We partner with a secure submission system to handle manuscript submissions.
Please note:
You will need an account for the submission system, which is separate to your Cambridge Core account. For login and submission support, please visit the
submission and support pages.
Please review this journal's author instructions, particularly the
preparing your materials
page, before submitting your manuscript.
Click Proceed to submission system to continue to our partner's website.
To save this undefined to your undefined account, please select one or more formats and confirm that you agree to abide by our usage policies. If this is the first time you used this feature, you will be asked to authorise Cambridge Core to connect with your undefined account.
Find out more about saving content to .
To send this article to your Kindle, first ensure no-reply@cambridge.org is added to your Approved Personal Document E-mail List under your Personal Document Settings on the Manage Your Content and Devices page of your Amazon account. Then enter the ‘name’ part of your Kindle email address below. Find out more about sending to your Kindle.
Find out more about saving to your Kindle.
Note you can select to save to either the @free.kindle.com or @kindle.com variations. ‘@free.kindle.com’ emails are free but can only be saved to your device when it is connected to wi-fi. ‘@kindle.com’ emails can be delivered even when you are not connected to wi-fi, but note that service fees apply.
To assess child vitamin A supplementation (VAS) coverage in 2019 and 2020 and explore key factors, including COVID-19 concerns, that influenced VAS status in four sub-Saharan African countries.
Design:
Data from eight representative household surveys were used to assess VAS coverage. Multivariable logistic regression models examined the effect of rural/urban residence, child sex and age, caregiver education, COVID-19 concern and household wealth on VAS status.
Setting:
Nine (2019) and 12 (2020) districts in Burkina Faso, Côte d’Ivoire, Guinea and Mali.
Participants:
28 283 caregivers of children aged 6–59 months.
Results:
Between 2019 and 2020, VAS coverage increased in Burkina Faso (82·2–93·1 %), Côte d’Ivoire (90·3–93·3 %) and Mali (76·1–79·3 %) and decreased in Guinea (86·0 % to 81·7 %). Rural children had a higher likelihood of VAS uptake compared with urban children in Burkina Faso (adjusted OR (aOR) = 4·22; 95 % CI: 3·11, 5·72), Côte d’Ivoire (aOR = 5·19; 95 % CI: 3·10, 8·70) and Mali (aOR = 1·41; 95 % CI: 1·15, 1·74). Children aged 12–59 months had a higher likelihood of VAS uptake compared with children aged 6–11 months in Côte d’Ivoire (aOR = 1·67; 95 % CI: 1·12, 2·48) and Mali (aOR = 1·74; 95 % CI: 1·34, 2·26). Moderate-to-high COVID-19 concern was associated with a lower likelihood of VAS uptake in Côte d’Ivoire (aOR = 0·55; 95 % CI: 0·37, 0·80).
Conclusion:
The increase in VAS coverage from 2019 to 2020 suggests that COVID-19 concerns may not have limited VAS uptake in some African countries, though geographic inequities should be considered.
The COVID-19 pandemic increased food insufficiency: a severe form of food insecurity. Drawing on an ecological framework, we aimed to understand factors that contributed to changes in food insufficiency from April to December 2020, in a large urban population hard hit by the pandemic.
Design:
We conducted internet surveys every 2 weeks in April–December 2020, including a subset of items from the Food Insecurity Experience Scale. Longitudinal analysis identified predictors of food insufficiency, using fixed effects models.
Setting:
Los Angeles County, which has a diverse population of 10 million residents.
Participants:
A representative sample of 1535 adults in Los Angeles County who are participants in the Understanding Coronavirus in America tracking survey.
Results:
Rates of food insufficiency spiked in the first year of the pandemic, especially among participants living in poverty, in middle adulthood and with larger households. Government food assistance from the Supplemental Nutrition Assistance Program was significantly associated with reduced food insufficiency over time, while other forms of assistance such as help from family and friends or stimulus funds were not.
Conclusions:
The findings highlight that during a crisis, there is value in rapidly monitoring food insufficiency and investing in government food benefits.
To assess the association between child ultra-processed food (UPF) consumption and home-school learning environment characteristics during school closures due to the COVID-19 pandemic in schoolchildren with low- and middle income in Chile.
Design:
Cross-sectional. UPF consumption was collected using the Nova screener. We apply the structured days hypothesis (SDH) to assess home-school learning environment characteristics with three constructs that summarised school preparedness for online teaching and learning, school closure difficulties for caregivers and child routine. We explored associations between child UPF consumption and home-school environment characteristics using multivariate linear regression analyses after controlling for child demographic and school characteristics.
Setting:
Low- and middle-income neighbourhoods in southeastern Santiago, Chile.
Participants:
Children from the Food Environment Chilean Cohort (n 428, 8–10 years old).
Results:
Based on the Nova score, child mean consumption of UPF was 4·3 (sd 1·9) groups. We found a statistically significant negative association between child routine for eating, play and study and child UPF consumption when we adjusted for child sociodemographic (model 1: β = –0·19, (95 % CI –0·40, 0·02)) and school characteristics (model 2: β = –0·20, (95 % CI –0·41, 0·00)). Associations between school preparedness for online teaching or school closure difficulties and UPF were not statistically significant.
Conclusions:
Variations in child routines during the COVID-19 pandemic were negatively associated with UPF intake in schoolchildren with low- and middle income. Our findings are consistent with the SDH, suggesting the school environment helps regulate eating behaviours. Future research should evaluate what happens when children return to in-person classes at school.
The present study examined military families’ use of food distribution resources and military (e.g. rank) and non-military (e.g. race/ethnicity) characteristics associated with using food distribution resources.
Design:
Secondary data analyses from a cross-sectional survey in the first 6 months of 2021.
Setting:
A national sample of eligible families completed an online survey.
Participants:
8326 enlisted military families with an active duty service member in the United States Army or Air Force who applied for supplemental childcare funding distributed by National Military Family Association.
Results:
13·2 % of the families reported utilising a food distribution resource in the past 12 months. Those with lower financial well-being were more likely to utilise such resources. Older (OR = 1·04, 95 % CI = 1·02, 1·05, P < 0·001), single-earner (OR = 0·73, 95 % CI = 0·61, 0·89, P = 0·001) families with a lower rank (OR = 0·69, 95 % CI = 0·64, 0·75, P < 0·001) and Army affiliation (compared with Air Force) (OR = 2·31, 95 % CI = 2·01, 2·67, P < 0·001) were more likely to utilise food distribution resources. Members of certain racial/ethnic minority groups were more likely to utilise food distribution resources than White respondents (OR from 1·47 for multi-racial to 1·69 for Asians), as were families with more dependent children (OR = 1·35, 95 % CI = 1·25, 1·47, P < 0·001).
Conclusions:
These results identify the extent of food distribution resource utilisation in military families with young children approximately 1 year into the COVID-19 pandemic. The results also identify characteristics associated with their use of food distribution resources. Findings are discussed with an emphasis on prevention and intervention implications for military families.
To examine diet quality and diet-related factors among male adults of reproductive age with and without disabilities.
Design:
Cross-sectional data from the National Health and Nutrition Examination Surveys, 2013–2018.
Setting:
Disability was reported as serious difficulty hearing, seeing, concentrating, walking, dressing and/or running errands due to physical, mental or emotional conditions. Diet quality was assessed by the Healthy Eating Index (HEI)-2015 and diet-related factors included self-rated diet healthfulness, food security and food assistance programmes. Multivariable linear regression estimated differences in HEI-2015 scores. Multivariable Poisson regression estimated adjusted prevalence ratios (aPR) and 95 % CI for diet-related factors.
Participants:
In total, 3249 males, 18–44 years; of whom, 441 (13·4 %) reported having disabilities.
Results:
Compared with males without disabilities, those with disabilities had a 2·69-point (95 % CI: –4·18, –1·20) lower mean total HEI-2015 score and approximately one-third to half of a point lower HEI-2015 component scores for greens and beans, total protein foods, seafood and plant proteins, fatty acids and added sugars. Males with any disabilities were more likely to have low food security (aPR = 1·57; 95 % CI: 1·28, 2·92); household participation in food assistance programmes (aPR = 1·61; 95 % CI: 1·34, 1·93) and consume fast food meals during the previous week (1–3 meals: aPR = 1·11; 95 % CI: 1·01–1·21 and 4 or more meals: aPR = 1·18; 95 % CI: 1·01–1·38) compared with males with no disabilities.
Conclusions:
Factors affecting diet and other modifiable health behaviours among male adults of reproductive age with disabilities require further investigation. Health promotion strategies that are adaptive to diverse populations within the disability community are needed.
To establish an international consensus on the definition of food security, measures and advocacy priorities in high-income countries.
Design:
A two-round online Delphi survey with closing in March 2020 and December 2021. Consensus was set a priori at 75 %. Qualitative data were synthesised and priorities were ranked.
Setting:
High-income countries.
Participants:
Household food security experts in academia, government and non-government organisations who had published in the last 5 years.
Results:
Up to thirty-two participants from fourteen high-income countries responded to the Delphi with a 25 % response rate in Round 1 and a 38 % response rate in Round 2. Consensus was reached on the technical food security definition and its dimensions. Consensus was not reached on a definition suitable for the general public. All participants agreed that food security monitoring systems provide valuable data for in-country decision-making. Favoured interventions were those that focused on upstream social policy influencing income. Respondents agreed that both national and local community level strategies were required to ameliorate food insecurity, reinforcing the complexity of the problem.
Conclusions:
This study furthers the conceptual understanding of the commonly used definition of food security and its constituent dimensions. Strong advocacy is needed to ensure food security monitoring, policy and mitigation strategies are implemented. The consensus on the importance of prioritising actions that address the underlying determinants of household food security by experts in the field from across wealthy nations provides evidence to focus advocacy efforts and generate public debate.
This paper describes the first web-based self-completed 24-h recall designed to categorise food intake according to Nova groups – Nova24h – and its agreement with a reference tool in estimating the dietary relative contribution of the four Nova food groups (% of total energy intake).
Design:
Comparisons of estimates of dietary relative contributions of Nova groups obtained by Nova24h and one standard interviewer-led 24-h recall.
Setting:
Nationwide adult cohort study in Brazil.
Participants:
The subjects were 186 participants of the NutriNet Brasil Cohort Study (n 186).
Results:
No statistically significant differences were observed between the Nova24h and the reference tool mean contributions of unprocessed or minimally processed foods (52·3 % v. 52·6 %), processed culinary ingredients (11·6 % v. 11·9 %), processed foods (17·1 % v. 14·7 %) and ultra-processed foods (19·0 % v. 20·9 %). Intraclass correlation coefficients between individual estimates obtained for each Nova group showed moderate to good agreement (0·54–0·78). Substantial or almost perfect agreement between the tools was seen regarding the ability to rank participants according to quintiles of contribution of each Nova group (PABAK 0·69–0·81).
Conclusions:
Nova24h is a suitable tool for estimating the dietary relative energy contribution of Nova food groups in the NutriNet Brasil cohort. New studies are necessary to verify its adequacy in other populations.
To identify the optimal weight gain at the end of the second trimester.
Design:
This was a population-based cohort study from the antenatal care system in Tianjin, China. We calculated gestational weight gain (GWG) based on the weight measured in the first trimester and the end of the second trimester. Restricted cubic spline analysis was performed to model the possible non-linear relationships between GWG and adverse outcomes. The optimal GWG was defined as the value of the lowest risk. Non-inferiority margins and the shape of the spline curves identified the recommended ranges in Chinese-specific BMI categories.
Setting:
Tianjin Maternal and Child Health Cohort.
Participants:
Singleton pregnant women aged 18–45 years.
Results:
In total, 69 859 pregnant women were included. Adverse outcome (including stillbirth, preterm birth, hypertensive disorders of pregnancy, gestational diabetes mellitus, small and large for gestational age) was significantly associated with GWG at the end of the second trimester. The risk score was non-linearly correlated with GWG in the underweight, normal weight and overweight groups. GWG at the end of the second trimester should not be < 7 kg in underweight group. For most normal-weight women, a GWG of about 8 kg is optimal. Pregnant women who are overweight should not have a GWG of more than 9 kg. We advised women with overweight and obesity to keep positive growth of GWG (> 0 kg) in the first and second trimesters.
Conclusions:
According to the comprehensive adverse maternal and infant outcomes, we recommend the optimal GWG at the end of the second trimester. This study may provide a considerable reference for weight management.
To assess the alignment of YouTube® videos providing dietary recommendations for gout with evidence-based guidelines targeted at the United Kingdom (UK) population and to establish their quality.
Design:
A content analysis of YouTube® videos providing dietary recommendations for gout was undertaken. Videos were categorised by video source. Each video’s dietary recommendations for gout were compared with three evidence-based guidelines for gout, producing a compliance score. Presence of non-guideline advice was assessed. Understandability and actionability were evaluated using the Patient Education Material Assessment Tool for Audio-Visual Materials. Reliability was assessed using an adapted-DISCERN tool and educational quality using the Global Quality Score Five-Point Scale. Differences between video source and continuous variables were assessed using one-way Kruskal–Wallis H tests. For categorical variables, associations were investigated using Fisher–Freeman–Halton tests.
Setting:
Online, May–June 2020.
Participants:
One-hundred thirty-one videos.
Results:
Alignment of videos with evidence-based guidelines was poor (median compliance score 27 % (interquartile range 17–37 %)). Additionally, 57 % of videos contained non-guideline advice. The health professional source group had the fewest videos containing non-guideline advice, but this was only significantly lower than the naturopath group (31 % v. 81 %, P = 0·009). Almost 70 % of videos were considered poorly actionable and 50 % poorly understandable. Most videos were rated poor for reliability (79 %) and poor to generally poor for educational quality (49 %).
Conclusions:
YouTube® videos providing dietary recommendations for gout frequently fail to conform to evidence-based guidelines, and their educational quality, reliability, understandability and actionability are often poor. More high-quality, comprehensive, evidence-based YouTube® videos are required for UK gout patients.
To examine associations between work and commute hours with food consumption and test whether neighbourhood type (20-minute neighbourhood (20MN)/non-20MN) moderate associations.
Design:
Cross-sectional analysis of the Places and Locations for Activity and Nutrition study (ProjectPLAN). Exposures were work hours (not working (0 h), working up to full-time (1–38 h/week), working overtime (> 38 h/week)), and among those employed, combined weekly work and commute hours (continuous). Outcomes were usual consumption of fruit, vegetables, takeaway food, snacks and soft drinks, and number of discretionary food types (takeaway, snacks and soft drinks) consumed weekly. Generalised linear models were fitted to examine associations between each exposure and outcome. The moderating role of neighbourhood type was examined through interaction terms between each exposure and neighbourhood type (20MN/non-20MN).
Setting:
Melbourne and Adelaide, Australia, 2018–2019.
Participants:
Adults ≥ 18 years old (n 769).
Results:
Although all confidence intervals contained the null, overall, patterns suggested non-workers and overtime workers have less healthy food behaviours than up-to-full-time workers. Among those employed, analysis of continuous work and commute hours data suggested longer work and commute hours were positively associated with takeaway consumption (OR = 1·014, 95 % CI 0·999, 1·030, P-value = 0·066). Patterns of better behaviours were observed across most outcomes for those in 20MN than non-20MN. However, differences in associations between work and commute hours with food consumption across neighbourhood type were negligible.
Conclusions:
Longer work and commute hours may induce poorer food behaviours. There was weak evidence to suggest 20MN moderate associations between work and commute hours with food consumption, although behaviours appeared healthier for those in 20MN.
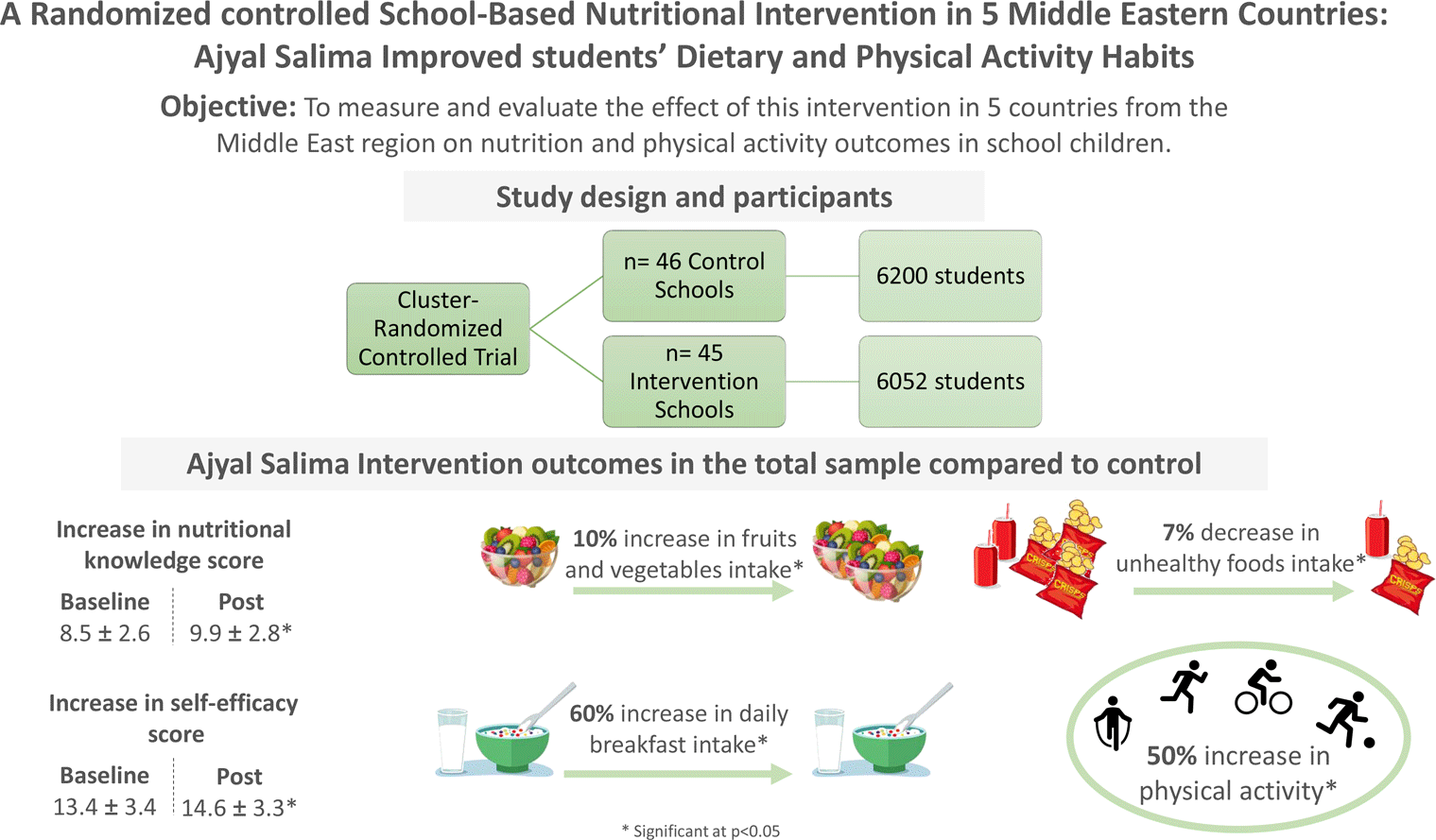
The purpose of this study was to measure the impact of the Ajyal Salima school intervention on nutrition and physical activity outcomes in children aged 9–11 years.
Design:
The study was a 1-year cluster-randomised controlled trial. Ajyal Salima used a multi-component approach including classroom activities, family programme and food service adaptation. Outcomes included daily intake of breakfast, frequency of healthy and unhealthy food consumption, frequency of physical activity, knowledge score and self-efficacy score. Intervention and control groups were compared for all main outcomes and a post-intervention qualitative evaluation assessed strengths and limitations of the intervention components.
Setting:
Schools in five countries – Lebanon, Jordan, Palestine, Saudi Arabia and Bahrain.
Participants:
Schools were selected by Ministries of Health and Education within their jurisdictions. Forty-five intervention schools (6052 students) and forty-six control schools (6200 students) were included in the analysis.
Results:
The intervention group had a significantly higher odds of consuming breakfast daily (OR 95 % CI = 1·60, 1·35, 1·90), consuming healthy foods (OR 95 % CI = 1·60, 1·39, 1·84) and a decreased odds of consuming unhealthy foods and sweetened beverages (OR, 95 % CI = 0·70, 0·60, 0·81). Additionally, school children in the intervention group, as compared with the control group, were 47 % more likely to exercise outside school hours (OR 95 % CI = 1·47, 1·23, 1·76). Lastly, children in the intervention group had a significantly improved nutritional knowledge score and improved self-efficacy by 1·3 score unit and 1·1 score unit, respectively.
Conclusions:
The Ajyal Salima intervention led to significant improvements in dietary and physical activity habits among school children and increased nutritional knowledge scores.
To assess the nutritional status and depression of the elderly forcibly displaced Myanmar nationals (FDMN) in Bangladesh and determine the associated factors of geriatric depression (GD).
Design:
This was a community-based, cross-sectional study among elderly FDMN. The Mini Nutritional Assessment Short-Form (MNA@-SF) and Geriatric Depression Scale Short-Form (GDS-15 SF) were used to determine malnutrition and GD, respectively.
Setting:
The study was conducted between November 2021 and March 2022 in Kutupalong Refugee Camp, Cox’s Bazar, Bangladesh.
Participants:
The study participants were elderly FDMN aged ≥ 60 years (n 430).
Results:
The mean age and BMI were 71·7(±7·8) years and 21·94(±2·6) kg/m2, respectively. There was a high prevalence of self-reported diabetes mellitus (32·1 %), hypertension (26·7 %), hypotension (20 %), skin diseases (28·4 %) and chronic obstructive pulmonary disease (16·5 %). The prevalence of malnutrition was 25·3 %, and another 29·1 % were at risk. The prevalence of GD was 57·9 %, and co-occurrences of GD and malnutrition were seen in 17·5 % of participants. GD was significantly higher among elderly people with malnutrition (adjusted OR, AOR = 1·71, 95 % CI: 1·01, 2·89). FDMN aged ≥ 80 years were at higher risk of GD (AOR = 1·84, 95 % CI: 1·01, 3·37), and having fewer than five members in the household was an independent predictor of GD. Diabetes mellitus (AOR = 1·95, 95 % CI: 1·24, 3·08) and hypotension (AOR = 2·17, 95 % CI: 1·25, 2·78) were also significantly associated with an increased risk of GD.
Conclusion:
A high prevalence of GD and malnutrition was observed among elderly FDMN in Bangladesh. The agencies working in Cox’s Bazar should focus on geriatric malnutrition and GD for the improvement of the health situation of FDMN in Bangladesh.
To map the scientific research on food environments in Brazil, based on the following questions: How many studies have addressed food environments?; What study designs and methodological approaches were applied?; What is the geographic scope of the studies?; What scenarios and dimensions of food environments were studied?; Which population groups were studied?; How were food environments conceptualised?; What are the main limitations of the studies?
Design:
Scoping review conducted in four databases, from January 2005 to December 2022, using different food environment-related terms to cover the main types and dimensions proposed in the literature. The studies were independently selected by two authors. A narrative synthesis was used to summarise the findings.
Setting:
Brazil.
Participants:
130 articles.
Results:
Scientific research on Brazilian food environments has been increasing. The analytical quantitative approach and the cross-sectional design were the most frequently used. Most articles were published in English. The majority of studies evaluated the community food environment, addressed aspects of the physical dimension, sampled the adult population, had food consumption as an outcome, used primary data, and were carried out in capital cities in the Southeast region. Furthermore, in most articles, no conceptual model was explicitly adopted.
Conclusions:
Gaps in literature are related to the need for conducting studies in the Brazilian countryside, the support for the formulation of research questions based on conceptual models, the use of valid and reliable instruments to collect primary data, in addition to the need for a greater number of longitudinal, intervention and qualitative studies.
We investigated the association between dietary oxidative balance score (DOBS) and mortality and whether this association can be modified by sleep duration.
Design:
We calculated DOBS to estimate the overall oxidative effects of the diet, with higher DOBS reflecting more antioxidant intake and less pro-oxidant intake. Cox proportional hazards models were employed to examine the associations between DOBS and all-cause, CVD and cancer mortality in the general population and people with different sleep durations.
Setting:
Prospective analysis was conducted using data from the US National Health and Nutrition Examination Survey (NHANES, 2005–2015).
Participants:
A total of 15 991 US adults with complete information on dietary intake, sleep duration and mortality were included.
Results:
During a median follow-up of 7·4 years, 1675 deaths were observed. Participants in the highest quartile of DOBS were significantly associated with the lower risk of all-cause mortality (hazard ratio (HR) = 0·75; 95 % CI 0·61, 0·93) compared with those in the lowest. Furthermore, we found statistically significant interactions between DOBS and sleep duration on all-cause mortality (P interaction = 0·021). The inverse association between DOBS and all-cause mortality was significant in short sleepers (HR = 0·66, 95 % CI 0·48, 0·92), but not in normal and long sleepers.
Conclusions:
Our study observed that higher DOBS was associated with lower all-cause mortality, and this association appeared to be stronger among short sleepers. This study provides nutritional guidelines for improving health outcomes in adults, especially for short sleepers.
Dietary patterns express the combination and variety of foods in the diet. The partial least squares method allows extracting dietary patterns related to a specific health outcome. Few studies have evaluated obesity-related dietary patterns associated with telomeres length. This study aims to identify dietary patterns explaining obesity markers and to assess their association with leukocyte telomere length (LTL), a biological marker of the ageing process.
Design:
Cross-sectional study.
Setting:
University campuses in the state of Rio de Janeiro, Brazil
Participants:
478 participants of a civil servants’ cohort study with data on food consumption, obesity measurements (total body fat, visceral fat, BMI, leptin and adiponectin) and blood samples.
Results:
Three dietary patterns were extracted: (1) fast food and meat; (2) healthy and (3) traditional pattern, which included rice and beans, the staple foods most consumed in Brazil. All three dietary patterns explained 23·2 % of food consumption variation and 10·7 % of the obesity-related variables. The fast food and meat pattern were the first factor extracted, explaining 11–13 % variation of the obesity-related response variables (BMI, total body fat and visceral fat), leptin and adiponectin showed the lowest percentage (4·5–0·1 %). The healthy pattern mostly explained leptin and adiponectin variations (10·7 and 3·3 %, respectively). The traditional pattern was associated with LTL (β = 0·0117; 95 % CI 0·0001, 0·0233) after adjustment for the other patterns, age, sex, exercise practice, income and energy intake.
Conclusion:
Leukocyte telomere length was longer among participants eating a traditional dietary pattern that combines fruit, vegetables and beans.
Recent meta-analyses demonstrate that small-quantity lipid-based nutrient supplements (SQ-LNS) for young children significantly reduce child mortality, stunting, wasting, anaemia and adverse developmental outcomes. Cost considerations should inform policy decisions. We developed a modelling framework to estimate the cost and cost-effectiveness of SQ-LNS and applied the framework in the context of rural Uganda.
Design:
We adapted costs from a costing study of micronutrient powder (MNP) in Uganda, and based effectiveness estimates on recent meta-analyses and Uganda-specific estimates of baseline mortality and the prevalence of stunting, wasting, anaemia and developmental disability.
Setting:
Rural Uganda.
Participants:
Not applicable.
Results:
Providing SQ-LNS daily to all children in rural Uganda (> 1 million) for 12 months (from 6 to 18 months of age) via the existing Village Health Team system would cost ∼$52 per child (2020 US dollars) or ∼$58·7 million annually. SQ-LNS could avert an average of > 242 000 disability-adjusted life years (DALYs) annually as a result of preventing 3689 deaths, > 160 000 cases of moderate or severe anaemia and ∼6000 cases of developmental disability. The estimated cost per DALY averted is $242.
Conclusions:
In this context, SQ-LNS may be more cost-effective than other options such as MNP or the provision of complementary food, although the total cost for a programme including all age-eligible children would be high. Strategies to reduce costs, such as targeting to the most vulnerable populations and the elimination of taxes on SQ-LNS, may enhance financial feasibility.
To develop a healthy diet for Ethiopian women closely resembling their current diet and taking fasting periods into account while tracking the cost difference.
Design:
Linear goal programming models were built for three scenarios (non-fasting, continuous fasting and intermittent fasting). Each model minimised a function of deviations from nutrient reference values for eleven nutrients (protein, Ca, Fe, Zn, folate, and the vitamins A, B1, B2, B3, B6, and B12). The energy intake in optimised diets could only deviate 5 % from the current diet.
Settings:
Five regions are included in the urban and rural areas of Ethiopia.
Participants:
Two non-consecutive 24-h dietary recalls (24HDR) were collected from 494 Ethiopian women of reproductive age from November to December 2019.
Results:
Women’s mean energy intake was well above 2000 kcal across all socio-demographic subgroups. Compared to the current diet, the estimated intake of several food groups was considerably higher in the optimised modelled diets, that is, milk and dairy foods (396 v. 30 g/d), nuts and seeds (20 v. 1 g/d) and fruits (200 v. 7 g/d). Except for Ca and vitamin B12 intake in the continuous fasting diet, the proposed diets provide an adequate intake of the targeted micronutrients. The proposed diets had a maximum cost of 120 Ethiopian birrs ($3·5) per d, twice the current diet’s cost.
Conclusion:
The modelled diets may be feasible for women of reproductive age as they are close to their current diets and fulfil their energy and nutrient demands. However, the costs may be a barrier to implementation.
To evaluate nutrition literacy status and its association with adherence to the Mediterranean diet (MD), anthropometric parameters and lifestyle behaviours among early adolescents.
Design:
This is a cross-sectional study. Nutrition literacy was evaluated using the ‘Adolescent Nutrition Literacy Scale’. Dietary intake was assessed by 24-h food recall. The ‘Mediterranean Diet Quality Index’ was used to evaluate adolescents’ adherence to the MD. Physical activity was assessed using the International Physical Activity Questionnaire (IPAQ). Body weight, height, waist, hip and neck circumference were measured.
Setting:
Four secondary schools in İzmir, Türkiye
Participants:
The study included 1074 secondary school students.
Results:
Adolescents’ nutrition literacy was at a moderate level. Nutrition literacy scores were significantly lower in those who skip main meals. Adolescents with high nutrition literacy had higher intakes of fibre, protein, protein, Ca, K, Mg, P, vitamin C, folate and Fe intake than those with low and moderate nutrition literacy (P < 0·05). According to IPAQ, active adolescents had higher nutrition literacy scores than inactive adolescents. There was no significant difference in BMI and anthropometric measurements of the adolescents according to their nutrition literacy level. Linear regression analysis showed that each unit increase in nutrition literacy increased adherence to the MD by 0·286 points (β = 0·286) and decreased total screen time by 0·182 points (β = –0·182).
Conclusions:
These findings showed that nutrition literacy among early adolescents was not optimal, and a higher nutrition literacy score was significantly associated with higher MD adherence, and healthy eating habits and lifestyle behaviours.
To examine the feasibility and implementation of an optimal defaults intervention designed to align grocery purchases with a diet recommended for people with or at-risk for type 2 diabetes.
Design:
This was a 5-week pilot randomised trial with three groups: in-person grocery shopping, shopping online and shopping online with ‘default’ carts. Participants were asked to shop normally in Week One, according to group assignment in Weeks Two–Four (intervention period), and as preferred in Week Five. All groups received diabetes-friendly recipes via email each intervention week.
Setting:
Participants grocery shopped in person or online. Grocery receipt forms, enrolment information and exit surveys were collected remotely and used to assess feasibility and implementation.
Participants:
Sixty-five adults with or at-risk for type 2 diabetes.
Results:
Sixty-two participants completed the exit survey and fifty-five submitted receipts all 5 weeks. Forty utilised recipes, 95 % of whom indicated recipes were somewhat or very useful. Orange chicken, quesadillas and pork with potato and apples were the most liked recipes. Most Defaults group participants accepted at least some default cart items. Recipes with the highest default acceptance were whole grain pasta and chicken, quesadillas with black beans and chicken with olives. Participants’ primary concerns about the intervention were costs associated with online shopping, inability to select preferred foods and some recipes including ingredients household members would not eat.
Conclusions:
The study had high retention, data were successfully collected remotely and the intervention was acceptable to most participants. Tailoring recipes to household preferences may be beneficial in future studies.
To examine the effectiveness of a workplace sugar-sweetened beverage (SSB) sales ban on reducing SSB consumption in employees, including those with cardiometabolic disease risk factors.
Design:
A controlled trial of ethnically diverse, full-time employees who consumed SSB heavily (sales ban n 315; control n 342). Outcomes included standardised measures of change in SSB consumption in the workplace (primary) and at home between baseline and 6 months post-sales ban.
Setting:
Sutter Health, a large non-profit healthcare delivery system in Northern California.
Participants:
Full-time employees at Sutter Health screened for heavy SSB consumption.
Results:
Participants were 66·1 % non-White. On average, participants consumed 34·7 ounces (about 1 litre) of SSB per d, and the majority had an elevated baseline BMI (mean = 29·5). In adjusted regression analyses, those exposed to a workplace SSB sales ban for 6 months consumed 2·7 (95 % CI –4·9, –0·5) fewer ounces of SSB per d while at work, and 4·3 (95 % CI –8·4, –0·2) fewer total ounces per d, compared to controls. Sales ban participants with an elevated BMI or waist circumference had greater post-intervention reductions in workplace SSB consumption.
Conclusions:
Workplace sales bans can reduce SSB consumption in ethnically diverse employee populations, including those at higher risk for cardiometabolic disease.