle within his system of sound contrasts. Such a child has a phonological disorder as well as a phonetic disorder. In a study of 80 children aged 6–15 years with cleft lip and palate, Albustanji et al. (Reference Albustanji, Albustanji, Hegazi and Amayreh2014) reported speech abnormalities including articulation and resonance deficits in 74% of subjects. Productive phonological processes in these children were consonant backing, final consonant deletion, gliding and stopping.
Although speech can improve following palatal surgery, phonetic and phonological defects may persist for many years. Nyberg et al. (Reference Nyberg, Peterson and Lohmander2014) examined the speech of 69 children who had a one-stage palatal repair at a mean age of 13 months. At 5 years of age, more than mild hypernasality, weak pressure consonants and perceived incompetent velopharyngeal function were present in 19 to 22% of children. This improved to less than 5% at 10 years of age. Audible nasal air leakage was present in 23% at 5 years and did not improve by 10 years. Frequent or persistent compensatory articulation was present in 30% at 5 years of age and in 6% at 10 years. At 5 years, 57% of children gave an impression of normal speech. This increased to 89% at 10 years. A high prevalence of distorted /s/ was present in these children at 5 and 10 years of age.
Children with cleft lip and palate often experience expressive language delay. Morris and Ozanne (Reference Morris and Ozanne2003) reported delayed expressive language in 9 of 20 cleft children aged 3 years. Eight of these children achieved a mean length of utterance (MLU) which was below average for their age. There is considerable evidence of delayed lexical development in children with cleft palate. Hardin-Jones and Chapman (Reference Hardin-Jones and Chapman2014) found that the size of the expressive lexicon of toddlers with cleft palate was significantly smaller than that of a noncleft group at 21 and 27 months of age. Discourse deficits have also been reported in children with cleft palate. Klintö et al. (Reference Klintö, Salameh and Lohmander2015) examined narrative retelling in 29 children with unilateral cleft lip and palate. An information score below 1 standard deviation from the norm value was obtained by 65.5% of these children. This compared with 30% in a comparison group of children. Several studies have found evidence of reading impairments in children with cleft palate. Conrad et al. (Reference Conrad, McCoy, De Volder, Richman and Nopoulos2014) found that subjects with non-syndromic cleft of the lip and/or palate performed significantly worse on a test of word reading than control subjects. Word reading deficits were not associated with measures of speech or hearing, but were correlated with auditory memory impairments.
Hearing loss is commonly found in children with cleft palate. In a retrospective audit of 123 newborns with cleft deformities, Tan et al. (Reference Tan, Hee, Yeoh, Lim, Tan, Yeow and Daniel2014) reported the incidence of hearing loss to be 24.4%. This was significantly higher than the hospital incidence of 0.3%. Hearing loss is most often conductive in nature and is associated with the development of otitis media with effusion. However, sensorineural hearing loss can also occur, particularly in children with syndromic cleft palate. Ventilation tube insertion is beneficial to the recovery of hearing in children with cleft palate and otitis media with effusion (Kuo et al., Reference Kuo, Tsao, Cheng, Lien, Hsu, Huang and Shiao2014). However, even after the placement of tubes, hearing loss may persist. Chen et al. (Reference Chen, Messner and Curtin2008) reported that of 30 newborns who failed hearing screening and had tympanostomy tubes placed, 43% had persistent hearing loss. Factors, which predicted persistent hearing loss, were cleft palate alone, female infants and the presence of an associated syndrome.
Unit 1.2 Speech, language and hearing in cleft lip and palate
(1) Which of the following factors is associated with velopharyngeal incompetence in children with cleft palate?
(2) Explain why the oral plosives /p, b, t, d, k, g/ are often substituted by the glottal stop /ʔ/ in the speech of children with cleft palate.
(3) In their study of the expressive lexicon in children with cleft palate, Hardin-Jones and Chapman (Reference Hardin-Jones and Chapman2014) reported that toddlers with cleft palate produced significantly more words beginning with sonorants and fewer words beginning with obstruents in their spontaneous speech samples. Why do you think this is the case?
(4) Give three reasons why children with cleft palate are at risk of language delay.
(5) Respond with true or false to each of the following statements about otitis media with effusion (OME) in children with cleft palate:
Client history
Rachel is 6 years old. She was born 11 weeks prematurely with a central cleft of the hard and soft palates. At 2;2 years, she underwent surgical repair of her palatal cleft. Rachel has a severe speech disorder, although her receptive language and expressive language have developed normally. Rachel has a history of fluctuating, mild to moderate, conductive hearing loss (average 45–55 dB). At 3;0 years, grommets were inserted. These were inserted again at 4;0 years. Auditory ability improved significantly following grommet insertion. At 5;11 years, T-tubes were inserted with reported improvements in hearing levels. Notwithstanding improvements in hearing, Rachel's performance in assessments of auditory discrimination for speech sounds remained inconsistent. There was no evidence of either oral apraxia or developmental apraxia of speech.
Rachel had received speech therapy for approximately three years by the time of the study. However, her speech problems had remained largely resistant to change and little progress had been made in therapy. There was also concern that Rachel had reached a plateau and that any further change in her speech would be difficult for her to achieve. Rachel had deficits across several aspects of speech production. She had difficulty initiating, maintaining and coordinating phonation. Her voice was breathy and she displayed high pitch. In relation to resonance, she exhibited hypernasality, nasal emission and nasal friction. A pharyngoplasty was performed at 5;5 years. However, it had had little effect in reducing her nasal emission. In terms of articulation, Rachel displayed glottalisation of consonants. There was also a lack of alveolar and post-alveolar segments in her speech. Rachel exhibited greater difficulty with the articulation of obstruents than nasals and approximants.
Unit 1.3 Client history
(1) Which feature of Rachel's history is frequently found in newborns with oral clefts?
(2) Is Rachel's cleft type consistent with the findings of studies of sex differences in clefting?
(3) Respond with true or false to each of the following statements about grommets and T-tubes:
Both devices are used to treat Eustachian-tubal insufficiency.
Grommets remain in situ for longer than T-tubes.
Both devices reside in the middle ear.
Both devices are naturally extruded by the tympanic membrane.
T-tubes are used when multiple grommet insertions have failed to provide adequate middle ear ventilation.
(4) Rachel had a breathy voice quality and other phonatory disturbances. Why are children with cleft palate at an increased risk of voice disorder?
(5) At 5;5 years, Rachel underwent a pharyngoplasty. Describe this procedure and state what it is intended to achieve.
Focus on phonological analysis – part 1
Audio- and video-recordings were made of Rachel's speech production during two clinical sessions over a period of five days. To obtain comprehensive coverage of the entire phonological system, the Sheffield Test of Phonetics and Phonology (Eastwood, Reference Eastwood1981) was used. The nearly 100 words from this test were supplemented by words recorded during spontaneous speech and picture description tasks. A detailed phonetic transcription of all words was completed. Symbols from the IPA and extensions to the IPA were used in the transcription. Following transcription, the PACS framework (Grunwell, Reference Grunwell1985) was used to carry out a phonological analysis of Rachel's speech. The data that was used in this analysis is examined in this unit and in the next unit.
Phonotactic structure
| glasses | [ˈɴᴡæç͋əç͋] |
| string | [ˈʩɁωɪɴ] |
| matches | [ˈmaɁjəħ͋] |
Oral–nasal contrast
| letter | [ˈɰeɁə] | nose | [ɴəʊҫ͋] |
| ladder | [ˈɰæɁə] | ring | [ʊɪɴ] |
| sugar | [ˈҫ͋ʊɁə] | fine | [f͉:aɪɴ] |
| down | [Ɂaʊɴ] | penny | [ˈp͡ʔeɴɪ] |
| dog | [ɁɒɁʰ] | singing | [ˈҫ͋ɪɴɪɴ] |
| cat | [ɁæɁʰ] | teaspoon | [ˈʔiҫ͋ᵬuɴ] |
Bilabials
| pig | [ʘɪʔʰ] | mud | [məʔʰ] |
| pen | [ʔeɴ] | mum | [məm] |
| tap | [ʔæʔ͡ʘ] | mouth | [maʊɵ] |
| paper | [ˈp͡ʔeɪp͡ʔə] | thumb | [ɵəm] |
| big | [mɪʔʰ] | jam | [ʔjæm] |
| baby | [ˈᵬeɪbɪ] | hammer | [ˈħæmə] |
| bike | [maɪʔʰ]/[ᵬaɪʔʰ] | shop | [ҫ͋jɒp̃ʰ] |
Unit 1.4 Focus on phonological analysis – part 1
(1) Describe the phonotactic structures of the words ‘glasses’, ‘string’ and ‘matches’. Is Rachel able to replicate these structures in her spoken productions? What does your answer to this question reveal about Rachel's phonological knowledge?
(2) Is Rachel able to maintain a broad oral–nasal contrast in her use of alveolar segments? Use examples from the above data to support your response.
(3) Is Rachel able to maintain a broad oral–nasal contrast in her use of velar segments? Use examples from the above data to support your response.
(4) Is there any similarity in the way in which Rachel realises alveolar and velar segments and the way in which she realises bilabial segments? What additional clue does Rachel provide for listeners to assist them in the identification of target bilabial segments? Use examples from the above data to support your response.
(5) Not all of Rachel's bilabial segments are realised as glottal stops. In what other ways are bilabial segments realised within her speech? What do most of these realisations have in common? One realisation is particularly unusual. Which one is it, and why do you think it occurs?
Focus on phonological analysis – part 2
Several other aspects of the manner of articulation were examined in Rachel's speech. They included her ability to signal the stop–fricative–approximant continuum and the stop–affricate continuum. These continua tell us something about Rachel's ability to signal the difference between open and close sounds and, in the case of the stop–affricate continuum, the timing of release of closure. Contrasts of place of articulation and the voicing of segments were also examined.
Stop–fricative–approximant continuum and stop–affricate continuum
| tap | [ʔæʔʰ] | zip | [ҫ͋ɪʔʘ] |
| down | [ʔaʊɴ] | cup | [ʔʊʔʰ] |
| chair | [ʔjɛə] | go | [ʔəʊ] |
| jam | [ʔjæm] | yes | [jɛʔ] |
| sock | [ҫ͋ɒʔʰ] | why | [waɪ] |
| shop | [ҫ͋jɒp̃ʰ] |
Place of articulation
| baby | [ƀeɪbɪ] | bucket | [ˈƀʊʔɪʔʰ] |
| toy | [ʔɔɪ] | Sue | [ç͋u] |
| cat | [ʔæʔʰ] | daddy | [ˈʔæʔɪ] |
| tap | [ʔæʔʘ] | dog | [ʔɒʔʰ] |
| paper | [p͡ʔeɪp͡ʔə] | sugar | [ˈç͋ɬʊʔə] |
| kick | [ʔɪʔʰ] | shoe | [ç̫͋u] |
Voicing
| pig | [ʘɪʔʰ] | bib | [ƀɪb̥ʰ] |
| baby | [ˈƀeɪbɪ] | tea | [ʔi] |
| letter | [ˈɰeʔə] | ladder | [ˈɰæʔə] |
| Sue | [ç͋u] | zoo | [ç͋u] |
| watch | [wɒʔç͋] | jam | [ʔjæm] |
| four | [f͉ɔ] | a van | [ə ˈf͈æɴ] |
| feather | [ˈf͉eʋə] | laughing | [ˈæf͉ɪɴ] |
| dig | [ʔɪʔʰ] | chair | [ʔjɛə] |
| key | [ʔi] | fridge | [fʋɪʔħ] |
| go | [ʔəʊ] | cover | [ˈʔʊʋə] |
Unit 1.5 Focus on phonological analysis – part 2
(1) Is Rachel able to signal a contrast between stop, fricative and approximant sounds? Use examples to illustrate how she signals this contrast.
(2) Does Rachel succeed in signalling a contrast between stops and affricates? Support your answer with examples from the above data.
(3) Prior to speech therapy, alveolar and postalveolar fricatives had pharyngeal realisations in Rachel's speech. Does Rachel effectively signal an alveolar–postalveolar contrast between these sounds following therapy? In what way does Rachel's post-therapy production of alveolar and postalveolar fricatives represent an improvement on her pre-therapy production?
(4) Is Rachel able to signal a voicing contrast for bilabial, alveolar and velar plosives? Does Rachel succeed in signalling a phonological contrast between /f/ and /v/?
(5) Which of the following statements best characterises Rachel's speech production?
Rachel is severely unintelligible on account of her use of segments that are phoneti-cally distant from target phonemes.
Rachel is severely unintelligible because of a lack of consistency in her use of phonemes.
Rachel is severely unintelligible because she is unable to signal a number of phonological contrasts in her speech.
Rachel is more intelligible than expected because she makes consistent use of phonetically deviant phonemes.
Rachel is more intelligible than expected because she is able to signal a contrast between plosive and fricative sounds.


