Fully relativistic particle-in-cell (PIC) simulations are crucial for advancing our knowledge of plasma physics. Modern supercomputers based on graphics processing units (GPUs) offer the potential to perform PIC simulations of unprecedented scale, but require robust and feature-rich codes that can fully leverage their computational resources. In this work, this demand is addressed by adding GPU acceleration to the PIC code Osiris. An overview of the algorithm, which features a CUDA extension to the underlying Fortran architecture, is given. Detailed performance benchmarks for thermal plasmas are presented, which demonstrate excellent weak scaling on NERSC's Perlmutter supercomputer and high levels of absolute performance. The robustness of the code to model a variety of physical systems is demonstrated via simulations of Weibel filamentation and laser-wakefield acceleration run with dynamic load balancing. Finally, measurements and analysis of energy consumption are provided that indicate that the GPU algorithm is up to ${\sim }$ 14 times faster and $\sim$
14 times faster and $\sim$ 7 times more energy efficient than the optimized CPU algorithm on a node-to-node basis. The described development addresses the PIC simulation community's computational demands both by contributing a robust and performant GPU-accelerated PIC code and by providing insight into efficient use of GPU hardware.
7 times more energy efficient than the optimized CPU algorithm on a node-to-node basis. The described development addresses the PIC simulation community's computational demands both by contributing a robust and performant GPU-accelerated PIC code and by providing insight into efficient use of GPU hardware.
Background: Healthcare accounts for 8.5% of total US greenhouse gas emissions (GHGE), with US healthcare the main contributor. Yet little effort has been made to measure healthcare related GHGE. Specifically, GHGE related to unnecessary antibiotic prescriptions is unclear, and to our knowledge, no one has used estimates of GHGE of unnecessary antibiotics as an antibiotic stewardship tool. We aimed to measure GHGE from solid waste associated with unnecessary antibiotic prescriptions for respiratory conditions. Methods: We calculated emissions for an outpatient prescription including the plastic bottle, paper leaflet, and paper bag (photos) based on the weight of each item multiplied by US Environmental Protection Agency (EPA) GHGE factors. Emission factors depend on waste type and treatment method which we assumed to be landfilled. To estimate unnecessary antibiotic prescriptions for respiratory infections, visits from nine University of Utah Health Urgent Care Centers from 2019-2022 were electronically identified and included if they had an ICD-10-CM code for a respiratory diagnosis where antibiotics are not indicated. Waste emissions of the paper and plastic in an individual prescription were then multiplied by the number of unnecessary respiratory antibiotic prescriptions for designated time periods to arrive at total landfilled waste emissions. We used similar methods applied to published 2014 data from CDC to estimate national waste emissions due to unnecessary antibiotic prescriptions for respiratory infections. Finally, we used the EPA’s GHG Equivalencies Calculator to convert emissions into tangible GHGE for providers and patients. Results: A prescription has 32g of paper and 15g of plastic waste. Among 124,461 urgent care visits (Table 1) in 2019-2022, 18,531 (14.9%) received an antibiotic. This equates to 593 kg of paper waste and 278 kg of plastic waste leading to a total landfilled waste emissions of 0.479 MT CO2e/ton. Using the EPA GHG Equivalencies Calculator, this equates to driving an average gasoline-powered car 1,228 miles. There were 14,482,976 unnecessary antibiotic prescriptions (Table 2) in the US for respiratory infections in 2014. Our estimates suggest these prescriptions led to 375.109 CO2e/ton of GHGE, the same as driving 961,610 miles by an average gasoline-powered vehicle. Conclusion: Unnecessary antibiotic prescriptions are associated with substantial GHGE. This estimate demands further evaluation across diagnoses and care delivery sites, and most importantly action. Additionally, the large GHG contribution of unnecessary antibiotics should be used as a stewardship tool to highlight low-value care that is likely contributing to global climate change.





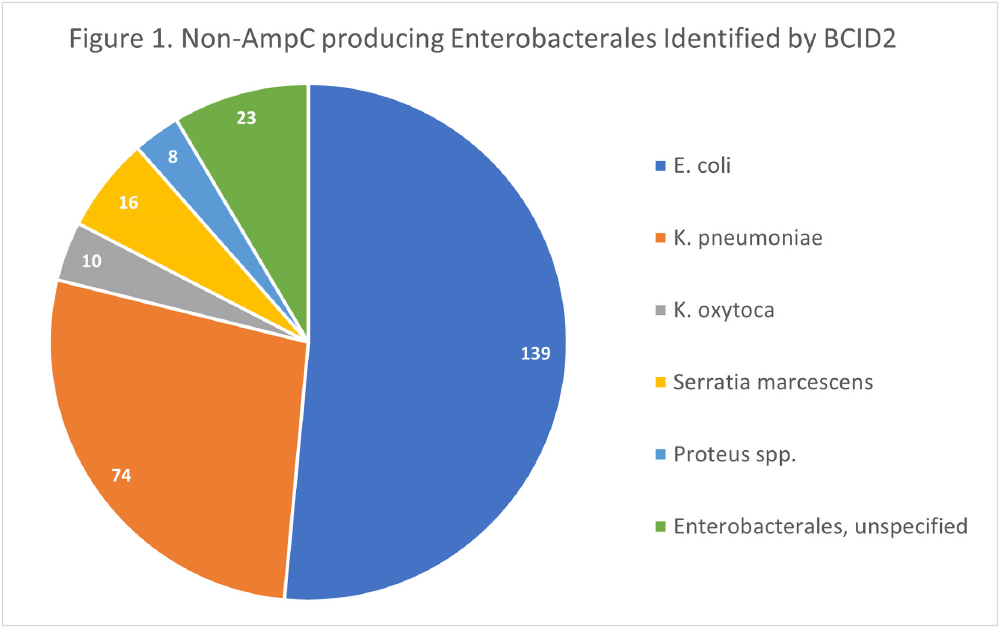
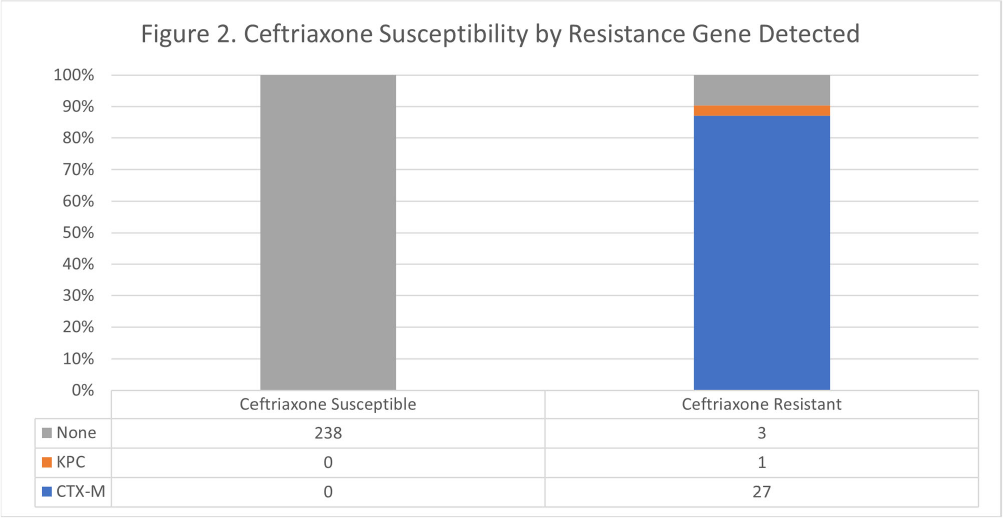
Background: The BioFire FilmArray Blood Culture Identification 2 (BCID2) Panel is used to identify organisms present in positive blood cultures within hours of detection at Virginia Commonwealth University Health System (VCUHS). BCID2 is also able to detect common resistance mechanisms including CTX-M, the most common extended-spectrum beta-lactamase (ESBL) in the United States, and several carbapenemases. The Antimicrobial Stewardship Program (ASP) at VCUHS established optimal treatment recommendations for each organism identified by BCID2 based on the detection of a resistance mechanism and local resistance patterns. The recommendation for the majority of Enterobacterales without a detected resistance mechanism is ceftriaxone. However, providers are often reluctant to de-escalate antibiotics without confirmed susceptibility testing, as there may be other mechanisms of antibiotic resistance in Gram-negative organisms. The objective of this evaluation was to measure the degree of congruence between BCID2 resistance mechanism detection and susceptibility testing by disk diffusion, and to validate the adequacy of the VCUHS ASP BCID2 treatment recommendations for Enterobacterales bacteremia. Methods: Patients with positive Enterobacterales BCID2 results from March 12 to June 19, 2023 were retrospectively identified. Organisms identified by BCID2 that were considered high-risk for clinically significant AmpC production due to an inducible AmpC gene (i.e., K. aerogenes, E. cloacae complex) were excluded. Results: A total of 270 results were included. The most commonly identified organism was E. coli (n = 139, 51.5%), followed by K. pneumoniae (n = 74, 27.4%). There were 27 (10%) isolates positive for CTX-M and 1 (0.4%) isolate positive for KPC. All CTX-M isolates were ceftriaxone resistant, and the KPC isolate was meropenem resistant. The remaining 242 isolates were negative for all resistance markers detected by BCID2. Of these, only 3 (1.2%) were resistant to ceftriaxone and notably, 8 (3.3%) were resistant to piperacillin/tazobactam. Overall, BCID2 CTX-M detection was 90% sensitive and 100% specific for predicting ceftriaxone resistance in Enterobacterales. Conclusion: CTX-M detection by BCID2 is highly sensitive and specific for predicting ceftriaxone resistance in Enterobacterales. CTX-M negative isolates were more often susceptible to ceftriaxone than to piperacillin/tazobactam, which is commonly used as empiric therapy for Gram-negative organisms at our institution. This highlights an excellent opportunity for safe and effective early de-escalation of antibiotics for treatment of Enterobacterales bacteremia.
The quenching of cluster satellite galaxies is inextricably linked to the suppression of their cold interstellar medium (ISM) by environmental mechanisms. While the removal of neutral atomic hydrogen (H i) at large radii is well studied, how the environment impacts the remaining gas in the centres of galaxies, which are dominated by molecular gas, is less clear. Using new observations from the Virgo Environment traced in CO survey (VERTICO) and archival H i data, we study the H i and molecular gas within the optical discs of Virgo cluster galaxies on 1.2-kpc scales with spatially resolved scaling relations between stellar ( $\Sigma_{\star}$), H i (
$\Sigma_{\star}$), H i ( $\Sigma_{\text{H}\,{\small\text{I}}}$), and molecular gas (
$\Sigma_{\text{H}\,{\small\text{I}}}$), and molecular gas ( $\Sigma_{\text{mol}}$) surface densities. Adopting H i deficiency as a measure of environmental impact, we find evidence that, in addition to removing the H i at large radii, the cluster processes also lower the average
$\Sigma_{\text{mol}}$) surface densities. Adopting H i deficiency as a measure of environmental impact, we find evidence that, in addition to removing the H i at large radii, the cluster processes also lower the average  $\Sigma_{\text{H}\,{\small\text{I}}}$ of the remaining gas even in the central
$\Sigma_{\text{H}\,{\small\text{I}}}$ of the remaining gas even in the central  $1.2\,$kpc. The impact on molecular gas is comparatively weaker than on the H i, and we show that the lower
$1.2\,$kpc. The impact on molecular gas is comparatively weaker than on the H i, and we show that the lower  $\Sigma_{\text{mol}}$ gas is removed first. In the most H i-deficient galaxies, however, we find evidence that environmental processes reduce the typical
$\Sigma_{\text{mol}}$ gas is removed first. In the most H i-deficient galaxies, however, we find evidence that environmental processes reduce the typical  $\Sigma_{\text{mol}}$ of the remaining gas by nearly a factor of 3. We find no evidence for environment-driven elevation of
$\Sigma_{\text{mol}}$ of the remaining gas by nearly a factor of 3. We find no evidence for environment-driven elevation of  $\Sigma_{\text{H}\,{\small\text{I}}}$ or
$\Sigma_{\text{H}\,{\small\text{I}}}$ or  $\Sigma_{\text{mol}}$ in H i-deficient galaxies. Using the ratio of
$\Sigma_{\text{mol}}$ in H i-deficient galaxies. Using the ratio of  $\Sigma_{\text{mol}}$-to-
$\Sigma_{\text{mol}}$-to- $\Sigma_{\text{H}\,{\small\text{I}}}$ in individual regions, we show that changes in the ISM physical conditions, estimated using the total gas surface density and midplane hydrostatic pressure, cannot explain the observed reduction in molecular gas content. Instead, we suggest that direct stripping of the molecular gas is required to explain our results.
$\Sigma_{\text{H}\,{\small\text{I}}}$ in individual regions, we show that changes in the ISM physical conditions, estimated using the total gas surface density and midplane hydrostatic pressure, cannot explain the observed reduction in molecular gas content. Instead, we suggest that direct stripping of the molecular gas is required to explain our results.

