The Residential Educational Therapeutic Unit Accompany from Hospital Sant Joan de Déu Barcelona, is a device integrated into the public health network, intended for the comprehensive care of children and adolescents under 18 years of age who suffer from an illness complex mental disorder, at serious risk of becoming chronic and generating significant disabilities at a functional, cognitive and emotional level. It was a result from a joint venture between the Department of Social Rights and the Department of Health. The device was created to respond to the increase in behavioral problems and mental health disorders of children underguardianship.
General Objective
To improve the quality of life in the physical, mental and social spheres of vulnerable children and adolescents with serious complex mental pathology through a biopsychosocial and community care model that integrates health, social, family and educational care and which is aimed at the recovery of the person’s life project.
Specific Objectives
To offer intensive intervention, personalized and in a co-responsible manner, that is to say, that integrates the therapeutic, education, social services and child protection teams.
Promote the community and social reintegration avoiding stigmatization and social exclusion.
Improve the intra-family relationship and the burden perceived by caregivers.
Decrease the number of renunciations of parental authority of a minor.
The unit has a capacity for 28 beds: 23 places for children/adolescents underguardianship of the administration and 5 places for cases that are at risk of family claudication due to their therapeutic and educational needs.
There are 5 coexisting therapeutic units. The apartments are referred as ‘homes’ and their organization is designed to encourage the active participation of residents with the professionals who attend them.
The Unit has a multidisciplinary team made up of the following professionals: Psychyatrists, Nurses, clinical psychologists, Social Workers, Educational worker, nursing assistants, administrative.
- 110 children and adolescents have been taken care, with an average cumulative stay of 13 months. In all cases in which the family had the guardianship of the patient, family claudication has been avoided There is a 36% discharge of those patients under guardian that have returned to their original family home 100% of the cases have been linked to an educational center adapted to their needs or to a training project
Image:

Image 2:

Overall, the care model implemented by the population served in the Acompanya’m unit is positively evaluated. Since it provides an intensive and personalized care, treatment and intervention for children suffering from a serious mental disorder of high complexity. A comprehensive, personalized, interdisciplinary approach is offered, coordinated and co-responsible with educational, protection and social services.
None Declared
Stigma is one of the most important barriers to help-seeking, treating maintenance and recovery for people suffering mental disorders. These attitudes, when present in mental health workers, may have a negative effect on the quality of health care.
to evaluate the levels of stigma in a representative sample of mental health workers and to explore potential modifiable factors associated to stigma attitudes.
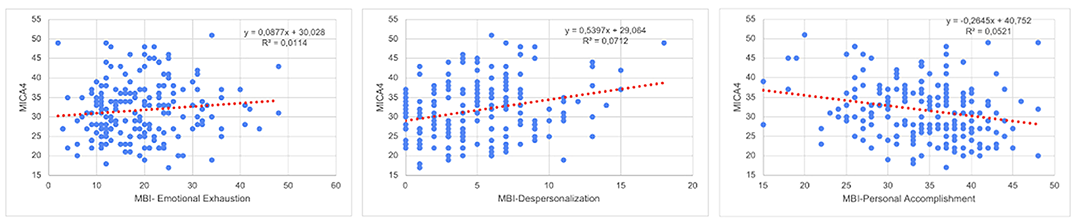
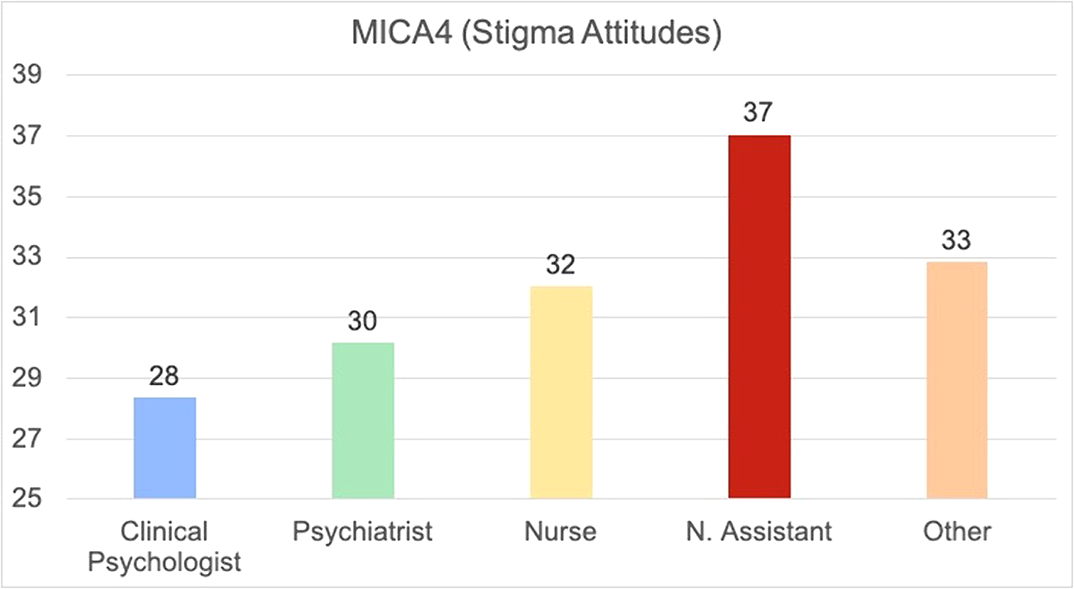
An online survey was conducted on the mental health workers of Castilla y León (Spain, 2409164 habs) while projecting the 2022 Mental Health Humanization plan in order to asses educational skills, burnout (Maschlach MBI), Professional Quiality of life (CVP-35) and Stigma attitudes (Mental Illness: Cinician’s Attitudes Scales, MICA4) together with sociodemographic and work position variables.
193 workers completed completed the survey. Stigma Attitude values of the sample were low (MICA4: 31.71; SD:7.3) and burnout were low or medium (medium Emotional Exhaustion: 19.22; SD8.89; low Depersonalization: 4.91; SD:3.61; Medium Personal Accomplishment: 34,17; 6.3). In the linear regression (R2=0.249; F:11,527; p<0,001), a lower Stigma was predicted by psychologist (Beta:0,207; p=0,003) or psychiatrist position (Beta:0,204; 0,005), Self-efficacy assessed by the item “I am qualified” in the CVP-35 (Beta:-10,144; p=0,023), and a higher stigma was predicted by nurse assistant position (Beta: -0.230; p=0.001), Depersonalization Burnout dimension (Beta:0,351; p<0,001) and years of service (Beta:0.148; p=0,023)
Some groups of mental workers are more vulnerable to develop stigma attitudes. These, may be increased by fatigue and burnout. Future interventions should determine if reducing burnout and increasing capacitation may be effective in stigma eradication
No significant relationships.
We characterize the star formation going on in the inner kiloparsec region of the galaxy NGC 1386 as derived from the analysis of a multiwavelength dataset covering the optical, near-IR and mid-IR at subarsec resolution. We detect 61 point sources, distributed in a ring of 960 pc radius around the center of the galaxy. From SED fitting we conclude that these are low mass ( ) young clusters, with age distributed from 1 to 10 Myr, with median at 3.6 Myr. Comparison of the Hα luminosity of the clusters derived from the Hα+[N ii] narrow band image with that expected from the fitted ionizing continuum shows that a large fraction of the ionizing photons escapes from the clusters. Moreover, a large fraction of these photons escapes from the regions around the star forming ring.
) young clusters, with age distributed from 1 to 10 Myr, with median at 3.6 Myr. Comparison of the Hα luminosity of the clusters derived from the Hα+[N ii] narrow band image with that expected from the fitted ionizing continuum shows that a large fraction of the ionizing photons escapes from the clusters. Moreover, a large fraction of these photons escapes from the regions around the star forming ring.

