The elderly represents the fastest growing group of the population. It is fair to assume that the portion of old age patients suffering from bipolar disorder will grow in a similar manner. Elderly patients represent approximately 25% of the bipolar population. Summarizing, 5–10% of patients were 50 years of age when they experienced their first manic episode, constituting the subgroup of late onset bipolar disorder (LOBD).
The purpose of this case report and literature review is to emphasise the importance of LOBD in old population and to highlight its still sparse-knowledge.
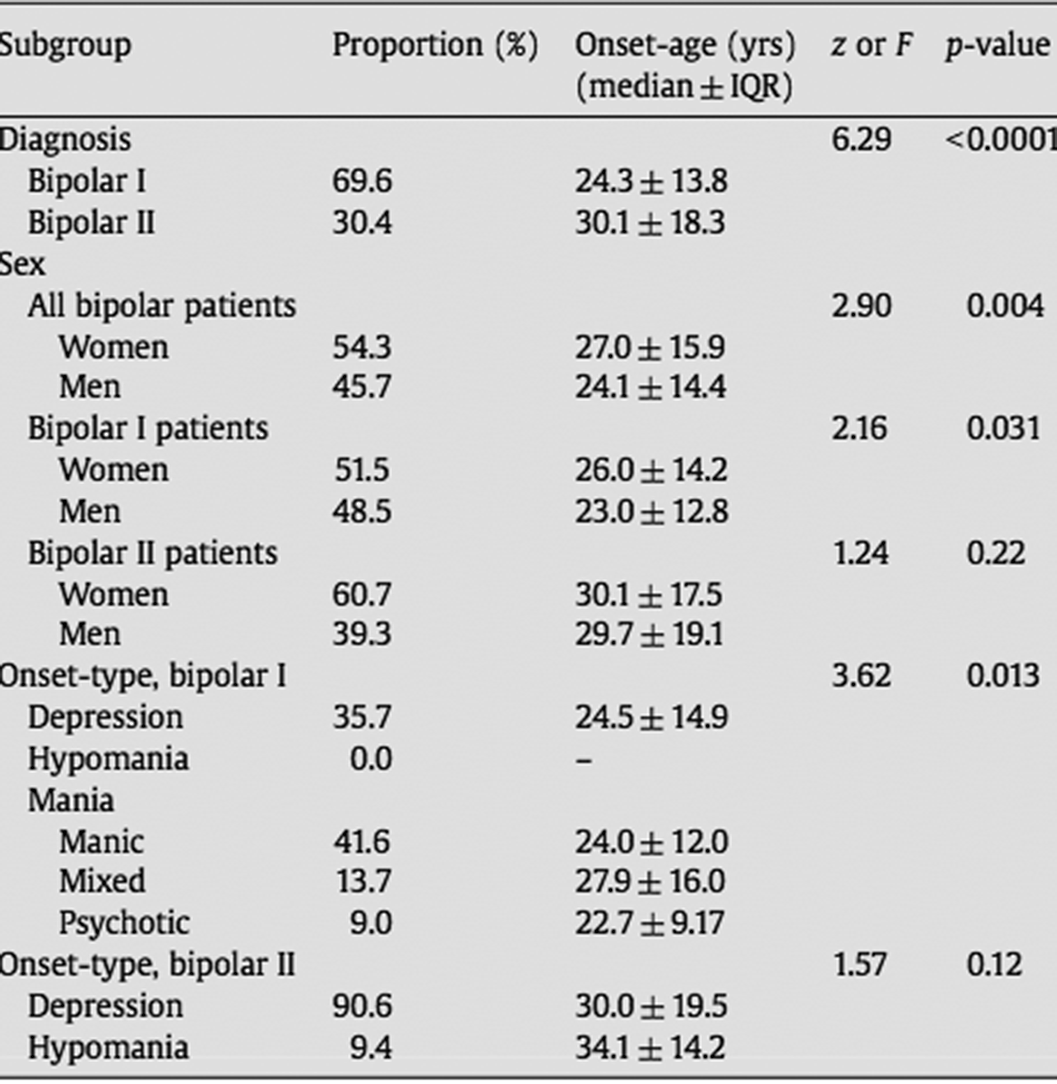
Descriptive case study and review of literature (Arnold,I. et al. Old Age Bipolar Disorder—Epidemiology, Aetiology and Treatment. Medicina 2021,57,587; Baldessarini et al. Onset-age of bipolar disorders at six international sites. J Affect Disord 2010;121(1-2):143-6).
A 60-year-old woman is brought to the emergency department for evaluation by her family. Over the past 7 days, the patient has become increasingly irritable and argumentative, is sleeping less, is talking faster than usual and has begun to express paranoid concerns about her students “stealing my exam”. The patient is a university professor.
In the assessment interview she is hyperverbal, expansive, and grandiose. The family has also just recently discovered that she has spent a large sum of money on the Internet.
She has no history of psychiatric contact or substance use disorders; however, she has a family history of severe depression.
In the absence of any plausible non-psychiatric condition that could mimic or induce mania, the working diagnosis is bipolar I disorder, most recent episode (MRE) manic with psychotic features.
Image:
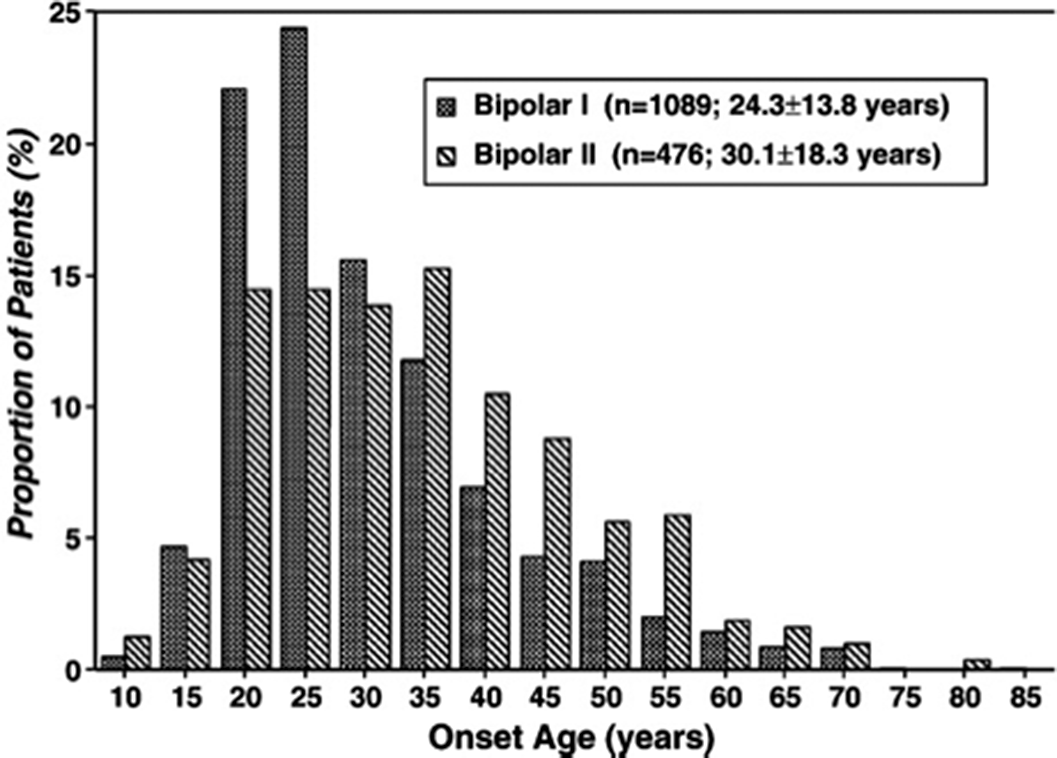
Image 2:
The share of older age bipolar disorder will grow constantly in the next decades and further research on this neglected patient group is urgently required.
None Declared
Traditionally, psychiatric wards had established a “locked door” policy but secluded conditions may increase patient’s discomfort1 that could affect the perception of health quality of care2. Recently, the “open-door” policy is being adopted in several European countries but its impact on patient satisfaction remains unknown (Schreiber, LK. BMC Psychiatry. 2019 May 14;19(1):149). Since 2019 our psychiatric hospital has implemented the open-door policy.
The aim of this study is to investigate the impact of the “open-door” policy on patient satisfaction during their stay in the acute inpatient unit of our psychiatric hospital.
This is an observational study. Prior to the implementation of the open door policy 31 patient satisfaction data was collected between October 2018 to April 2019 and it was also assessed with 31 subjects between July to October 2019, after the implementation of the open “door-policy”. The inclusion criteria were being >18 years old, reading Spanish correctly and with a length of stay >72 hours. The patients with dementia disorder and intellectual disability where excluded from the study. We used the Satispsy-22-E scale, a self-administered questionnaire (Frías, V., et al. 2018. Psychiatry Res. Oct;268:8-14). It assesses patient’s experience of hospitalization through 22 items distributed into 6 dimensions. The score range is from 0 to 100. Differences in Satispsy-22-E scores were analysed by applying ANOVA using the IBM-SPSS (v. 25).
Total scores in Satispsy-22 are provided in Figure 1. We found that patient satisfaction was increased in the dimensions of “personal experience” and “food” (p<0.05). No significant differences were found in staff, quality of care, information, activity dimensions and Total score (Table 2).Dimension F-Test Statistic Value Staff 1.402 p=0.241 Quality of Care 841 p=0.362 Personal Experience 4.071 p=0.048* Information 656 p=0.420 Activity 434 p=0.512 Food 4.507 p=0.037* TOTAL 3.645 p=0.61
Image:
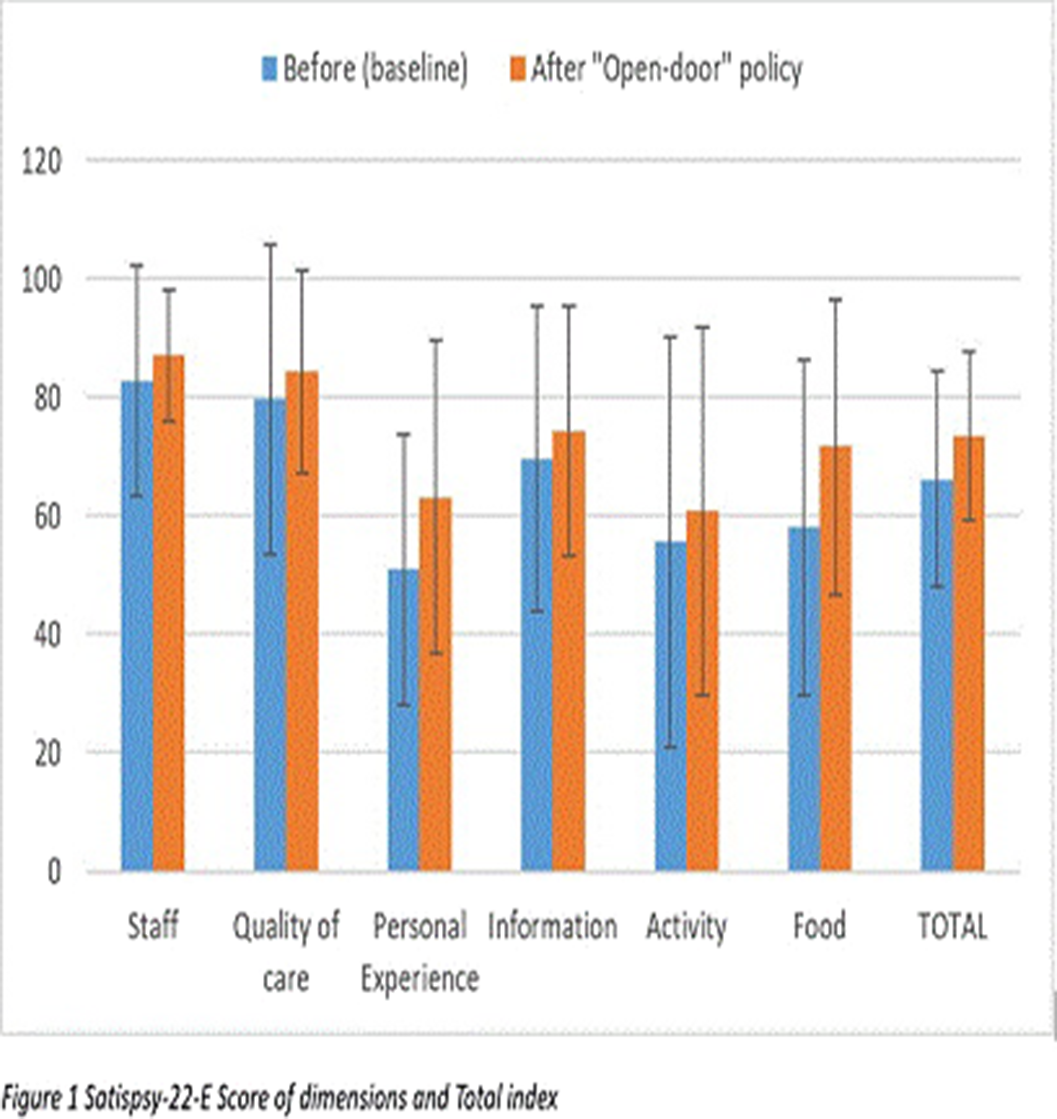
Our results provide preliminary evidence indicating that the open-door policy could have a positive impact on patient satisfaction, especially in relation to the personal experience on an acute inpatient psychiatric unit.
None Declared
New orbit-averaged equations for low collisionality neoclassical fluxes in large aspect ratio stellarators with mirror ratios close to unity are derived. The equations retain finite orbit width effects by employing the second adiabatic invariant $J$ as a velocity-space coordinate and they have been implemented in the orbit-averaged neoclassical code KNOSOS (Velasco et al., J. Comput. Phys., vol. 418, 2020, 109512; Velasco et al., Nucl. Fusion, vol. 61, 2021, 116013). The equations are used to study the $1/\nu$
as a velocity-space coordinate and they have been implemented in the orbit-averaged neoclassical code KNOSOS (Velasco et al., J. Comput. Phys., vol. 418, 2020, 109512; Velasco et al., Nucl. Fusion, vol. 61, 2021, 116013). The equations are used to study the $1/\nu$ regime and the lower collisionality regimes. For generic large aspect ratio stellarators with mirror ratios close to unity, as the collision frequency decreases, the $1/\nu$
regime and the lower collisionality regimes. For generic large aspect ratio stellarators with mirror ratios close to unity, as the collision frequency decreases, the $1/\nu$ regime transitions directly into the $\nu$
regime transitions directly into the $\nu$ regime, without passing through a $\sqrt {\nu }$
regime, without passing through a $\sqrt {\nu }$ regime. An explicit formula for the neoclassical fluxes in the $\nu$
regime. An explicit formula for the neoclassical fluxes in the $\nu$ regime is obtained. The formula includes the effect of particles that transition between different types of wells. While these transitions produce stochastic scattering independent of the value of the collision frequency in velocity space, the diffusion in real space remains proportional to the collision frequency. The $\sqrt {\nu }$
regime is obtained. The formula includes the effect of particles that transition between different types of wells. While these transitions produce stochastic scattering independent of the value of the collision frequency in velocity space, the diffusion in real space remains proportional to the collision frequency. The $\sqrt {\nu }$ regime is only recovered in large aspect ratio stellarators close to omnigeneity: large aspect ratio stellarators with large mirror ratios and optimized large aspect ratio stellarators with mirror ratios close to unity. Neoclassical transport in large aspect ratio stellarators with large mirror ratios can be calculated with the orbit-averaged equations derived by Calvo et al. (Plasma Phys. Control. Fusion, vol. 59, 2017, 055014). In these stellarators, the $\sqrt {\nu }$
regime is only recovered in large aspect ratio stellarators close to omnigeneity: large aspect ratio stellarators with large mirror ratios and optimized large aspect ratio stellarators with mirror ratios close to unity. Neoclassical transport in large aspect ratio stellarators with large mirror ratios can be calculated with the orbit-averaged equations derived by Calvo et al. (Plasma Phys. Control. Fusion, vol. 59, 2017, 055014). In these stellarators, the $\sqrt {\nu }$ regime exists in the collisionality interval $(a/R) \ln (R/a) \ll \nu _{ii} R a/\rho _i v_{ti} \ll R/a$
regime exists in the collisionality interval $(a/R) \ln (R/a) \ll \nu _{ii} R a/\rho _i v_{ti} \ll R/a$ . In optimized large aspect ratio stellarators with mirror ratios close to unity, the $\sqrt {\nu }$
. In optimized large aspect ratio stellarators with mirror ratios close to unity, the $\sqrt {\nu }$ regime occurs in an interval of collisionality that depends on the deviation from omnigeneity $\delta$
regime occurs in an interval of collisionality that depends on the deviation from omnigeneity $\delta$ : $\delta ^{2} |\ln \delta | \ll \nu _{ii} R a/\rho _i v_{ti} \ll 1$
: $\delta ^{2} |\ln \delta | \ll \nu _{ii} R a/\rho _i v_{ti} \ll 1$ . Here, $\nu _{ii}$
. Here, $\nu _{ii}$ is the ion–ion collision frequency, $\rho _i$
is the ion–ion collision frequency, $\rho _i$ and $v_{ti}$
and $v_{ti}$ are the ion gyroradius and thermal speed, and $a$
are the ion gyroradius and thermal speed, and $a$ and $R$
and $R$ are the minor and major radii.
are the minor and major radii.

