In individuals with first episode psychosis (FEP) and cannabis use disorder (CUD), reducing cannabis use is associated with improved clinical outcomes. Access to evidence-based psychological interventions to decrease cannabis use in FEP clinics is highly variable; E-mental health interventions may help to address this gap. Development of E-interventions for CUD in individuals with FEP is in its incipient phases.
To assess preferences for online psychological interventions aiming at decreasing or stopping cannabis use in young adults with psychosis and CUD.
Individuals aged 18 to 35 years old with psychosis and CUD were recruited from seven FEP intervention programs in Canada and responded to an electronic survey between January 2020-July 2022. We used the Case 2 Best Worst Scaling methodology that is grounded in the trade-off utility concept to collect and analyse data. Participants selected the best or worst option for each of the nine questions corresponding to three distinct domains. For each domain we used conditional logistic regression and marginal models (i.e., three models in total) to estimate preferences for attributes (e.g., duration, frequency of online intervention sessions) and attribute levels (e.g., 15 minutes, every day).
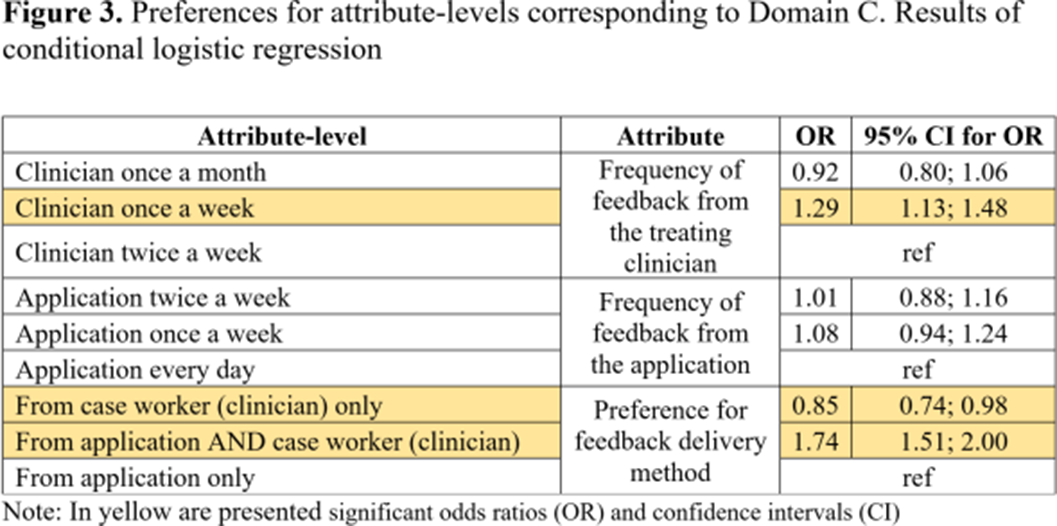
Participants (N=104) showed higher preferences for the following attributes: duration of online sessions; mode of receiving the intervention; method of feedback delivery and the frequency of feedback from clinicians (Table 1). Attribute-level analyses showed higher preferences for participating once a week in short (15 minutes) online interventions (Figure 1). Participants valued the autonomy offered by online interventions which aligns with their preference for completing the intervention outside the clinic and only require assistance once a week (Figure 2). Participants’ preferences were higher for receiving feedback related to cannabis consumption both from the application and clinicians at a frequency of once a week from clinicians (Figure 3). Note: In boldface significant odds ratios (OR) and confidence intervals (CI)Attributes Domains OR 95% CI for OR Duration session A 1.62 1.45; 1.82 Frequency sessions 0.98 0.87; 1.09 Duration intervention ref Preferred mode of receiving the intervention B 1.63 1.46; 1.83 Preferred location for participating 1.07 0.96; 1.20 Frequency of assistance from the clinician ref Preference for the feedback delivery method C 1.21 1.08; 1.36 Frequency of feedback from the treating clinician 1.14 1.02; 1.28 Frequency of feedback from the application ref
Image:
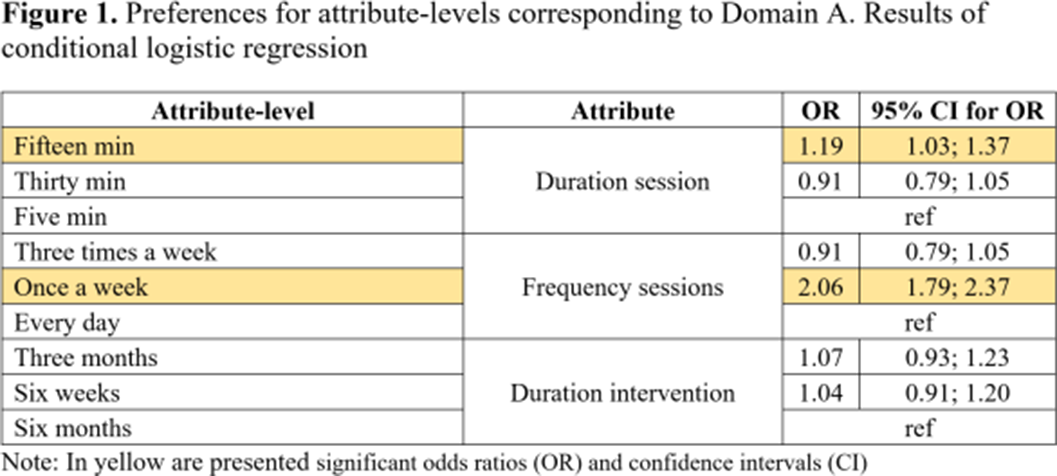
Image 2:
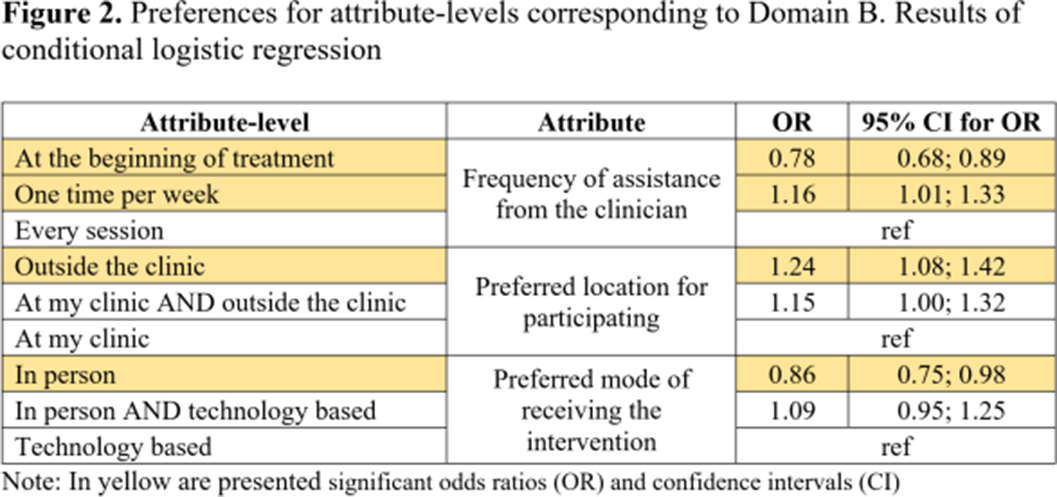
Image 3:
Using advanced methodologies to assess preferences, our results can inform the development of highly acceptable E-Mental health interventions for decreasing cannabis use in individuals with CUD and FEP.
None Declared
We present analysis of the far ultraviolet (FUV) emission of sources in the central region of the Coma cluster ( $z=0.023$) using the data taken by the UVIT aboard the multi-wavelength satellite mission AstroSat. We find a good correlation between the UVIT FUV flux and the fluxes in both wavebands of the Galex mission, for the common sources. We detect stars and galaxies, amongst which the brightest (
$z=0.023$) using the data taken by the UVIT aboard the multi-wavelength satellite mission AstroSat. We find a good correlation between the UVIT FUV flux and the fluxes in both wavebands of the Galex mission, for the common sources. We detect stars and galaxies, amongst which the brightest ( $r \lesssim 17$ mag) galaxies in the field of view are mostly members of the Coma cluster. We also detect three quasars (
$r \lesssim 17$ mag) galaxies in the field of view are mostly members of the Coma cluster. We also detect three quasars ( $z = 0.38, 0.51, 2.31$), one of which is likely the farthest object observed by the UVIT so far. In almost all the optical and UV colour-colour and colour-magnitude planes explored in this work, the Coma galaxies, other galaxies and bright stars could be separately identified, but the fainter stars and quasars often coincide with the faint galaxies. We have also investigated galaxies with unusual FUV morphology which are likely to be galaxies experiencing ram-pressure stripping in the cluster. Amongst others, two confirmed cluster members which were not investigated in the literature earlier, have been found to show unusual FUV emission. All the distorted sources are likely to have fallen into the cluster recently, and hence have not virialised yet. A subset of our data have optical spectroscopic information available from the archives. For these sources (
$z = 0.38, 0.51, 2.31$), one of which is likely the farthest object observed by the UVIT so far. In almost all the optical and UV colour-colour and colour-magnitude planes explored in this work, the Coma galaxies, other galaxies and bright stars could be separately identified, but the fainter stars and quasars often coincide with the faint galaxies. We have also investigated galaxies with unusual FUV morphology which are likely to be galaxies experiencing ram-pressure stripping in the cluster. Amongst others, two confirmed cluster members which were not investigated in the literature earlier, have been found to show unusual FUV emission. All the distorted sources are likely to have fallen into the cluster recently, and hence have not virialised yet. A subset of our data have optical spectroscopic information available from the archives. For these sources ( ${\sim} 10\%$ of the sample), we find that 17 galaxies identify as star-forming, 18 as composite and 13 as host galaxies for active galactic nuclei, respectively on the emission-line diagnostic diagram.
${\sim} 10\%$ of the sample), we find that 17 galaxies identify as star-forming, 18 as composite and 13 as host galaxies for active galactic nuclei, respectively on the emission-line diagnostic diagram.

