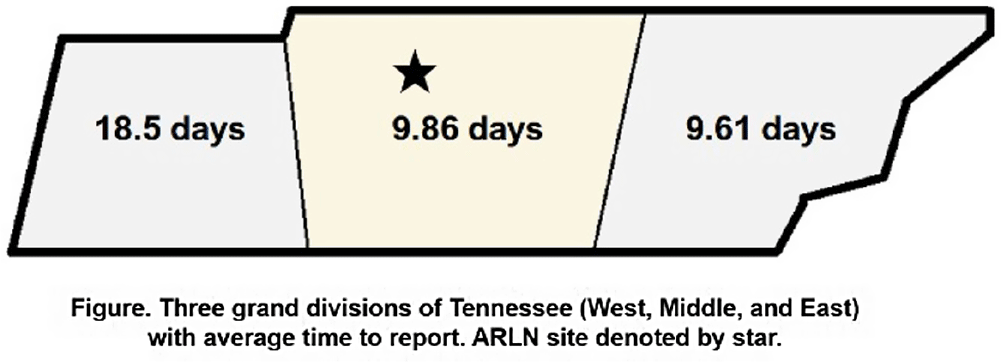
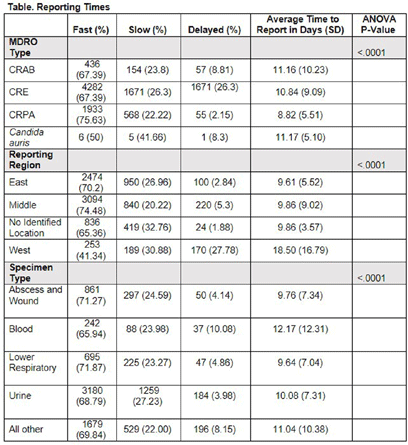
Background: Identification and timely reporting of multi-drug resistant organisms (MDROs) drives efficacy of infection prevention efforts. Data on MDRO reporting timeliness and inter-facility variability are limited. Facility-dependent variability in MDRO reporting across Tennessee was examined to identify opportunities for MDRO surveillance improvement. Methods: Data for reported Tennessee MDROs including carbapenem-resistant Enterobacterales (CRE), carbapenem-resistant Acinetobacter baumannii (CRAB), Carbapenem-resistant Pseudomonas aeruginosa (CRPA) and Candida auris, were obtained from the southeast regional Antibiotic Resistance Laboratory Network (ARLN) from 2018-2022, excluding screening and colonization specimens. Variance in days accrued from specimen collection to ARLN receipt was analyzed using one-way analysis of variance (ANOVA) with Tukey’s test (SAS 9.4). Facilities were categorized as fast (1-10 days), slow (11-20 days), or delayed (21-100 days) reporters. Results: There were 9,569 MDRO isolates reported. CRPA was reported faster than other MDROs (p < 0.001), while specimens from West Tennessee compared to other regions (p < 0.001) (Figure) and blood cultures compared to other specimens were reported more slowly (p < 0.001) (Table). There was no difference in reporting times for facilities using on-site microbiology laboratories versus reference laboratories (P = 0.062). Conclusion: MDRO reporting times varied across Tennessee by region, specimen, and organism. Future work to elucidate drivers of variability will consist of surveys and focused interviews with laboratory personnel to identify shared and unique barriers and opportunities for improvement.
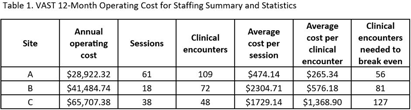
Background: In rural areas, antimicrobial stewardship programs often have limited access to infectious disease (ID) expertise. Videoconference Antimicrobial Stewardship Teams (VASTs) pair rural Veterans Affairs (VA) medical centers with an ID expert to discuss treatment of patients with concerns for infection. In a pilot study, VASTs were effective at improving antimicrobial use. Here, we evaluated 12-month operating costs for staffing for 3 VASTs. Methods: We used the following data to describe 12 months of clinical encounters for 3 VASTs operating from January 2022 – March 2023: the number of VAST sessions completed and clinical encounters; Current Procedural Terminology (CPT) codes associated with clinical encounters; session attendees (by role) and the time spent (percent effort) on VAST-related activities. The annual operating cost was based on the annual salaries and percent effort of VAST attendees. We used these characteristics combined with private-sector and Medicare reimbursements to evaluate the cost of implementation and number of clinical encounters needed to offset those costs (breakeven) for each site. Results: Three VASTs recorded 229 clinical encounters during 117 sessions (Table 1). Based on CPT codes, the approximate revenue per patient was $516.46. Site A, the only site to break even, had the most sessions and clinical encounters as well as the lowest operating costs. For Site B, a slight increase in the clinical encounters, which might be achieved by 3 additional VAST sessions, would help achieve breakeven. For Site C, increasing the number of clinical encounters to 3-4 per session would have helped their VAST break even without requiring a decrease in operating costs. Conclusions: The frequency of VAST sessions, volume of clinical encounters, and low operating costs all contributed the VAST at Site A achieving a financial break-even point within 12 months. Consideration of the potential number of clinical encounters and sessions will help other VASTs achieve financial sustainment, independent of cost-savings related to potential decreases in expenditures for antibiotics and antibiotic-related adverse events. These results also provide insight into possible adoption and diffusion of VAST-like programs in the Medicare hospital setting.