Background: Infections lead to high mortality among patients on chronic dialysis; knowledge of multi-drug resistant infections is limited. The Centers for Disease Control and Prevention’s Emerging Infections Program (EIP) conducts laboratory- and population-based surveillance for carbapenem-resistant Enterobacterales (CRE) in 10 U.S. sites and carbapenem-resistant Acinetobacter baumannii (CRAB) in 9 U.S. sites. We investigated clinical characteristics, healthcare exposures, and outcomes of CRE and CRAB cases in persons on chronic dialysis from 2016-2021. Methods: Among EIP catchment-area residents on chronic dialysis, we defined a CRE case as the first isolation of Escherichia coli, Enterobacter cloacae complex, Klebsiella aerogenes (formerly Enterobacter aerogenes), Klebsiella oxytoca, Klebsiella pneumoniae, or Klebsiella variicola resistant to any carbapenem, from a normally sterile site or urine in a 30-day period. A CRAB case was defined as the first isolation of Acinetobacter baumannii complex resistant to any carbapenem (excluding ertapenem), from a normally sterile site or urine (or lower respiratory tract or wound since 2021) in a 30-day period. Medical records were reviewed. A case was considered colonized if the case culture had no associated infection type or colonization was documented in the medical record. Descriptive analyses, including analyses stratified by pathogen, were conducted. Results: Among 426 cases, 314 were CRE, and 112 were CRAB; most cases were male (235, 55.2%), Black (229, 53.8%), and 51-80 years old (320, 75.1%) (Table). An infection was associated with 363 (85.2%) case cultures; bloodstream infections (148; 40.8%), urinary tract infections (134; 36.9%), and pneumonia (17; 4.7%) were the most frequent. Overall, most cases had documented healthcare exposures (excluding outpatient dialysis) in the year before incident specimen collection, including: 366 (85.9%) hospitalizations, 235 (55.2%) surgeries, 209 (49.1%) long-term care facility stays, 54 (12.7%) long-term acute care facility stays. Additionally, 125 (29.3%) had an intensive care unit admission within the 7 days before incident specimen collection. Compared to CRE cases, a higher proportion of CRAB cases (a) had a long-term care facility stay (82/112 [73.2%] versus 127/314 [40.5%], P<.0001) or hospitalization (103/112 [92%] versus 263/314 [83.8%], P = .03) within the preceding year and (b) died within 30 days of incident specimen collection (40/112 [35.7%] versus 64/314 [20.4%], P = .001). Discussion: Among CRE and CRAB cases in persons on chronic dialysis, healthcare exposures were common, and mortality was high. Additional efforts to better describe the burden of these organisms and associated risk factors in the dialysis population are needed for tailoring infection prevention strategies to this vulnerable.

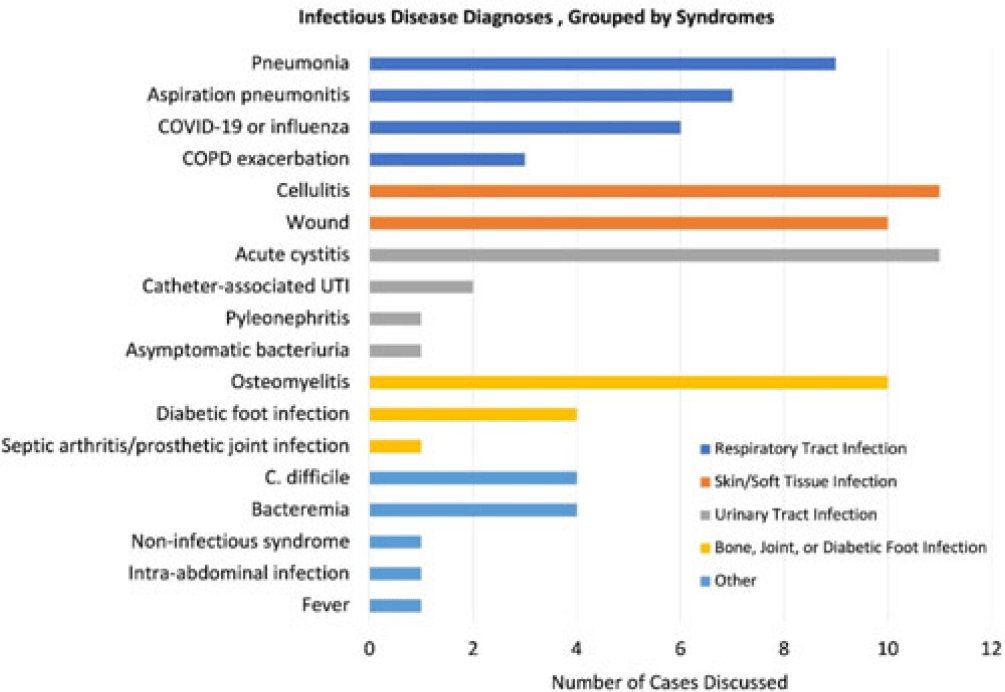
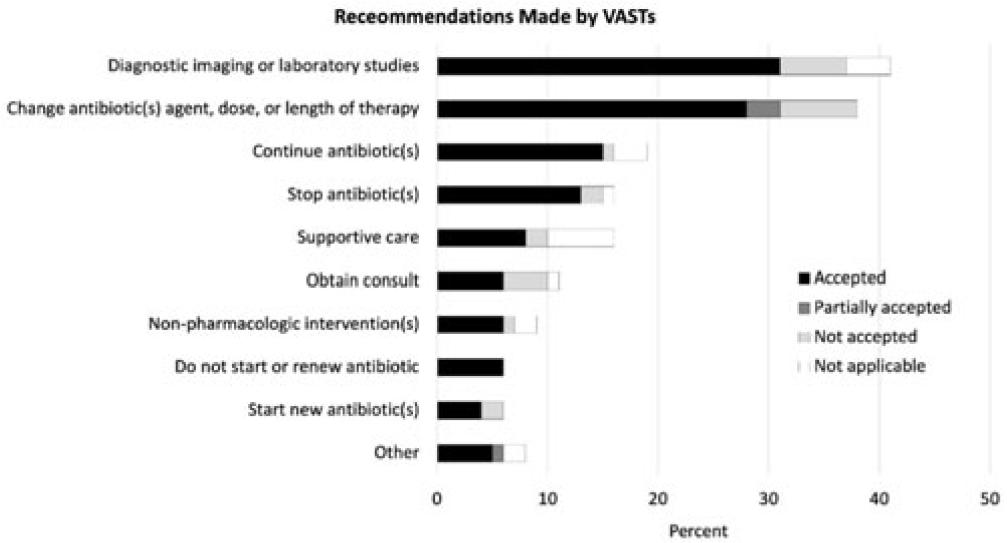
Background: Healthcare settings without access to infectious diseases experts may struggle to implement effective antibiotic stewardship programs. We previously described a successful pilot project using the Veterans Affairs (VA) telehealth system to form a Videoconference Antimicrobial Stewardship Team (VAST) that connected multidisciplinary teams from rural VA medical centers (VAMCs) with infectious diseases experts at geographically distant locations. VASTs discussed patients from the rural VAMC, with the overarching goal of supporting antibiotic stewardship. This project is currently ongoing. Here, we describe preliminary outcomes describing the cases discussed, recommendations made, and acceptance of those recommendations among 4 VASTs. Methods: Cases discussed at any of the 4 participating intervention sites were independently reviewed by study staff, noting the infectious disease diagnoses, recommendations made by infectious diseases experts and, when applicable, acceptance of those recommendations at the rural VAMC within 1 week. Discrepancies between independent reviewers were discussed and, when consensus could not be reached, discrepancies were discussed with an infectious diseases clinician. Results: The VASTs serving 4 different rural VAMCs discussed 96 cases involving 92 patients. Overall, infection of the respiratory tract was the most common syndrome discussed by VASTs (Fig. 1). The most common specific diagnoses among discussed cases were cellulitis (n = 11), acute cystitis (n = 11), wounds (n = 11), and osteomyelitis (n = 10). Of 172 recommendations, 41 (24%) related to diagnostic imaging or laboratory results and 38 (22%) were to change the antibiotic agent, dose, or duration (Fig. 2). Of the 151 recommendations that could be assessed via chart review, 122 (81%) were accepted within 1 week. Conclusions: These findings indicate successful implementation of telehealth to connect clinicians at rural VAMCs with an offsite infectious diseases expert. The cases represented an array of common infectious syndromes. The most frequent recommendations pertained to getting additional diagnostic information and to adjusting, but not stopping, antibiotic therapy. These results suggest that many of the cases discussed warrant antibiotics and that VASTs may use the results of diagnostic studies to tailor that therapy. The high rate of acceptance suggests that the VASTs are affecting patient care. Future work will describe VAST implementation at 4 additional VAMCs, and we will assess whether using telehealth to disseminate infectious diseases expertise to rural VAMCs supports changes in antibiotic use that align with principles of antimicrobial stewardship.
Disclosures: None

