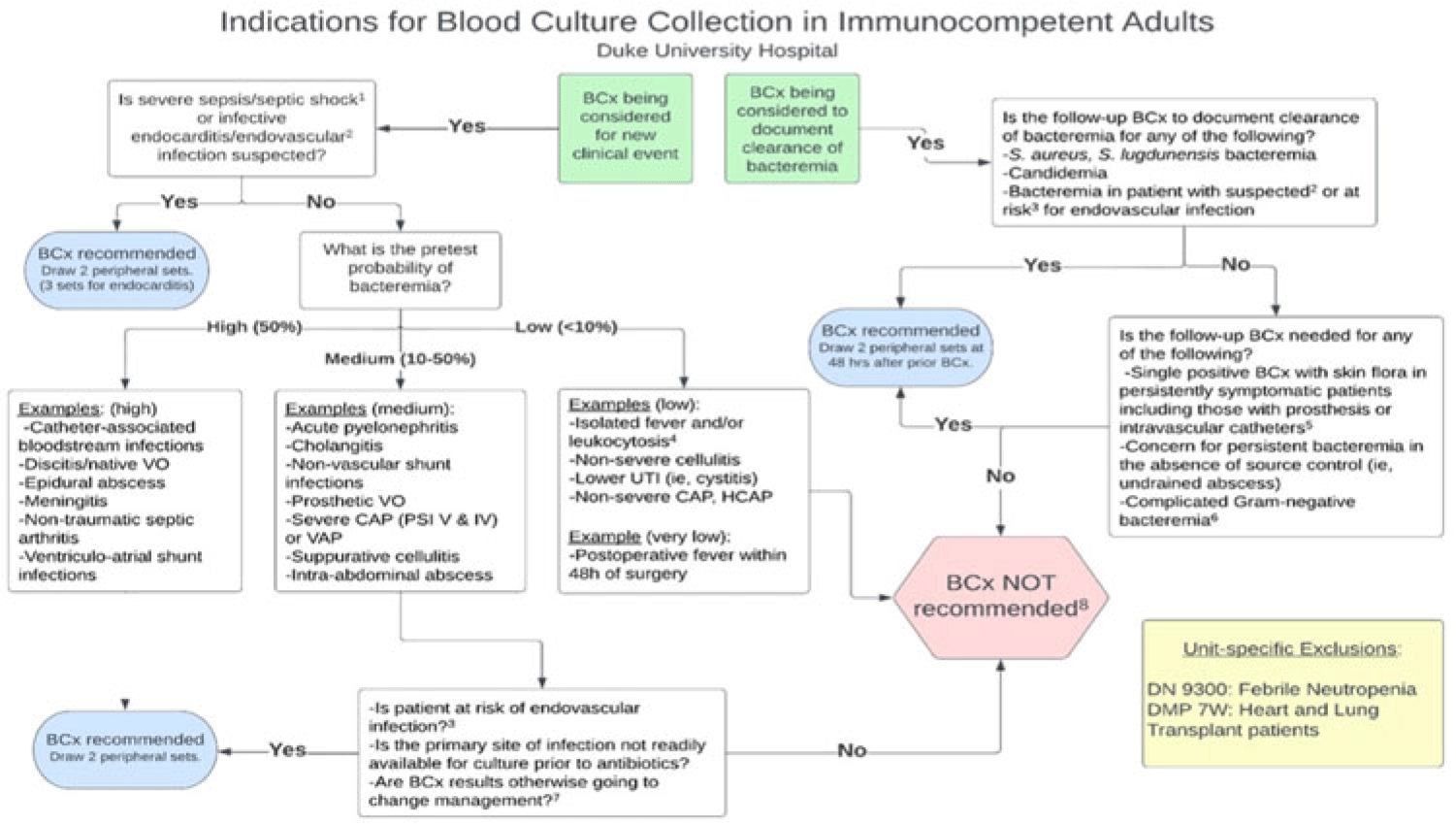
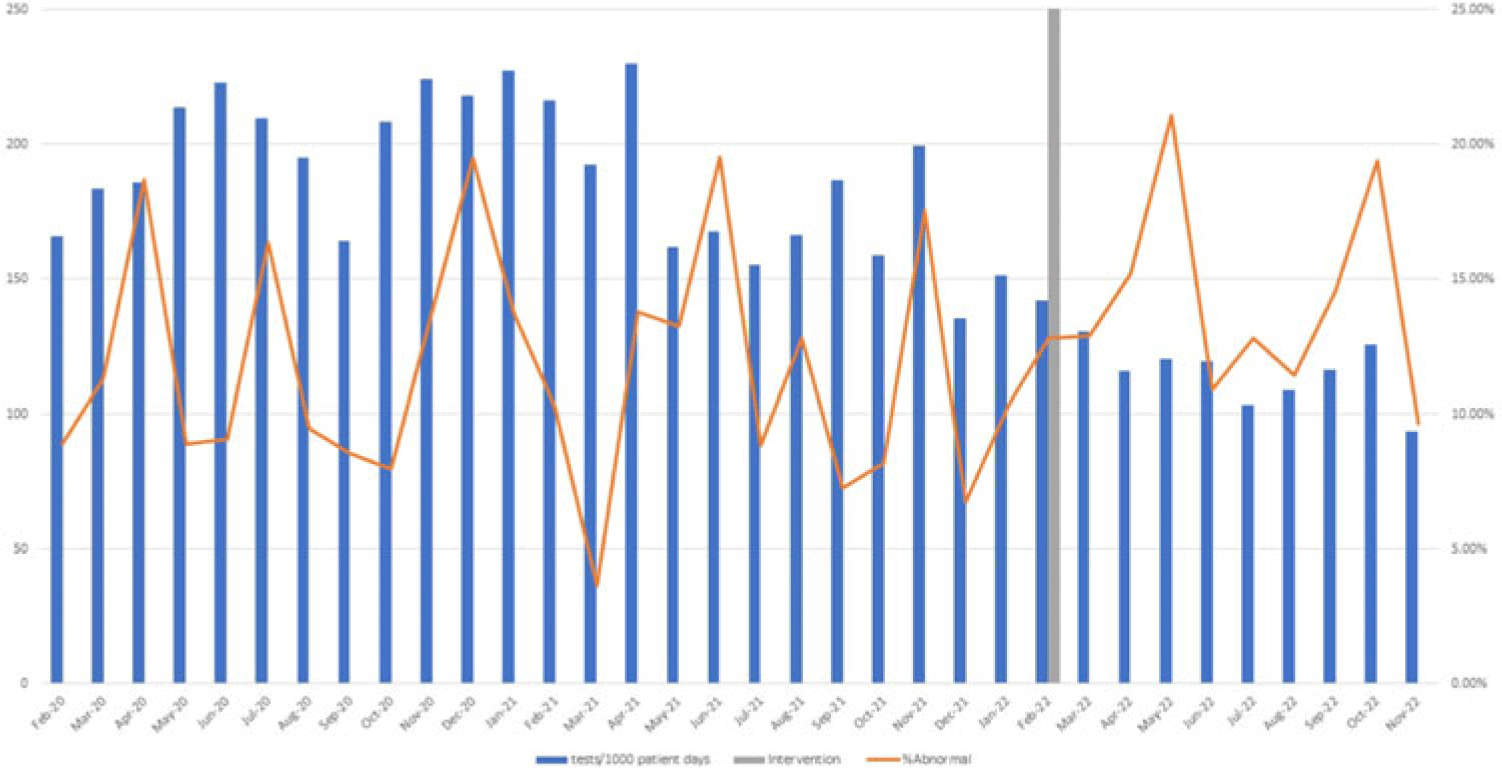
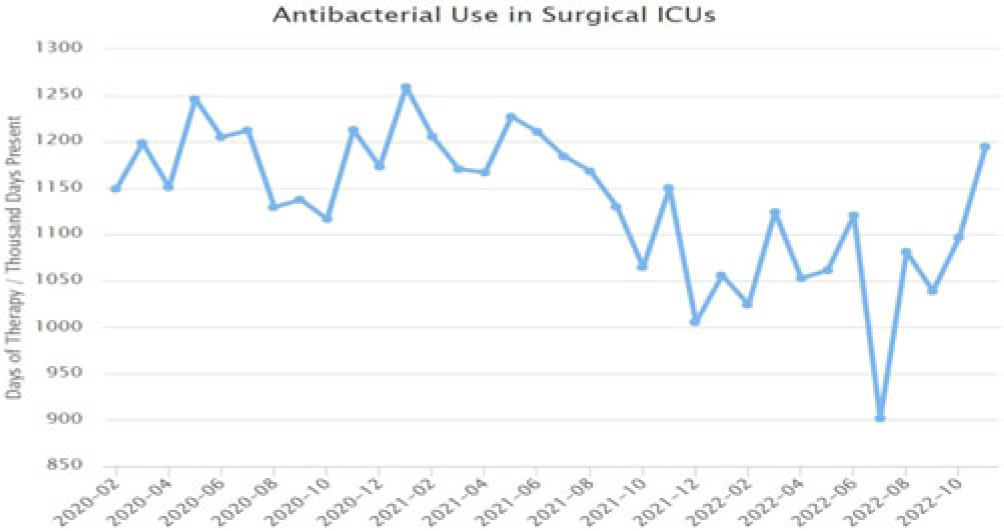
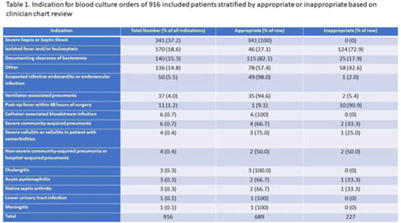
Background: Blood cultures are commonly ordered for patients with low risk of bacteremia. Liberal blood-culture ordering increases the risk of false-positive results, which can lead to increased length of stay, excess antibiotics, and unnecessary diagnostic procedures. We implemented a blood-culture indication algorithm with data feedback and assessed the impact on ordering volume and percent positivity. Methods: We performed a prospective cohort study from February 2022 to November 2022 using historical controls from February 2020 to January 2022. We introduced the blood-culture algorithm (Fig. 1) in 2 adult surgical intensive care units (ICUs). Clinicians reviewed charts of eligible patients with blood cultures weekly to determine whether the blood-culture algorithm was followed. They provided feedback to the unit medical directors weekly. We defined a blood-culture event as ≥1 blood culture within 24 hours. We excluded patients aged <18 years, absolute neutrophil count <500, and heart and lung transplant recipients at the time of blood-culture review. Results: In total, 7,315 blood-culture events in the preintervention group and 2,506 blood-culture events in the postintervention group met eligibility criteria. The average monthly blood-culture rate decreased from 190 blood cultures per 1,000 patient days to 142 blood cultures per 1,000 patient days (P < .01) after the algorithm was implemented. (Fig. 2) The average monthly blood-culture positivity increased from 11.7% to 14.2% (P = .13). Average monthly days of antibiotic therapy (DOT) was lower in the postintervention period than in the preintervention period (2,200 vs 1,940; P < .01). (Fig. 3) The ICU length of stay did not change before the intervention compared to after the intervention: 10 days (IQR, 5–18) versus 10 days (IQR, 5–17; P = .63). The in-hospital mortality rate was lower during the postintervention period, but the difference was not statistically significant: 9.24% versus 8.34% (P = .17). The all-cause 30-day mortality was significantly lower during the intervention period: 11.9% versus 9.7% (P < .01). The unplanned 30-day readmission percentage was significantly lower during the intervention period (10.6% vs 7.6%; P < .01). Over the 9-month intervention, we reviewed 916 blood-culture events in 452 unique patients. Overall, 74.6% of blood cultures followed the algorithm. The most common reasons overall for ordering blood cultures were severe sepsis or septic shock (37%), isolated fever and/or leukocytosis (19%), and documenting clearance of bacteremia (15%) (Table 1). The most common indications for inappropriate blood cultures were isolated fever and/or leukocytosis (53%). Conclusions: We introduced a blood-culture algorithm with data feedback in 2 surgical ICUs and observed decreases in blood-culture volume without a negative impact on ICU LOS or mortality rate.
Disclosure: None
We present WALLABY pilot data release 1, the first public release of H i pilot survey data from the Wide-field ASKAP L-band Legacy All-sky Blind Survey (WALLABY) on the Australian Square Kilometre Array Pathfinder. Phase 1 of the WALLABY pilot survey targeted three
 $60\,\mathrm{deg}^{2}$
regions on the sky in the direction of the Hydra and Norma galaxy clusters and the NGC 4636 galaxy group, covering the redshift range of
$60\,\mathrm{deg}^{2}$
regions on the sky in the direction of the Hydra and Norma galaxy clusters and the NGC 4636 galaxy group, covering the redshift range of
 $z \lesssim 0.08$
. The source catalogue, images and spectra of nearly 600 extragalactic H i detections and kinematic models for 109 spatially resolved galaxies are available. As the pilot survey targeted regions containing nearby group and cluster environments, the median redshift of the sample of
$z \lesssim 0.08$
. The source catalogue, images and spectra of nearly 600 extragalactic H i detections and kinematic models for 109 spatially resolved galaxies are available. As the pilot survey targeted regions containing nearby group and cluster environments, the median redshift of the sample of
 $z \approx 0.014$
is relatively low compared to the full WALLABY survey. The median galaxy H i mass is
$z \approx 0.014$
is relatively low compared to the full WALLABY survey. The median galaxy H i mass is
 $2.3 \times 10^{9}\,{\rm M}_{{\odot}}$
. The target noise level of
$2.3 \times 10^{9}\,{\rm M}_{{\odot}}$
. The target noise level of
 $1.6\,\mathrm{mJy}$
per 30′′ beam and
$1.6\,\mathrm{mJy}$
per 30′′ beam and
 $18.5\,\mathrm{kHz}$
channel translates into a
$18.5\,\mathrm{kHz}$
channel translates into a
 $5 \sigma$
H i mass sensitivity for point sources of about
$5 \sigma$
H i mass sensitivity for point sources of about
 $5.2 \times 10^{8} \, (D_{\rm L} / \mathrm{100\,Mpc})^{2} \, {\rm M}_{{\odot}}$
across 50 spectral channels (
$5.2 \times 10^{8} \, (D_{\rm L} / \mathrm{100\,Mpc})^{2} \, {\rm M}_{{\odot}}$
across 50 spectral channels (
 ${\approx} 200\,\mathrm{km \, s}^{-1}$
) and a
${\approx} 200\,\mathrm{km \, s}^{-1}$
) and a
 $5 \sigma$
H i column density sensitivity of about
$5 \sigma$
H i column density sensitivity of about
 $8.6 \times 10^{19} \, (1 + z)^{4}\,\mathrm{cm}^{-2}$
across 5 channels (
$8.6 \times 10^{19} \, (1 + z)^{4}\,\mathrm{cm}^{-2}$
across 5 channels (
 ${\approx} 20\,\mathrm{km \, s}^{-1}$
) for emission filling the 30′′ beam. As expected for a pilot survey, several technical issues and artefacts are still affecting the data quality. Most notably, there are systematic flux errors of up to several 10% caused by uncertainties about the exact size and shape of each of the primary beams as well as the presence of sidelobes due to the finite deconvolution threshold. In addition, artefacts such as residual continuum emission and bandpass ripples have affected some of the data. The pilot survey has been highly successful in uncovering such technical problems, most of which are expected to be addressed and rectified before the start of the full WALLABY survey.
${\approx} 20\,\mathrm{km \, s}^{-1}$
) for emission filling the 30′′ beam. As expected for a pilot survey, several technical issues and artefacts are still affecting the data quality. Most notably, there are systematic flux errors of up to several 10% caused by uncertainties about the exact size and shape of each of the primary beams as well as the presence of sidelobes due to the finite deconvolution threshold. In addition, artefacts such as residual continuum emission and bandpass ripples have affected some of the data. The pilot survey has been highly successful in uncovering such technical problems, most of which are expected to be addressed and rectified before the start of the full WALLABY survey.
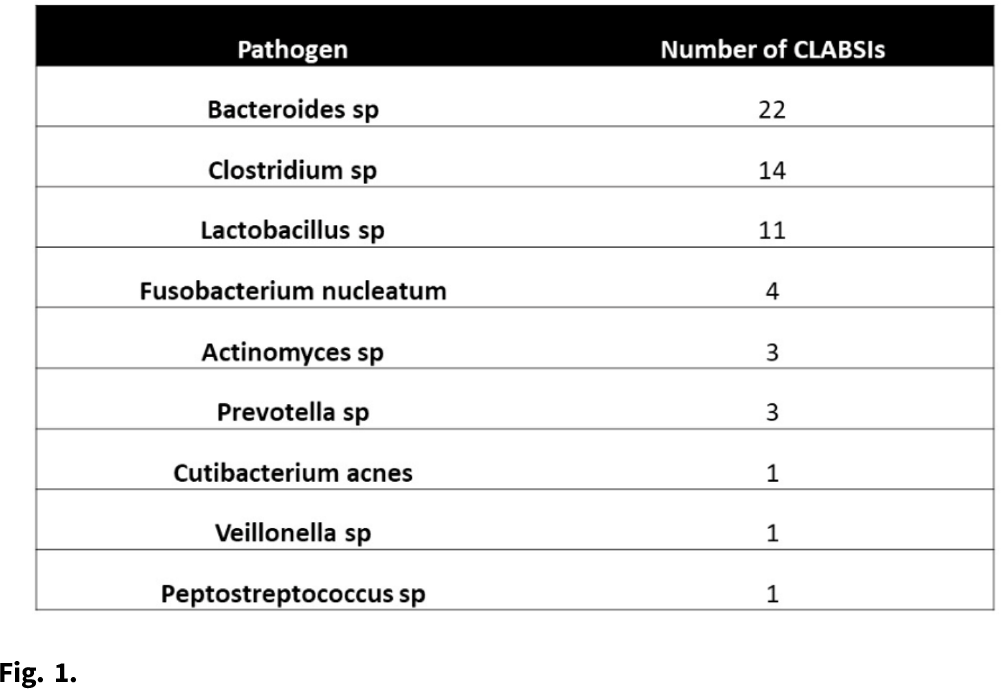
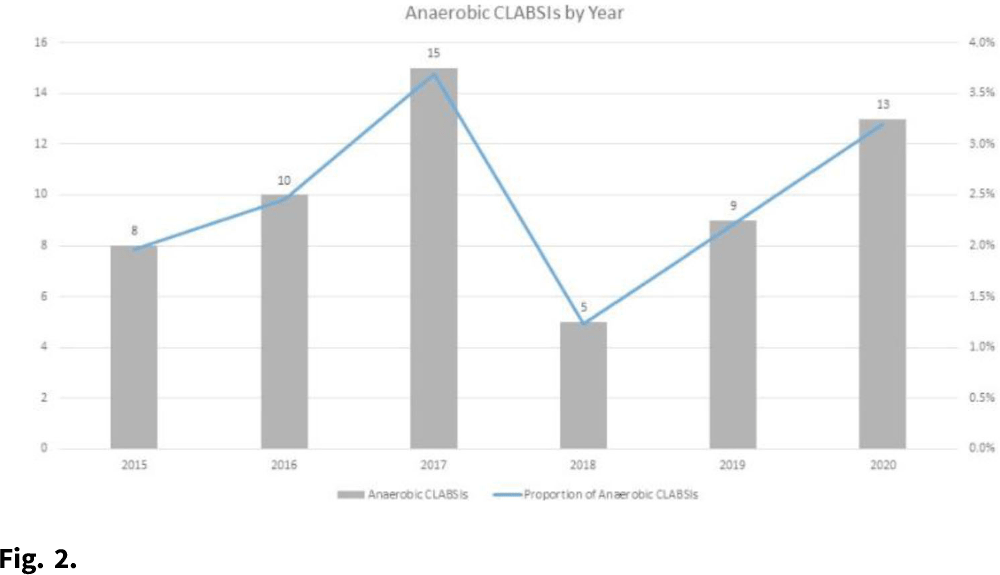
Background: Central-line–associated bloodstream infections (CLABSIs) arise from bacteria migrating from the skin along the catheter, by direct inoculation, or from pathogens that form biofilms on the interior surface of the catheter. However, given the oxygen-poor environments that obligate anaerobes require, these organisms are unlikely to survive long enough on the skin or on the catheter after direct inoculation to be the true cause of a CLABSI. Although some anaerobic CLABSIs may meet the definition for a mucosal-barrier-injury, laboratory-confirmed, bloodstream infection (MBI-LCBI), some may be not. We sought to determine the proportion of CLABSIs attributed to obligate anaerobic bacteria, and we sought to determine the pathophysiologic source of these infections. Methods: We performed a retrospective analysis of prospectively collected CLABSI data at 54 hospitals (academic and community) in the southeastern United States from January 2015 to December 2020. We performed chart reviews on a convenient sample for which medical records were available. We calculated the proportion of CLABSIs due to obligate anaerobes, and we have described a subset of anaerobic CLABSI cases. Results: We identified 60 anaerobic CLABSIs of 2,430 CLABSIs (2.5%). Of the 60 anaerobic CLABSIs, 7 were polymicrobial with nonanaerobic bacteria. The most common species we identified were Bacteroides, Clostridium, and Lactobacillus (Table 1). The proportion of anaerobic CLABSIs per year varied from 1.2% to 3.7% (Fig. 1). Of 60 anaerobic CLABSIs, 29 (48%) occurred in the only quaternary-care academic medical center in the database. In contrast, an average of 0.6 (SD, 0.6) anaerobic CLABSIs occurred in the 53 community hospitals over the 6-year study period. Of these 29 anaerobic CLABSIs, 23 (79%) were clinically consistent with secondary bloodstream infections (BSIs) due to gastrointestinal or genitourinary source, but they lacked appropriate documentation to meet NHSN criteria for secondary BSI or MBI-LCBI based on case reviews by infection prevention physicians. The other 6 anaerobic CLABSIs did not have a clear clinical etiology and did not meet MBI-LCBI criteria. In addition, 27 (93%) of 29 anaerobic CLABSIs occurred in patients who were either solid-organ transplant recipients, were stem-cell transplant recipients, or were receiving chemotherapy. Lastly, 27 (93%) of 29 anaerobic CLABSIs were treated with antibiotics. Conclusions: Anaerobic CLABSIs are uncommon events, but CLABSI may disproportionately affect large, academic hospitals caring for a high proportion of medically complex patients. Additional criteria could be added to the MBI-LCBI to better classify anaerobic BSI.
Funding: None
Disclosures: None
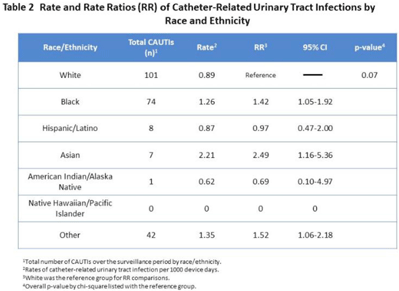
Background: Racial and ethnic disparities in healthcare access, medical treatment, and outcomes have been extensively reported. However, the impact of racial and ethnic differences in patient safety, including healthcare-associated infections, has not been well described. Methods: We performed a retrospective review analyzing prospectively collected data on central-line–associated bloodstream infection (CLABSI) and catheter-associated urinary tract infection (CAUTI) rates per 1,000 device days. Data for adult patients admitted to an academic medical center between 2018 and 2021 were stratified by 7 racial and ethnic groups: non-Hispanic White, non-Hispanic Black, Hispanic/Latino, Asian, American Indian/Alaska Native, Native Hawaiian/Pacific Islander, and othe. The “other” group was composed of bi- or multiracial patients, or those for whom no data were reported. We compared the CLABSI and CAUTI rates between the different racial and ethnic groups using Poisson regression. Results: Compared to non-Hispanic White patients, the rate of CLABSI was significantly higher in non-Hispanic Black patients (1.27; 95% CI, 1.02–1.58; P < .03) and those in the “other” race category (1.79; 95% CI, 1.39–2.30; P < .001, respectively), and these trends increased in Hispanic/Latino patients (Table 1). Similarly, Black patients had higher rates of CAUTI (1.42; 95% CI, 1.05–1.92; P < .02), as did Asian patients (2.49; 95% CI, 1.16–5.36; P < .02), and patients in the “other” category (1.52; 95% CI, 1.06–2.18; P < .02) (Table 2). Conclusions: Racial and ethnic minorities may be vulnerable to a higher rate of patient safety events, including CLABSIs and CAUTIs. Additional analyses controlling for potential confounding factors are needed to better understand the relationship between race or ethnicity, clinical management, and healthcare-associated infections. This evaluation is essential to inform mitigation strategies and to provide optimum, equitable care for all.
Funding: None
Disclosures: None