The First Large Absorption Survey in H i (FLASH) is a large-area radio survey for neutral hydrogen in and around galaxies in the intermediate redshift range  $0.4\lt z\lt1.0$, using the 21-cm H i absorption line as a probe of cold neutral gas. The survey uses the ASKAP radio telescope and will cover 24,000 deg
$0.4\lt z\lt1.0$, using the 21-cm H i absorption line as a probe of cold neutral gas. The survey uses the ASKAP radio telescope and will cover 24,000 deg $^2$ of sky over the next five years. FLASH breaks new ground in two ways – it is the first large H i absorption survey to be carried out without any optical preselection of targets, and we use an automated Bayesian line-finding tool to search through large datasets and assign a statistical significance to potential line detections. Two Pilot Surveys, covering around 3000 deg
$^2$ of sky over the next five years. FLASH breaks new ground in two ways – it is the first large H i absorption survey to be carried out without any optical preselection of targets, and we use an automated Bayesian line-finding tool to search through large datasets and assign a statistical significance to potential line detections. Two Pilot Surveys, covering around 3000 deg $^2$ of sky, were carried out in 2019-22 to test and verify the strategy for the full FLASH survey. The processed data products from these Pilot Surveys (spectral-line cubes, continuum images, and catalogues) are public and available online. In this paper, we describe the FLASH spectral-line and continuum data products and discuss the quality of the H i spectra and the completeness of our automated line search. Finally, we present a set of 30 new H i absorption lines that were robustly detected in the Pilot Surveys, almost doubling the number of known H i absorption systems at
$^2$ of sky, were carried out in 2019-22 to test and verify the strategy for the full FLASH survey. The processed data products from these Pilot Surveys (spectral-line cubes, continuum images, and catalogues) are public and available online. In this paper, we describe the FLASH spectral-line and continuum data products and discuss the quality of the H i spectra and the completeness of our automated line search. Finally, we present a set of 30 new H i absorption lines that were robustly detected in the Pilot Surveys, almost doubling the number of known H i absorption systems at  $0.4\lt z\lt1$. The detected lines span a wide range in H i optical depth, including three lines with a peak optical depth
$0.4\lt z\lt1$. The detected lines span a wide range in H i optical depth, including three lines with a peak optical depth  $\tau\gt1$, and appear to be a mixture of intervening and associated systems. Interestingly, around two-thirds of the lines found in this untargeted sample are detected against sources with a peaked-spectrum radio continuum, which are only a minor (5–20%) fraction of the overall radio-source population. The detection rate for H i absorption lines in the Pilot Surveys (0.3 to 0.5 lines per 40 deg
$\tau\gt1$, and appear to be a mixture of intervening and associated systems. Interestingly, around two-thirds of the lines found in this untargeted sample are detected against sources with a peaked-spectrum radio continuum, which are only a minor (5–20%) fraction of the overall radio-source population. The detection rate for H i absorption lines in the Pilot Surveys (0.3 to 0.5 lines per 40 deg $^2$ ASKAP field) is a factor of two below the expected value. One possible reason for this is the presence of a range of spectral-line artefacts in the Pilot Survey data that have now been mitigated and are not expected to recur in the full FLASH survey. A future paper in this series will discuss the host galaxies of the H i absorption systems identified here.
$^2$ ASKAP field) is a factor of two below the expected value. One possible reason for this is the presence of a range of spectral-line artefacts in the Pilot Survey data that have now been mitigated and are not expected to recur in the full FLASH survey. A future paper in this series will discuss the host galaxies of the H i absorption systems identified here.
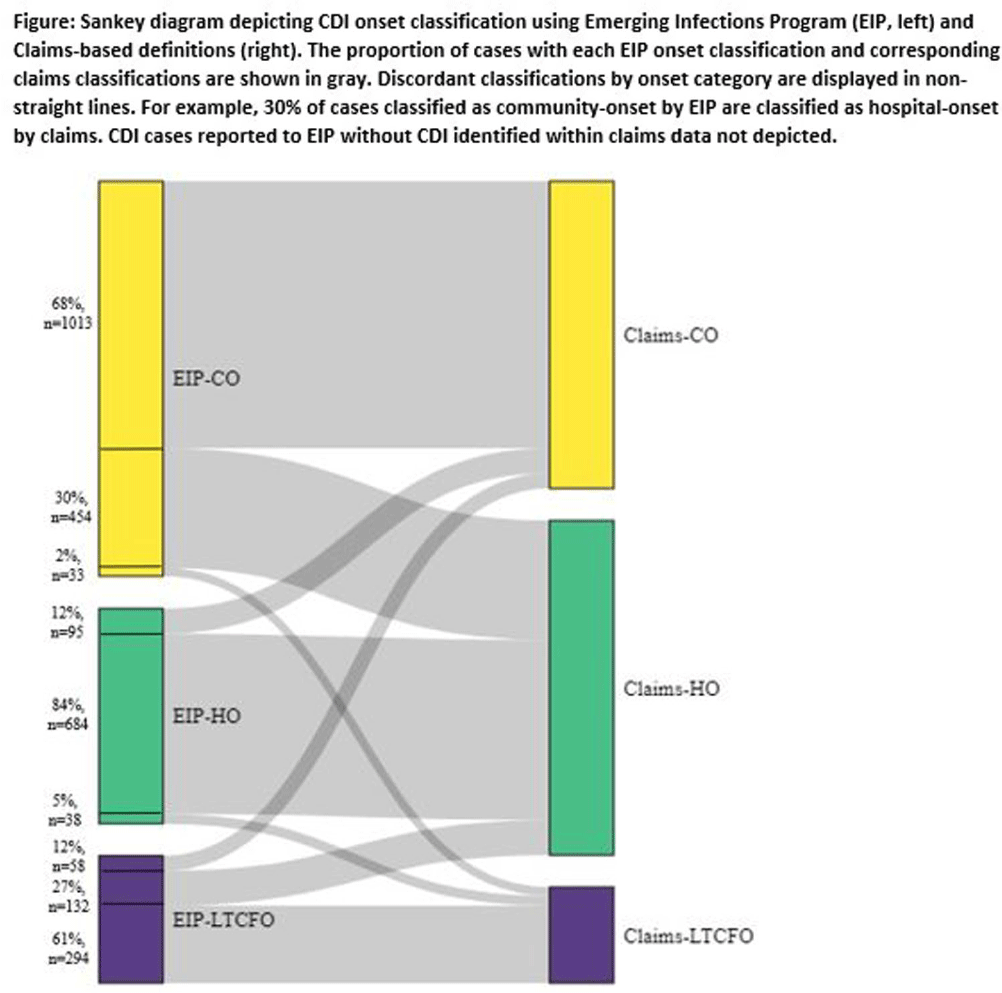
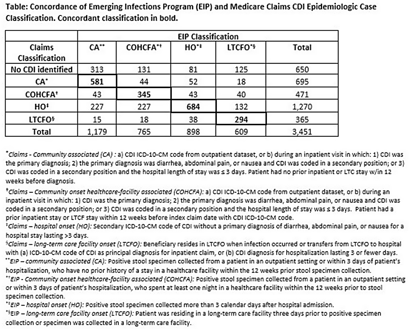
Background: Medicare claims are frequently used to study Clostridioides difficile infection (CDI) epidemiology. Categorizing CDI based on location of onset and potential exposure is critical in understanding transmission patterns and prevention strategies. While claims data are well-suited for identifying prior healthcare utilization exposures, they lack specimen collection and diagnosis dates to assign likely location of onset. Algorithms to classify CDI onset and healthcare association using claims data have been published, but the degree of misclassification is unknown. Methods: We linked patients with laboratory-confirmed CDI reported to four Emerging Infections Program (EIP) sites from 2016-2020 to Medicare beneficiaries using residence, birth date, sex, and hospitalization and/or healthcare exposure dates. Uniquely linked patients with fee-for-service Medicare A/B coverage and complete EIP case report forms were included. Patients with a claims CDI diagnosis code within ±28 days of a positive CDI test reported to EIP were categorized as hospital-onset (HO), long-term care facility onset (LTCFO), or community-onset (CO, either healthcare facility-associated [COHCFA] or community-associated [CA]) using a previously published algorithm based on claim type, ICD-10-CM code position, and duration of hospitalization (if applicable). EIP classifies CDI into these categories using positive specimen collection date and other information from chart review (e.g. admit/discharge dates). We assessed concordance of EIP and claims case classifications using Cohen’s kappa. Results: Of 10,002 eligible EIP-identified CDI cases, 7,064 were linked to a unique beneficiary; 3,451 met Medicare A/B fee-for-service coverage inclusion criteria. Of these, 650 (19%) did not have a claims diagnosis code ±28 days of the EIP specimen collection date (Table); 48% (313/650) of those without a claims diagnosis code were categorized by EIP as CA CDI. Among those with a CDI diagnosis code, concurrence of claims-based and EIP CDI classification was 68% (κ=0.56). Concurrence was highest for HO and lowest for COHCFA CDI. A substantial number of EIP-classified CO CDIs (30%, Figure) were misclassified as HO using the claims-based algorithm; half of these had a primary ICD-10 diagnosis code of sepsis (226/454; 50%). Conclusions: Evidence of CDI in claims data was found for 81% of EIP-reported CDI cases. Medicare classification algorithms concurred with the EIP classification in 68% of cases. Discordance was most common for community-onset CDI patients, many of whom were hospitalized with a primary diagnosis of sepsis. Misclassification of CO-CDI as HO may bias findings of claims-based CDI studies.