Refine listing
Actions for selected content:
1418749 results in Open Access
1 Neurocognitive Correlates of Oculomotor Performance among U.S. Military Personnel with Mild Traumatic Brain Injury
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 666-667
-
- Article
-
- You have access
- Export citation
83 Association Between Tele-Neuropsychological Versus In-person Assessment in a Clinical Sample of Veterans with a History of Traumatic Brain Injury
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 486-487
-
- Article
-
- You have access
- Export citation
9 Serum Neurofilament is Associated with Diffusion Kurtosis Imaging in Chronic Mild-Moderate Traumatic Brain Injury
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, p. 121
-
- Article
-
- You have access
- Export citation
98 On Combining In-Person and Remote National Alzheimer’s Coordinating Center (NACC) Uniform Data Set (UDS) data
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 500-501
-
- Article
-
- You have access
- Export citation
6 Semantic and Phonemic Fluency in Alcohol Dependent Individuals
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 799-800
-
- Article
-
- You have access
- Export citation
29 Regulate to Remember: Cognitive Reappraisal Ability Impacts Prospective Memory Performance
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 818-819
-
- Article
-
- You have access
- Export citation
2 Neurocognition and Functional Status Among Ethnoculturally Diverse Older Adults: Support for the External Validity of the ADAS-Cog
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 86-87
-
- Article
-
- You have access
- Export citation
5 Cognitive Rehabilitation Using Teleneuropsychology. A Cohort Study in South America
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, p. 209
-
- Article
-
- You have access
- Export citation
51 Longitudinal Performance on the NIH Toolbox Cognition Module in a Cognitive Aging Sample
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 359-360
-
- Article
-
- You have access
- Export citation
91 Agent Orange Exposure and Mild Cognitive Impairment in U.S. Vietnam Era Veterans
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 392-393
-
- Article
-
- You have access
- Export citation
80 Ecological Momentary Assessment of the Fluctuations in Cognitive Performance and Contextual States of Community-Dwelling Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 483-484
-
- Article
-
- You have access
- Export citation
87 Examining the use of the Embedded Performance Validity Test in the Brief Visuospatial Memory Test-Revised Among Spanish-Speaking Patients
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 760-761
-
- Article
-
- You have access
- Export citation
20 The Influence of Brain Injury Severity, Anxiety, and Depression on Objective and Subjective Prospective Memory Problems
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 129-130
-
- Article
-
- You have access
- Export citation
92 Validation of Coin-in-Hand Procedure in a Veteran Population
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 764-765
-
- Article
-
- You have access
- Export citation
11 Contributions of Cardiovascular Burden, Peripheral Inflammation, and Brain Integrity on Digital Clock Drawing Performance in Non-Demented Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 325-326
-
- Article
-
- You have access
- Export citation
29 Vascular Burden Mediates the Relationship Between ADHD and Cognition in Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 637-638
-
- Article
-
- You have access
- Export citation
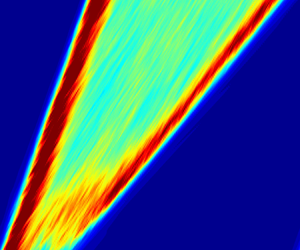
Scaling and mechanism of the propagation speed of the upstream turbulent front in pipe flow
-
- Journal:
- Journal of Fluid Mechanics / Volume 977 / 25 December 2023
- Published online by Cambridge University Press:
- 21 December 2023, R4
-
- Article
- Export citation
45 Gender Differences in Mathematics and its Cognitive and Non-Cognitive Predictors in Community College Students.
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 651-652
-
- Article
-
- You have access
- Export citation
58 Hippocampal Subregions Predict Executive Function Across the Adult Lifespan
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 466-467
-
- Article
-
- You have access
- Export citation
Invited Symposium 3: Pediatric Neuropsychology Medical Advances and Life Span Outcomes
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 665-666
-
- Article
-
- You have access
- Export citation
