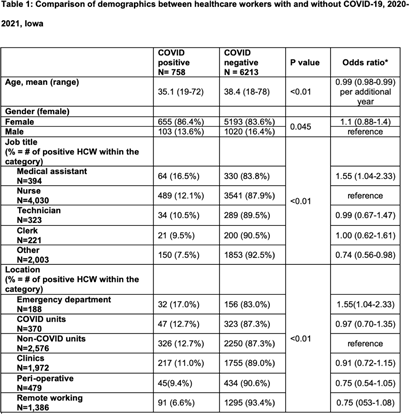
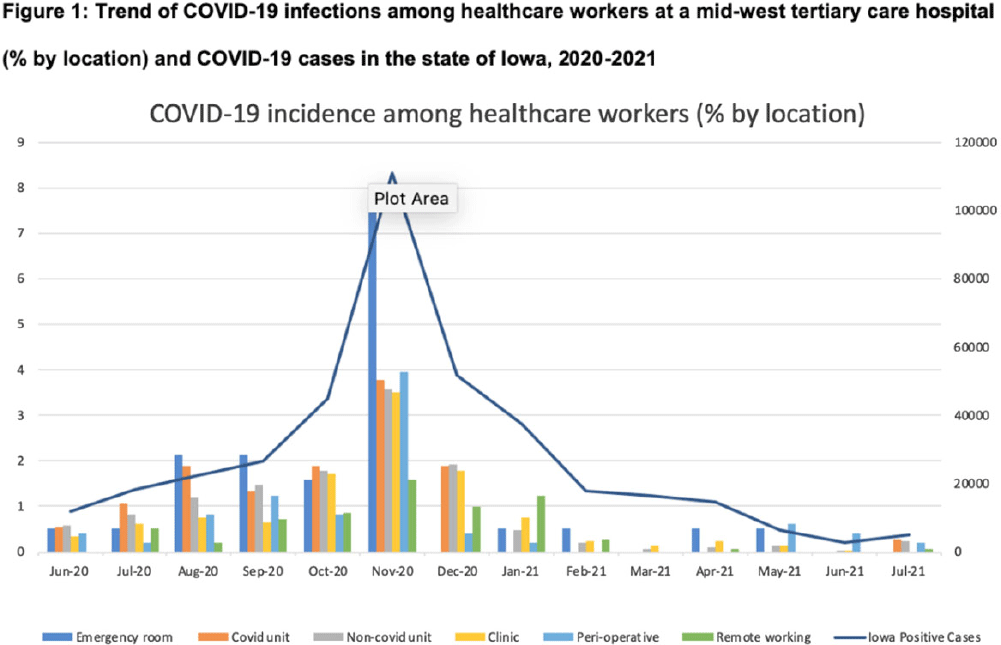
Background: Whether working on COVID-19 designated units put healthcare workers (HCWs) at higher risk of acquiring COVID-19 is not fully understood. We report trends of COVID-19 incidence among nonphysician HCWs and the association between the risk of acquiring COVID-19 and work location in the hospital. Methods: The University of Iowa Hospitals & Clinics (UIHC) is an 811-bed, academic medical center serving as a referral center for Iowa. We retrospectively collected COVID-19–associated data for nonphysician HCWs from Employee Health Clinic between June 1st 2020 and July 31th 2021. The data we abstracted included age, sex, job title, working location, history of COVID-19, and date of positive COVID-19 test if they had a history of COVID-19. We excluded HCWs who did not have a designated working location and those who worked on multiple units during the same shift (eg, medicine resident, hospitalist, etc) to assess the association between COVID-19 infections and working location. Job titles were divided into the following 5 categories: (1) nurse, (2) medical assistant (MA), (3) technician, (4) clerk, and (5) others (eg patient access, billing office, etc). Working locations were divided into the following 6 categories: (1) emergency department (ED), (2) COVID-19 unit, (3) non–COVID-19 unit, (4) Clinic, (5) perioperative units, and (6) remote work. Results: We identified 6,971 HCWs with work locations recorded. During the study period, 758 HCWs (10.8%) reported being diagnosed with COVID-19. Of these 758 COVID-19 cases, 658 (86.8%) were diagnosed before vaccines became available. The location with the highest COVID-19 incidence was the ED (17%), followed by both COVID-19 and non–COVID-19 units (12.7%), clinics (11.0%), perioperative units (9.4%) and remote work stations (6.6%, p Conclusions: Strict and special infection control strategies may be needed for HCWs in the ED, especially where vaccine uptake is low. The administrative control of HCWs working remotely may be associated with a lower incidence of COVID-19. Given that the difference in COVID-19 incidence among HCWs by location was lower and comparable after the availability of COVID-19 vaccines, facilities should make COVID-19 vaccination mandatory as a condition of employment for all HCWs, especially in areas where the COVID-19 incidence is high.
Funding: None
Disclosures: None
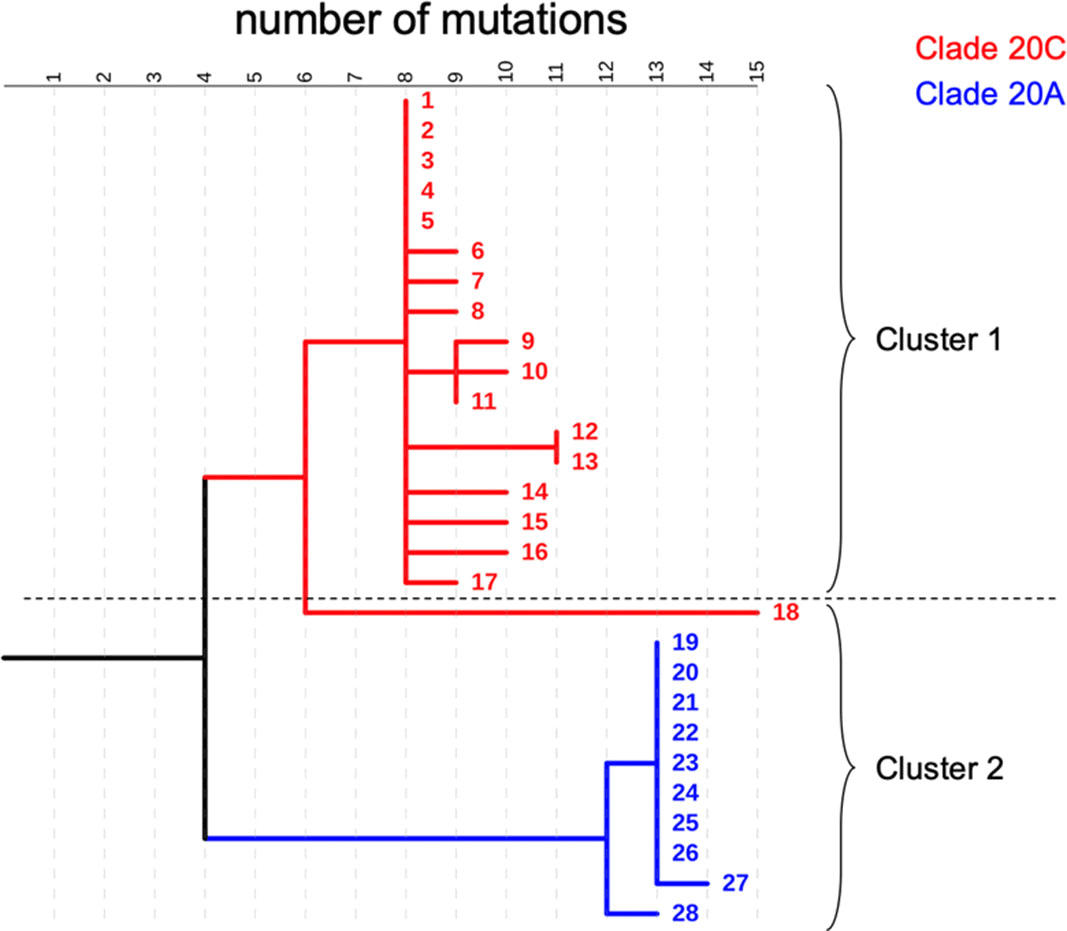
Background: COVID-19 in hospitalized patients may be the result of community acquisition or in-hospital transmission. Molecular epidemiology can help confirm hospital COVID-19 transmission and outbreaks. We describe large COVID-19 clusters identified in our hospital and apply molecular epidemiology to confirm outbreaks. Methods: The University of Iowa Hospitals and Clinics is an 811-bed academic medical center. We identified large clusters involving patients with hospital onset COVID-19 detected during March–October 2020. Large clusters included ≥10 individuals (patients, visitors, or HCWs) with a laboratory confirmed COVID-19 diagnosis (RT-PCR) and an epidemiologic link. Epidemiologic links were defined as hospitalization, work, or visiting in the same unit during the incubation or infectious period for the index case. Hospital onset was defined as a COVID-19 diagnosis ≥14 days from admission date. Admission screening has been conducted since May 2020 and serial testing (every 5 days) since July 2020. Nasopharyngeal swab specimens were retrieved for viral whole-genome sequencing (WGS). Cluster patients with a pairwise difference in ≤5 mutations were considered part of an outbreak. WGS was performed using Oxford Nanopore Technology and protocols from the ARTIC network. Results: We identified 2 large clusters involving patients with hospital-onset COVID-19. Cluster 1: 2 hospital-onset cases were identified in a medical-surgical unit in June 2020. Source and contact tracing revealed 4 additional patients, 1 visitor, and 13 employees with COVID-19. Median age for patients was 62 (range, 38–79), and all were male. In total, 17 samples (6 patients, 1 visitor, and 10 HCWs) were available for WGS. Cluster 2: A hospital-onset case was identified via serial testing in a non–COVID-19 intensive care unit in September 2020. Source investigation, contact tracing, and serial testing revealed 3 additional patients, and 8 HCWs. One HCW also had a community exposure. Patient median age was 60 years (range, 48–68) and all were male. In total, 11 samples (4 patients and 7 HCWs) were sequenced. Using WGS, cluster 1 was confirmed to be an outbreak: WGS showed 0–5 mutations in between samples. Cluster 2 was also an outbreak: WGS showed less diversity (0–3 mutations) and ruled out the HCW with a community exposure (20 mutations of difference). Conclusion: Whole-genome sequencing confirmed the outbreaks identified using classic epidemiologic methods. Serial testing allowed for early outbreak detection. Early outbreak detection and implementation of control measures may decrease outbreak size and genetic diversity.
Funding: No
Disclosures: None
Figure 1.