We construct an explicit algebraic example of a subshift of finite type over a group  $\Gamma $ with an invariant Markov measure which has completely positive sofic entropy (with respect to ‘most’ sofic approximations) and yet does not have a direct Bernoulli factor because its model spaces shatter into exponentially many clusters of sub-exponential size. The example and its analysis are related to random low-density parity-check (LDPC) codes.
$\Gamma $ with an invariant Markov measure which has completely positive sofic entropy (with respect to ‘most’ sofic approximations) and yet does not have a direct Bernoulli factor because its model spaces shatter into exponentially many clusters of sub-exponential size. The example and its analysis are related to random low-density parity-check (LDPC) codes.
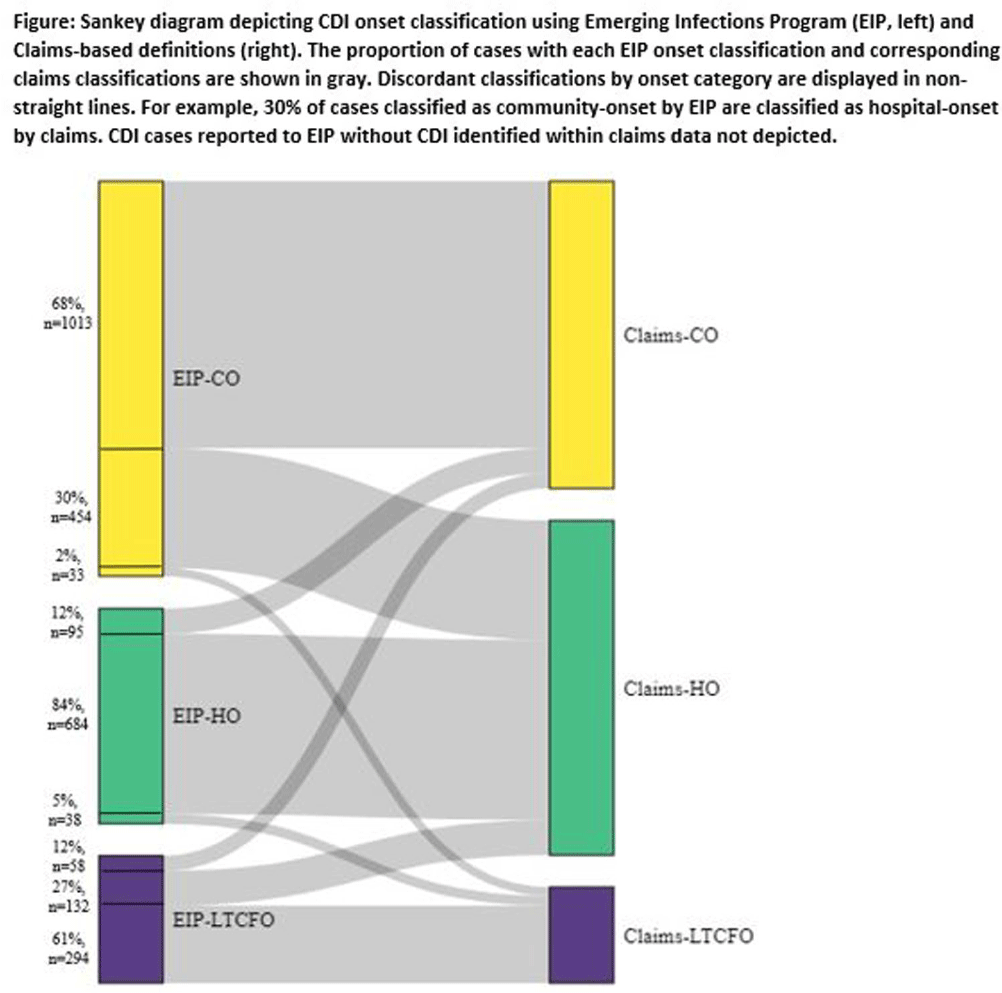
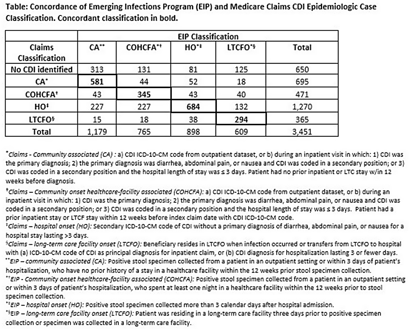
Background: Medicare claims are frequently used to study Clostridioides difficile infection (CDI) epidemiology. Categorizing CDI based on location of onset and potential exposure is critical in understanding transmission patterns and prevention strategies. While claims data are well-suited for identifying prior healthcare utilization exposures, they lack specimen collection and diagnosis dates to assign likely location of onset. Algorithms to classify CDI onset and healthcare association using claims data have been published, but the degree of misclassification is unknown. Methods: We linked patients with laboratory-confirmed CDI reported to four Emerging Infections Program (EIP) sites from 2016-2020 to Medicare beneficiaries using residence, birth date, sex, and hospitalization and/or healthcare exposure dates. Uniquely linked patients with fee-for-service Medicare A/B coverage and complete EIP case report forms were included. Patients with a claims CDI diagnosis code within ±28 days of a positive CDI test reported to EIP were categorized as hospital-onset (HO), long-term care facility onset (LTCFO), or community-onset (CO, either healthcare facility-associated [COHCFA] or community-associated [CA]) using a previously published algorithm based on claim type, ICD-10-CM code position, and duration of hospitalization (if applicable). EIP classifies CDI into these categories using positive specimen collection date and other information from chart review (e.g. admit/discharge dates). We assessed concordance of EIP and claims case classifications using Cohen’s kappa. Results: Of 10,002 eligible EIP-identified CDI cases, 7,064 were linked to a unique beneficiary; 3,451 met Medicare A/B fee-for-service coverage inclusion criteria. Of these, 650 (19%) did not have a claims diagnosis code ±28 days of the EIP specimen collection date (Table); 48% (313/650) of those without a claims diagnosis code were categorized by EIP as CA CDI. Among those with a CDI diagnosis code, concurrence of claims-based and EIP CDI classification was 68% (κ=0.56). Concurrence was highest for HO and lowest for COHCFA CDI. A substantial number of EIP-classified CO CDIs (30%, Figure) were misclassified as HO using the claims-based algorithm; half of these had a primary ICD-10 diagnosis code of sepsis (226/454; 50%). Conclusions: Evidence of CDI in claims data was found for 81% of EIP-reported CDI cases. Medicare classification algorithms concurred with the EIP classification in 68% of cases. Discordance was most common for community-onset CDI patients, many of whom were hospitalized with a primary diagnosis of sepsis. Misclassification of CO-CDI as HO may bias findings of claims-based CDI studies.
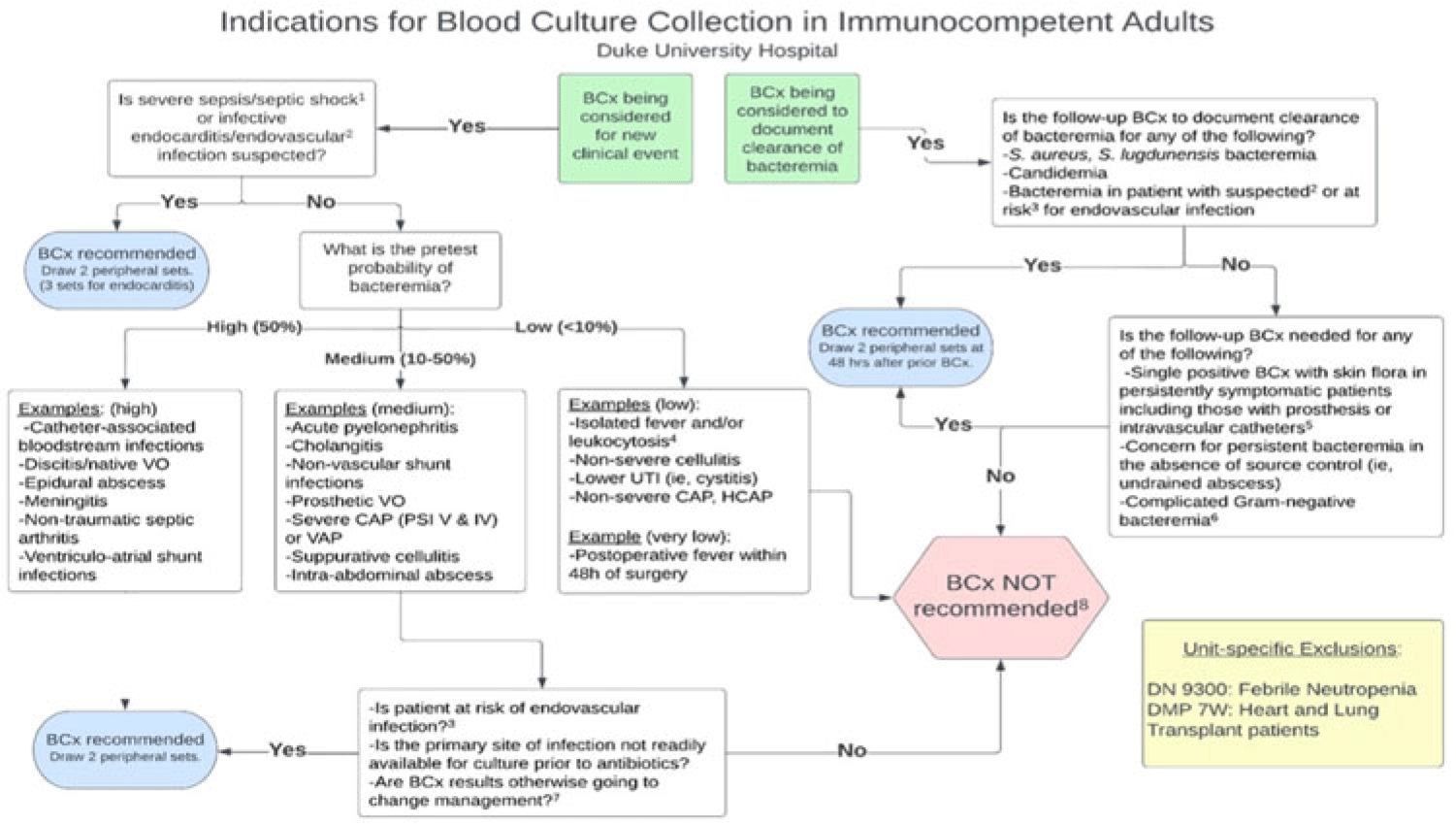
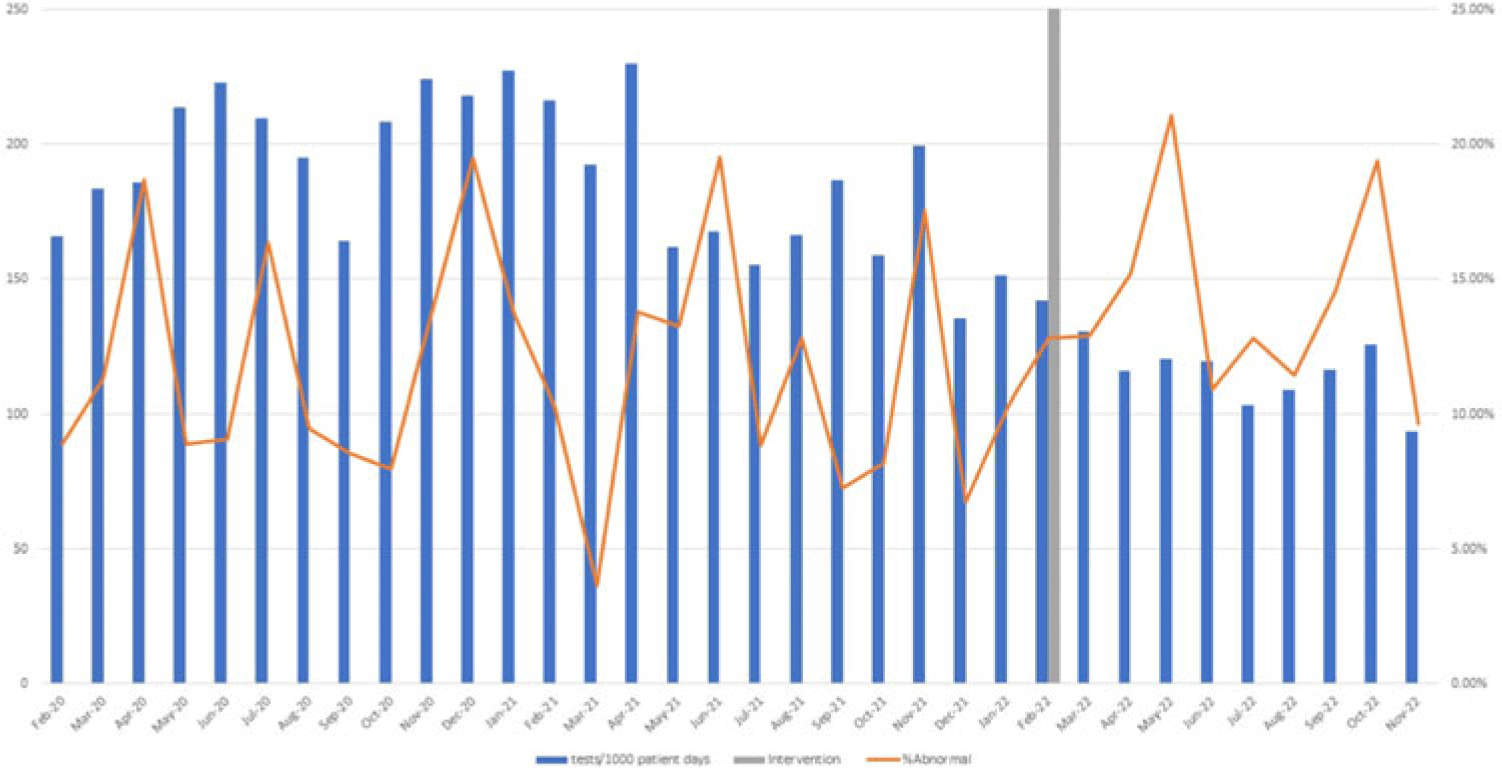
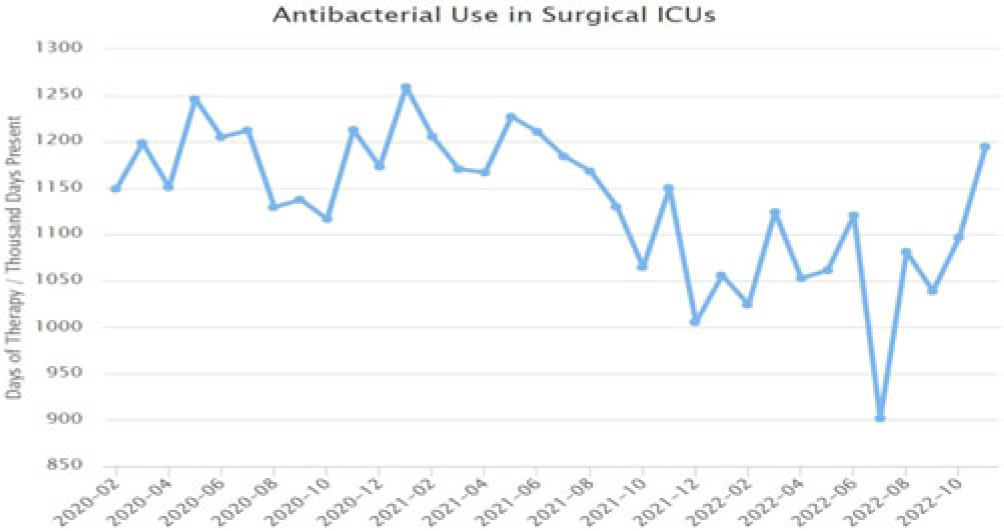
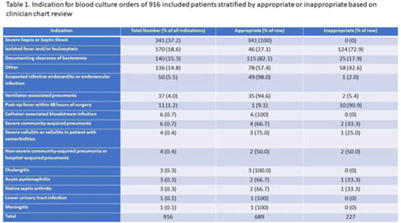
Background: Blood cultures are commonly ordered for patients with low risk of bacteremia. Liberal blood-culture ordering increases the risk of false-positive results, which can lead to increased length of stay, excess antibiotics, and unnecessary diagnostic procedures. We implemented a blood-culture indication algorithm with data feedback and assessed the impact on ordering volume and percent positivity. Methods: We performed a prospective cohort study from February 2022 to November 2022 using historical controls from February 2020 to January 2022. We introduced the blood-culture algorithm (Fig. 1) in 2 adult surgical intensive care units (ICUs). Clinicians reviewed charts of eligible patients with blood cultures weekly to determine whether the blood-culture algorithm was followed. They provided feedback to the unit medical directors weekly. We defined a blood-culture event as ≥1 blood culture within 24 hours. We excluded patients aged <18 years, absolute neutrophil count <500, and heart and lung transplant recipients at the time of blood-culture review. Results: In total, 7,315 blood-culture events in the preintervention group and 2,506 blood-culture events in the postintervention group met eligibility criteria. The average monthly blood-culture rate decreased from 190 blood cultures per 1,000 patient days to 142 blood cultures per 1,000 patient days (P < .01) after the algorithm was implemented. (Fig. 2) The average monthly blood-culture positivity increased from 11.7% to 14.2% (P = .13). Average monthly days of antibiotic therapy (DOT) was lower in the postintervention period than in the preintervention period (2,200 vs 1,940; P < .01). (Fig. 3) The ICU length of stay did not change before the intervention compared to after the intervention: 10 days (IQR, 5–18) versus 10 days (IQR, 5–17; P = .63). The in-hospital mortality rate was lower during the postintervention period, but the difference was not statistically significant: 9.24% versus 8.34% (P = .17). The all-cause 30-day mortality was significantly lower during the intervention period: 11.9% versus 9.7% (P < .01). The unplanned 30-day readmission percentage was significantly lower during the intervention period (10.6% vs 7.6%; P < .01). Over the 9-month intervention, we reviewed 916 blood-culture events in 452 unique patients. Overall, 74.6% of blood cultures followed the algorithm. The most common reasons overall for ordering blood cultures were severe sepsis or septic shock (37%), isolated fever and/or leukocytosis (19%), and documenting clearance of bacteremia (15%) (Table 1). The most common indications for inappropriate blood cultures were isolated fever and/or leukocytosis (53%). Conclusions: We introduced a blood-culture algorithm with data feedback in 2 surgical ICUs and observed decreases in blood-culture volume without a negative impact on ICU LOS or mortality rate.
Disclosure: None

