Elimination disorders (ED) include enuresis, defined as wetting from 5 years, and encopresis, defined as soiling from 4 years onwards after organic causes are excluded. They are highly prevalent in childhood and often associated with clinically relevant comorbid psychological disorders. However, no systematic review or meta-analysis examines their co-occurrence with internalizing and externalizing problems in children.
The aim of this study is to determine if, and to what extent, children with ED show higher internalizing and externalizing problems than their healthy peers.
A multistep literature search was performed from database inception until May 1st, 2022. PRISMA/MOOSE-compliant systematic review (PROSPERO: CRD42022303555) were used to identify studies reporting on internalizing and/or externalizing symptoms in children with an ED and a healthy control (HC) group. First, a systematic review was provided. Second, where data allowed for it, a quantitative meta-analysis using random effects model was conducted to analyze the differences between the ED and the HC groups for internalizing and externalizing symptoms. Effect size was standardized mean difference. Meta-regression analyses were conducted to examine the effect of sex, age, and study quality. Funnel plots were used to detect a publication bias. Where found, the trim and fill method was used to correct it.
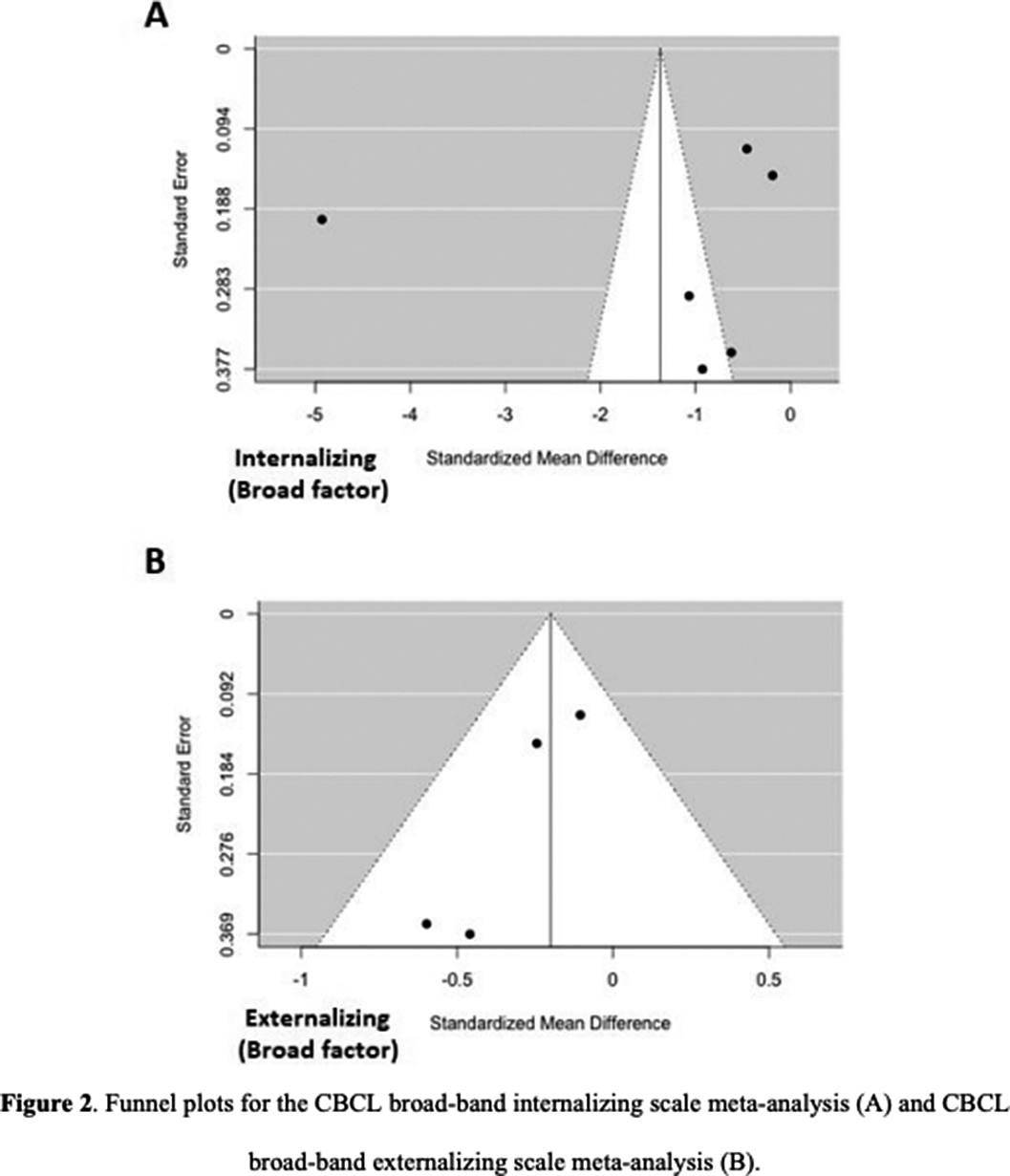
36 articles were included, 32 of them reporting on enuresis (n=3244; mean age=9.4; SD=3.4; 43.84% female) and 7 of them on encopresis (n=214; mean age=8.6; SD=2.3; 36.24% female) [Image 1]. The ED group presented significantly lower self-concept (ES:0.42; 95%CI: [0.08;9.76]; p=0.017) and higher symptom scores for thought problems (ES:-0.26; 95%CI: [-0.43;-0.09]; p=0.003), externalizing symptoms (ES:-0.20; 95%CI: [-0.37;-0.03]; p=0.020), attention problems (ES:-0.37; 95%CI: [-0.51;-0.22]; p=0.0001), aggressive behaviour (ES:-0.33; 95%CI: [-0.62;-0.04]; p=0.025) and social problems (ES: 0.39; 95%CI: [-0.58;-0.21]; p=0.0001) [Image 2]. Significant publication biases were found across several of the studied domains [Image 3]. No significant effect of sex, age or quality of the study score was found.
Image:
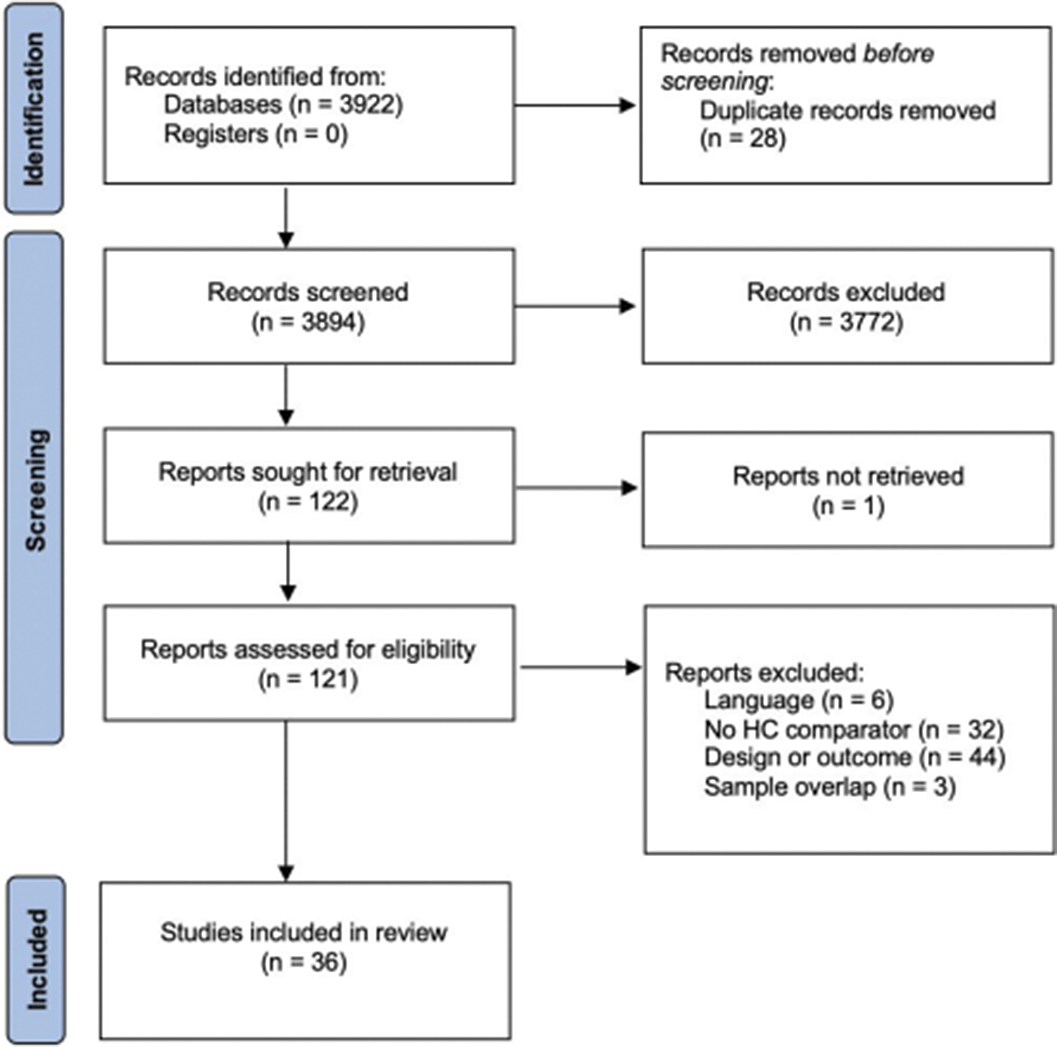
Image 2:
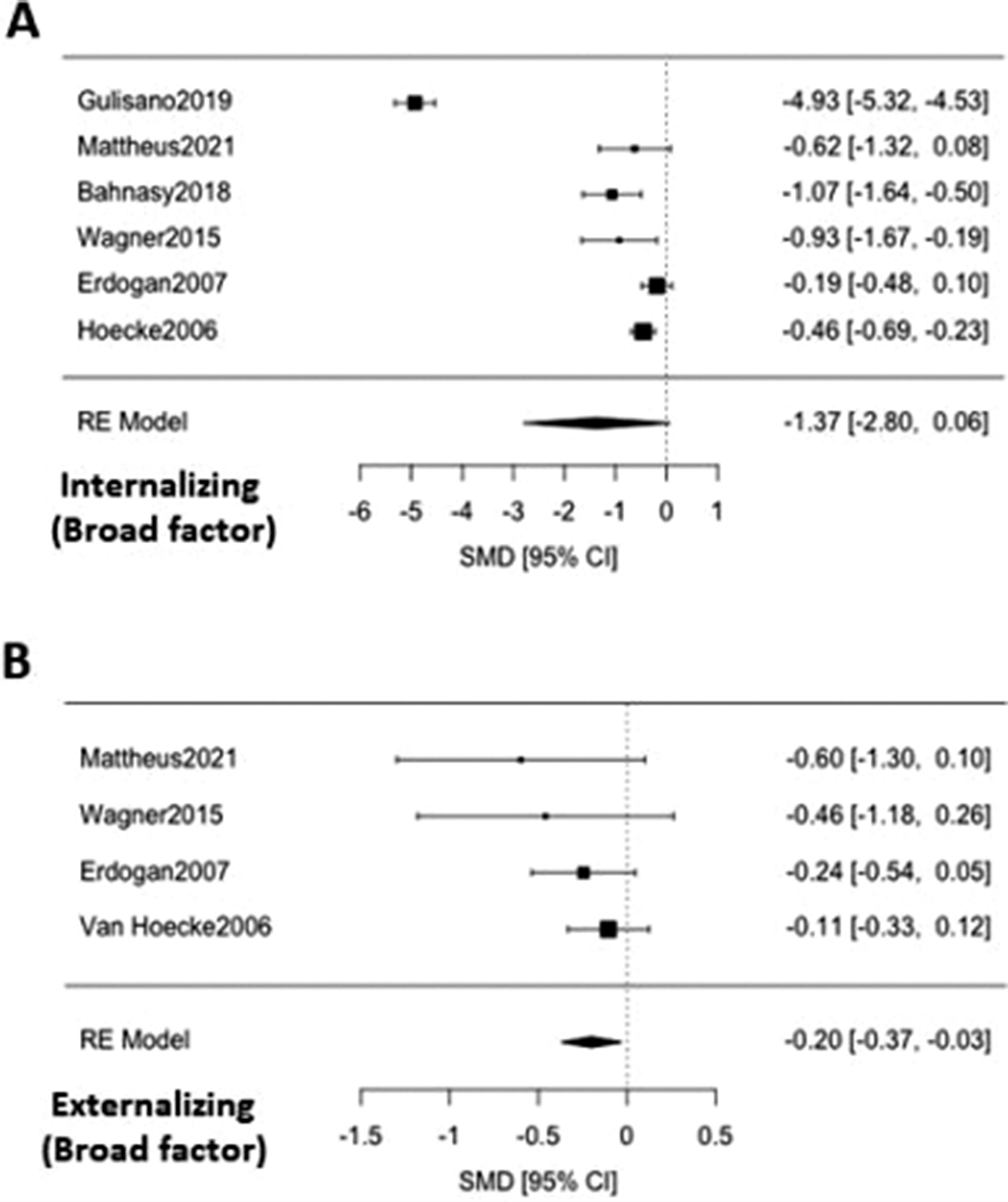
Image 3:
Children with an elimination disorder may have significant internalizing and externalizing problems, as well as impaired self-concept. It is recommendable to screen for them in children with ED and provide interventions as appropriate.
None Declared

