With wide-field phased array feed technology, the Australian Square Kilometre Array Pathfinder (ASKAP) is ideally suited to search for seemingly rare radio transient sources that are difficult to discover previous-generation narrow-field telescopes. The Commensal Real-time ASKAP Fast Transient (CRAFT) Survey Science Project has developed instrumentation to continuously search for fast radio transients (duration  $\lesssim$ 1 s) with ASKAP, with a particular focus on finding and localising fast radio bursts (FRBs). Since 2018, the CRAFT survey has been searching for FRBs and other fast transients by incoherently adding the intensities received by individual ASKAP antennas, and then correcting for the impact of frequency dispersion on these short-duration signals in the resultant incoherent sum (ICS) in real time. This low-latency detection enables the triggering of voltage buffers, which facilitates the localisation of the transient source and the study of spectro-polarimetric properties at high time resolution. Here we report the sample of 43 FRBs discovered in this CRAFT/ICS survey to date. This includes 22 FRBs that had not previously been reported: 16 FRBs localised by ASKAP to
$\lesssim$ 1 s) with ASKAP, with a particular focus on finding and localising fast radio bursts (FRBs). Since 2018, the CRAFT survey has been searching for FRBs and other fast transients by incoherently adding the intensities received by individual ASKAP antennas, and then correcting for the impact of frequency dispersion on these short-duration signals in the resultant incoherent sum (ICS) in real time. This low-latency detection enables the triggering of voltage buffers, which facilitates the localisation of the transient source and the study of spectro-polarimetric properties at high time resolution. Here we report the sample of 43 FRBs discovered in this CRAFT/ICS survey to date. This includes 22 FRBs that had not previously been reported: 16 FRBs localised by ASKAP to  $\lesssim 1$ arcsec and 6 FRBs localised to
$\lesssim 1$ arcsec and 6 FRBs localised to  $\sim 10$ arcmin. Of the new arcsecond-localised FRBs, we have identified and characterised host galaxies (and measured redshifts) for 11. The median of all 30 measured host redshifts from the survey to date is
$\sim 10$ arcmin. Of the new arcsecond-localised FRBs, we have identified and characterised host galaxies (and measured redshifts) for 11. The median of all 30 measured host redshifts from the survey to date is  $z=0.23$. We summarise results from the searches, in particular those contributing to our understanding of the burst progenitors and emission mechanisms, and on the use of bursts as probes of intervening media. We conclude by foreshadowing future FRB surveys with ASKAP using a coherent detection system that is currently being commissioned. This will increase the burst detection rate by a factor of approximately ten and also the distance to which ASKAP can localise FRBs.
$z=0.23$. We summarise results from the searches, in particular those contributing to our understanding of the burst progenitors and emission mechanisms, and on the use of bursts as probes of intervening media. We conclude by foreshadowing future FRB surveys with ASKAP using a coherent detection system that is currently being commissioned. This will increase the burst detection rate by a factor of approximately ten and also the distance to which ASKAP can localise FRBs.
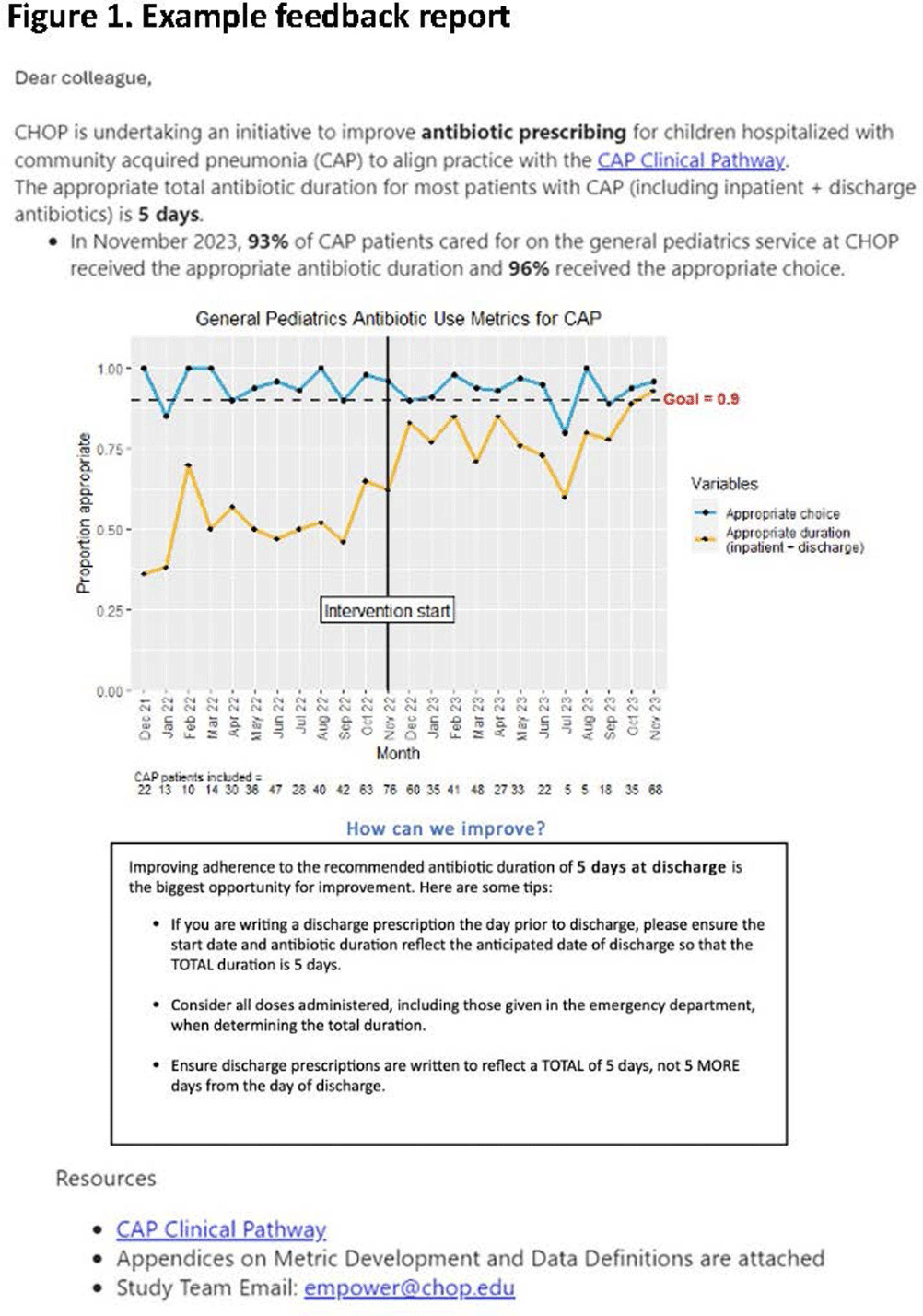
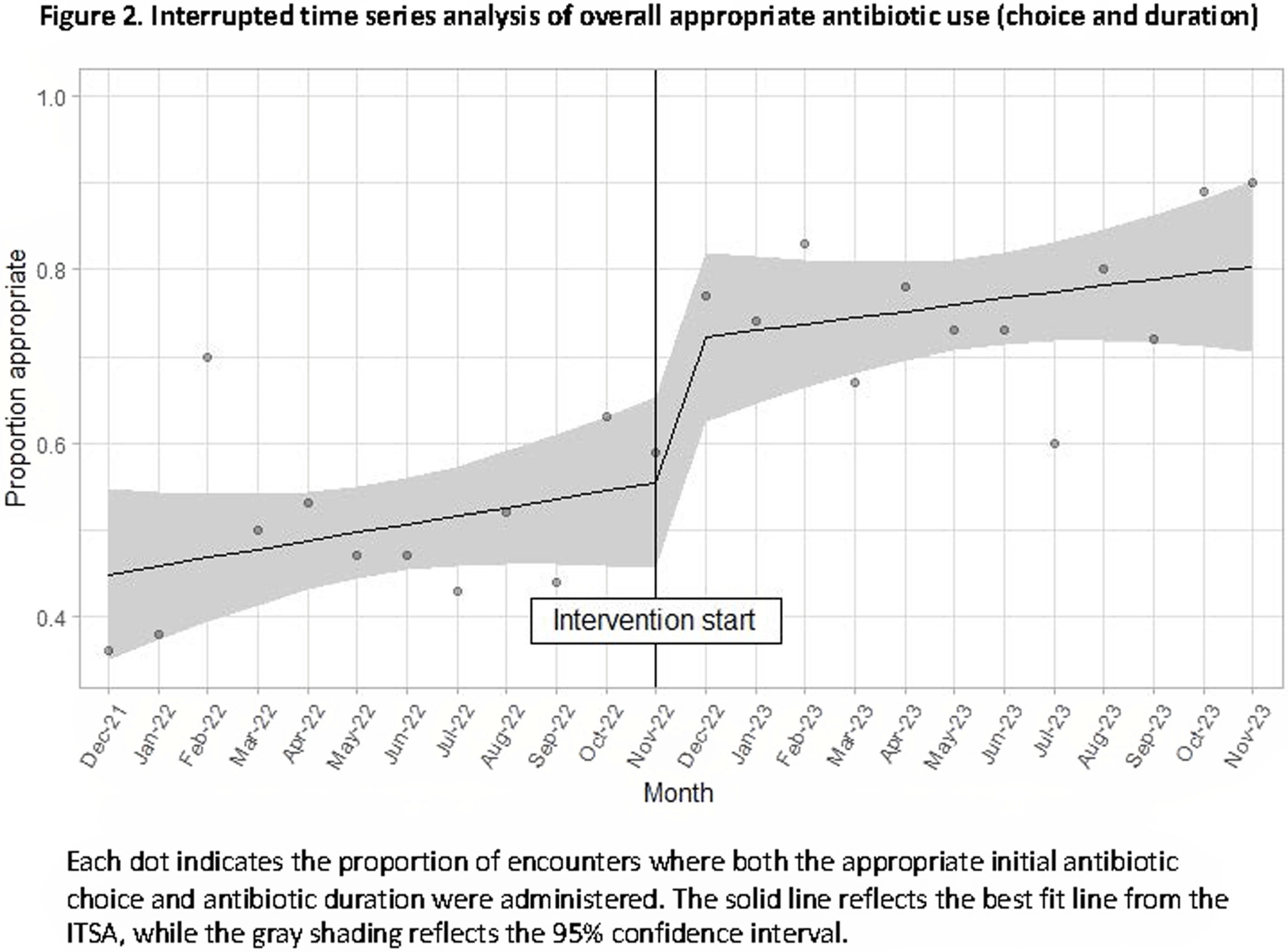
Background: Feedback reports summarizing clinician performance are effective tools to improve antibiotic stewardship in the ambulatory setting, but few studies have evaluated their effectiveness for pediatric inpatients. We developed and implemented feedback reports reflecting electronically-derived measures of appropriate antibiotic choice and duration for community acquired pneumonia (CAP) and measured their impact on appropriate antibiotic use in children hospitalized for CAP. Methods: We performed a single center quasi-experimental study including children 6 months to 17 years hospitalized for CAP between 12/1/2021-11/30/2023. Children with chronic medical conditions, ICU stays >48 hours, and outside transfers were excluded. The intervention occurred in 11/2022 and included clinician education, a monthly group-level feedback report disseminated by email (Figure 1), and a monthly review of clinician performance during a virtual quality improvement meeting. Patient characteristics were compared using chi-square or Wilcoxon rank sum tests. Interrupted time series analysis (ITSA) was used to measure the immediate change in the proportion of CAP encounters receiving both the appropriate antibiotic choice and duration, as well as the change in slope from the preintervention to the postintervention periods. Choice and duration were analyzed separately using ITSA as a secondary analysis. Results: There were 817 CAP encounters, including 420 preintervention and 397 postintervention. Patients admitted in the postintervention period were older (median age 2 years vs 3 years, P=0.03), but otherwise there were no differences in race, ethnicity, sex, ICU admission, or complicated pneumonia. Preintervention, 52% of encounters received both the appropriate antibiotic choice and duration; 96% of encounters received the appropriate antibiotic choice and 54% received the appropriate duration. The ITSA demonstrated an immediate 16% increase in the proportion of patients receiving both appropriate antibiotic choice and duration (95% confidence interval, 1-31%; P = 0.047) and no significant further increase over time following the intervention (P = 0.84) (Figure 2). When antibiotic choice was analyzed separately by ITSA, there was no immediate change or change over time in the proportion of patients receiving the appropriate antibiotic choice. In the ITSA of duration alone, there was an immediate 17% increase in the proportion receiving the appropriate duration (95% confidence interval, 2-33%; P = 0.03) and no change over time. Conclusion: Feedback reports generated from electronically-derived metrics of antibiotic choice and duration, combined with ongoing clinician education, increased the proportion of children with CAP treated with the appropriate antibiotic duration. Electronic feedback reports are a scalable and impactful intervention to improve antibiotic use in children hospitalized with CAP.