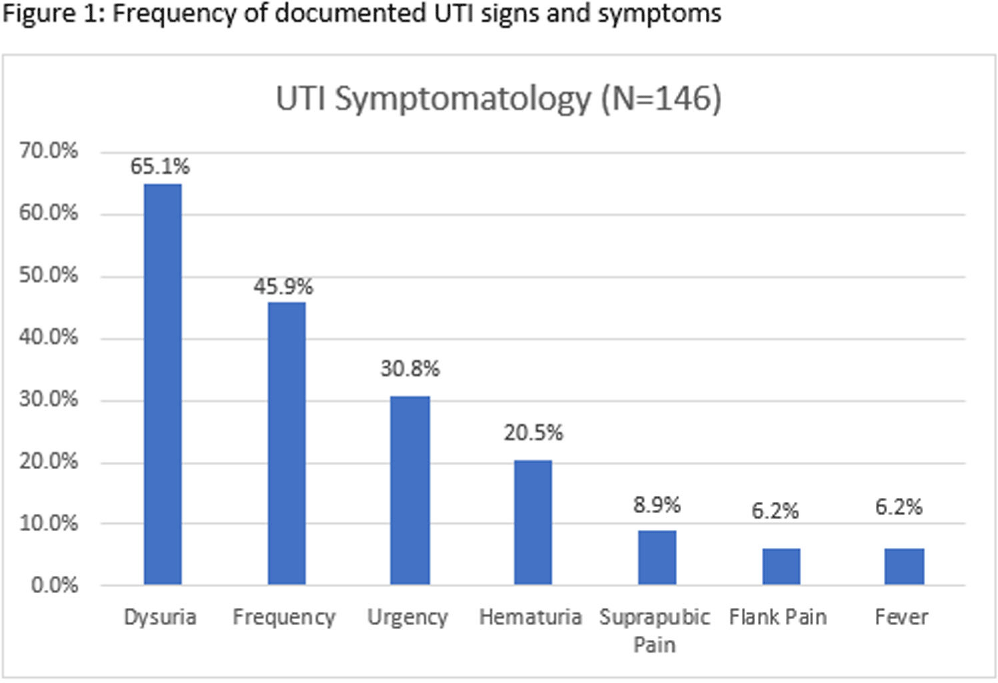
Background: Infectious Diseases Society of America guidelines recommend antibiotic prescribing for urinary tract infections (UTIs) when there is a positive culture and signs and symptoms of infection. Despite these guidelines, prescribing for asymptomatic bacteriuria remains prevalent. We conducted a chart review of UTI outpatient encounters to determine the prevalence of antibiotic prescribing as well as patient and provider factors associated with inappropriate prescribing for UTIs. Methods: Patients who were seen at any Department of Veterans Affairs (VA) outpatient clinic with a positive urine culture from 1/1/2019-12/31/2022 were evaluated for inclusion. Exclusion criteria were pregnancy, neutropenia, neurogenic bladder, spinal cord injury/disorder, chronic kidney disease stage III and above, and those undergoing urologic surgical procedures within 7 days. Inappropriate prescribing was defined as an antibiotic prescription given for UTI treatment when no signs or symptoms of infection were recorded during the patient encounter. Chi-square, Fisher’s exact and t-tests were used to evaluate the association between patient and provider characteristics and antibiotic prescribing. Results: Among 341 visits, most patients were male (70%), White (40%), older (mean age of 65.8 ± 15.9 years) and treated at an urban facility (57%). Antibiotics were prescribed for 67% (229/341) of visits. Of the 229 antibiotic courses prescribed, 119 (52%) were appropriate; issued to patients with > = 1 sign or symptom consistent with a urinary tract infection. The most common symptom recorded was dysuria, followed by frequency, urgency, and hematuria (Figure 1). The remaining 110 (48%) antibiotic prescriptions were inappropriate; given to patients without documented UTI-related signs or symptoms. The proportion of inappropriate prescribing was higher among advanced practice practitioners (39/56; 69%) compared to physicians (68/113; 60%; P < 0 .0001). Prescribing of an antibiotic did not differ by gender (p-value=0.3779), race (p-value=0.3972), age (p-value=0.7461) or urban versus rural geography (p-value=0.3647). Discussion: In outpatient clinics, nearly half of antibiotics prescribed to patients with a positive urine culture occurred in the absence of documented of signs or symptoms of a UTI. These results suggest that interventions to improve antibiotic use for UTI-related concerns in the outpatient setting should address UTI-related signs and symptoms as well as asymptomatic bacteriuria. Advanced practice practitioners were more likely to prescribe without documentation of relevant signs or symptoms than physicians. Improving meaningful documentation about the presence or absence of signs and symptoms of a UTI may help reduce inappropriate antibiotic prescriptions in the outpatient setting.
Disclosure: Robin Jump: Research support to my institution from Merck and Pfizer; Advisory boards for Pfizer
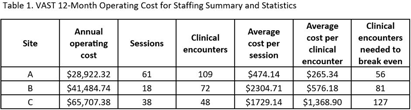
Background: In rural areas, antimicrobial stewardship programs often have limited access to infectious disease (ID) expertise. Videoconference Antimicrobial Stewardship Teams (VASTs) pair rural Veterans Affairs (VA) medical centers with an ID expert to discuss treatment of patients with concerns for infection. In a pilot study, VASTs were effective at improving antimicrobial use. Here, we evaluated 12-month operating costs for staffing for 3 VASTs. Methods: We used the following data to describe 12 months of clinical encounters for 3 VASTs operating from January 2022 – March 2023: the number of VAST sessions completed and clinical encounters; Current Procedural Terminology (CPT) codes associated with clinical encounters; session attendees (by role) and the time spent (percent effort) on VAST-related activities. The annual operating cost was based on the annual salaries and percent effort of VAST attendees. We used these characteristics combined with private-sector and Medicare reimbursements to evaluate the cost of implementation and number of clinical encounters needed to offset those costs (breakeven) for each site. Results: Three VASTs recorded 229 clinical encounters during 117 sessions (Table 1). Based on CPT codes, the approximate revenue per patient was $516.46. Site A, the only site to break even, had the most sessions and clinical encounters as well as the lowest operating costs. For Site B, a slight increase in the clinical encounters, which might be achieved by 3 additional VAST sessions, would help achieve breakeven. For Site C, increasing the number of clinical encounters to 3-4 per session would have helped their VAST break even without requiring a decrease in operating costs. Conclusions: The frequency of VAST sessions, volume of clinical encounters, and low operating costs all contributed the VAST at Site A achieving a financial break-even point within 12 months. Consideration of the potential number of clinical encounters and sessions will help other VASTs achieve financial sustainment, independent of cost-savings related to potential decreases in expenditures for antibiotics and antibiotic-related adverse events. These results also provide insight into possible adoption and diffusion of VAST-like programs in the Medicare hospital setting.
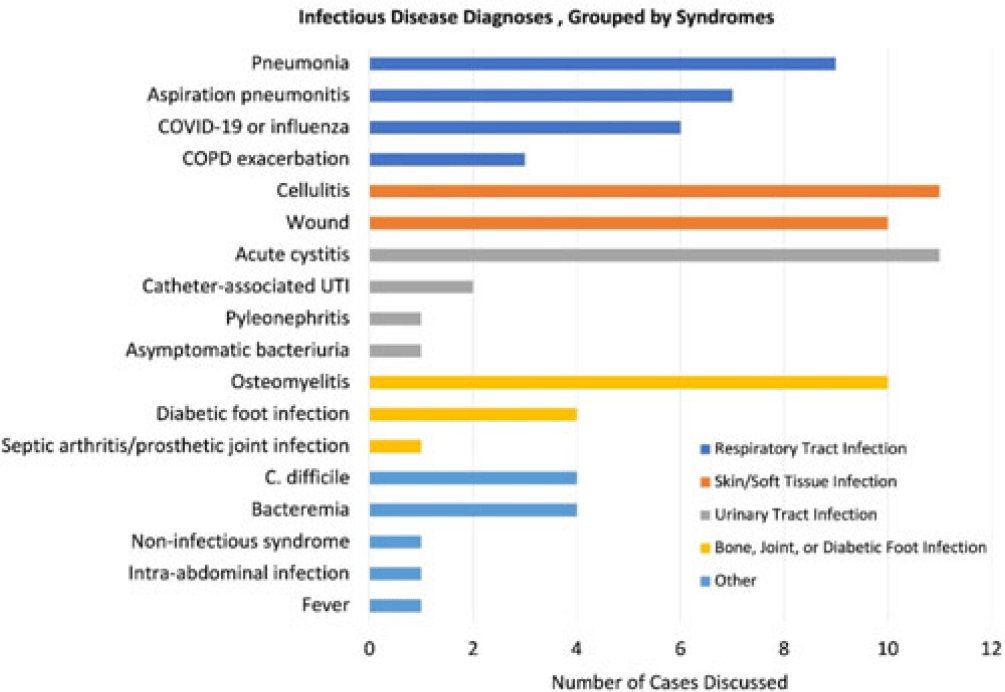
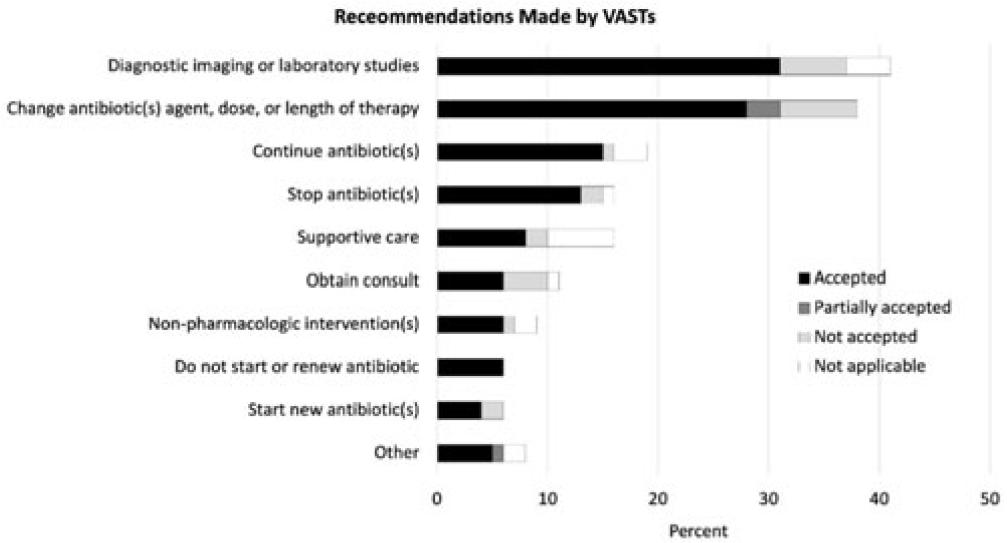
Background: Healthcare settings without access to infectious diseases experts may struggle to implement effective antibiotic stewardship programs. We previously described a successful pilot project using the Veterans Affairs (VA) telehealth system to form a Videoconference Antimicrobial Stewardship Team (VAST) that connected multidisciplinary teams from rural VA medical centers (VAMCs) with infectious diseases experts at geographically distant locations. VASTs discussed patients from the rural VAMC, with the overarching goal of supporting antibiotic stewardship. This project is currently ongoing. Here, we describe preliminary outcomes describing the cases discussed, recommendations made, and acceptance of those recommendations among 4 VASTs. Methods: Cases discussed at any of the 4 participating intervention sites were independently reviewed by study staff, noting the infectious disease diagnoses, recommendations made by infectious diseases experts and, when applicable, acceptance of those recommendations at the rural VAMC within 1 week. Discrepancies between independent reviewers were discussed and, when consensus could not be reached, discrepancies were discussed with an infectious diseases clinician. Results: The VASTs serving 4 different rural VAMCs discussed 96 cases involving 92 patients. Overall, infection of the respiratory tract was the most common syndrome discussed by VASTs (Fig. 1). The most common specific diagnoses among discussed cases were cellulitis (n = 11), acute cystitis (n = 11), wounds (n = 11), and osteomyelitis (n = 10). Of 172 recommendations, 41 (24%) related to diagnostic imaging or laboratory results and 38 (22%) were to change the antibiotic agent, dose, or duration (Fig. 2). Of the 151 recommendations that could be assessed via chart review, 122 (81%) were accepted within 1 week. Conclusions: These findings indicate successful implementation of telehealth to connect clinicians at rural VAMCs with an offsite infectious diseases expert. The cases represented an array of common infectious syndromes. The most frequent recommendations pertained to getting additional diagnostic information and to adjusting, but not stopping, antibiotic therapy. These results suggest that many of the cases discussed warrant antibiotics and that VASTs may use the results of diagnostic studies to tailor that therapy. The high rate of acceptance suggests that the VASTs are affecting patient care. Future work will describe VAST implementation at 4 additional VAMCs, and we will assess whether using telehealth to disseminate infectious diseases expertise to rural VAMCs supports changes in antibiotic use that align with principles of antimicrobial stewardship.
Disclosures: None
Objectives: To address the importation of multi-drug-resistant organisms (MDROs) when a colonized or infected patient is transferred from another VA facility, the Veterans Health Administration (VHA) launched the Inpatient Pathogen Tracker (IPT) in 2020. IPT tracks MDRO-infected/colonized patients and alerts MDRO Program Coordinators (MPCs) and Infection Preventionists (IPs) when such patients are admitted to their facility to facilitate rapid identification and isolation of infected/colonized patients. IPT usage has been low during initial rollout (32.5%). The VHA and the CARRIAGE QUERI Program developed targeted implementation strategies to increase utilization of IPT’s second iteration, VA Bug Alert (VABA). Methods: Familiarity with IPT was assessed via pre-education survey (3/2022). All sites received standard VABA implementation including: 1) adaptation of VABA features based on end-user feedback (completed 4/2022), 2) development and delivery of an educational module regarding the revised tool (completed 4/2022), and 3) internal facilitation from the VHA MDRO Program Office (ongoing) (see Figure for all key timepoints). Intent to register for VABA was assessed via post-education survey (4-5/2022). Sites (125 eligible) not registered for VABA by 6/1/2022 were randomly assigned to receive one of two conditions from 6/2022–8/2022: continued standard implementation alone or enhanced implementation. Enhanced implementation added the following to standard implementation: 1) audit and feedback reports and 2) external facilitation, including interviews and education about VABA. We compared the number of sites with ≥1 MPC/IP registered for VABA to-date between implementation conditions. Results: Pre-education survey. 168 MPC/IPs across 117 sites responded (94% of eligible sites). Among respondents, 25% had used IPT, 35.1% were familiar with but had not used IPT, and 39.9% were unfamiliar with IPT. Post-education survey. 93 MPC/IPs across 80 sites responded (59% of eligible sites). Of these, 81.7% said they planned to register for VABA, 4.3% said they would not register, and 14.0% said they were unsure. Post-6/1/2022 Registrations. By 6/1/2022, 71% of sites had ≥1 registered VABA user. Of the 28 unregistered sites eligible for enhanced implementation, thirteen were assigned to receive enhanced implementation, and fifteen were assigned to receive continued standard implementation. Eight sites in the enhanced implementation condition (61.5%) registered for VABA. Seven standard-implementation-only sites (46.7%) registered. The number of registered sites did not significantly differ by implementation condition (Fisher’s exact p=0.476). Conclusions: Standard and enhanced implementation were equally effective at encouraging VABA registration, suggesting that allocating resources to enhanced implementation may not be necessary.
Disclosures: None.


