The reform of mental health care is a key health policy target. Mental health care provision in Spain is designed with national and regional strategies that stablish the objectives to develop. The Castilla y Leon regional strategy 2022-2026 aim to stabilsh the priorities for objectives and actions with stakeholders from th eregional society.
To evaluate priorities in the implementation of a Mental Health strategy with the consensus of professionals and society.
An initial consensus was achieved with the regional health goverment and local mental health representatives, considering the 2022-2026 national strategy and other mental health plans from nearby regions. Lines in the strategy included transversal lines (part of all the mental health scope) and action lines (priorities focused in one relevant field)
Priorities were stablished by different representatives from mental health and other healthcare professionals, social and educational stakeholders, scientific societies, people with mental health disorders and families. After agreeing to participate in the process, they had to answer an online survey. For each line, they have to score from 0 to 10.
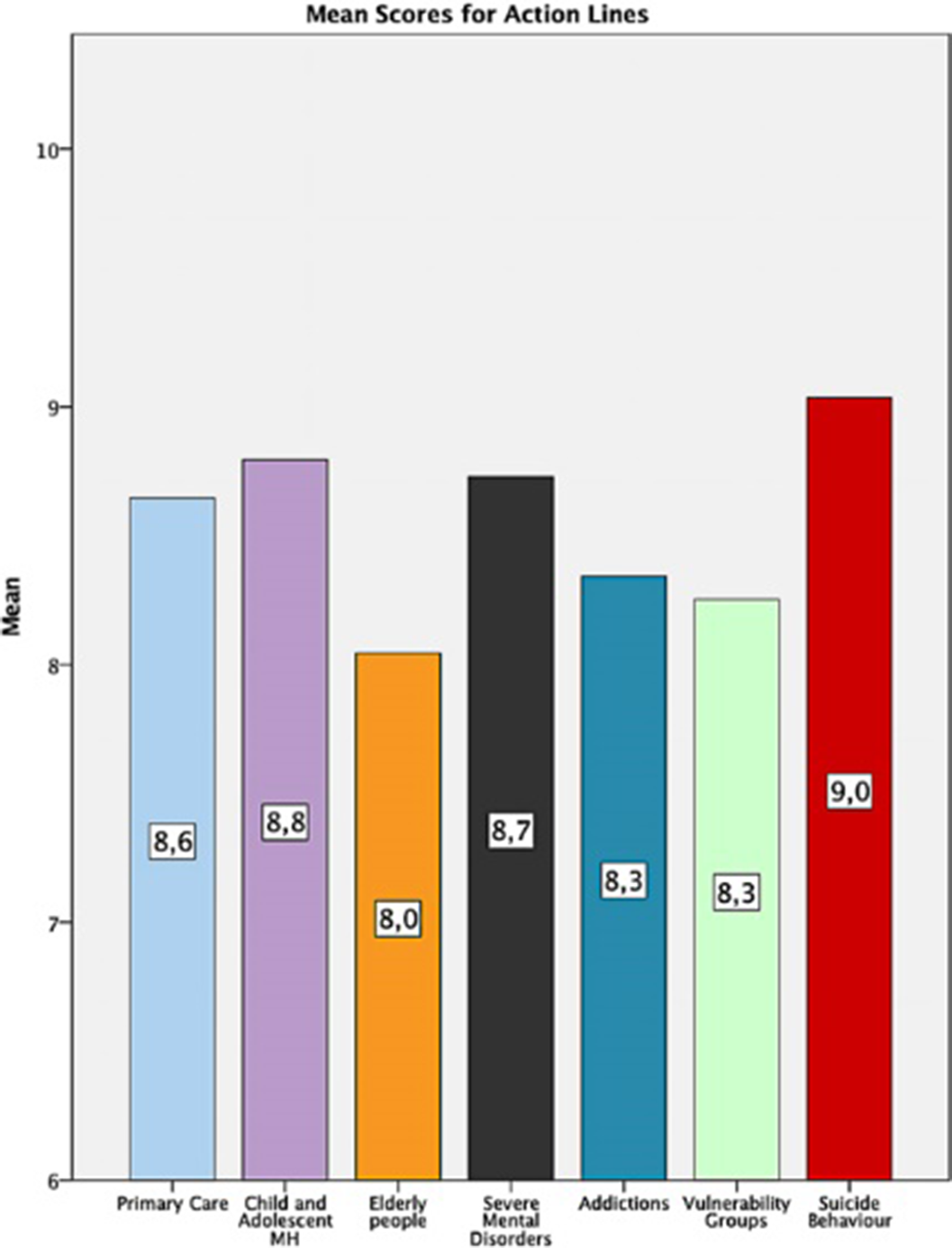
500 subjects participated (44% Healthcare workers, 5.8% education or social services, 3.8% Justice, 8,6% workers for associations, 14% Mental Health Care users). All the lines were highly appreciated (mean score >7). Within the transversal lines, the highest score was for the Humanization line (8.81±1.43) and the lowest for the Digitalization line (7.18±1.92). In the Action Lines, the highest score was for Suicide (9.03±11.5) and the lowest for Elder people (8.04±1.94).
Prevention line had higher scores by Education, Justice, Associations and Healthcare professionals and the lowest was for users (F: 2.754; p=0.012). In the Digitalization line the higher scores were in the health professionals and scientific societies and the lowest in the users (F:4.665; p<0.001). In the research, innovation and Training line, the higher scores were for professionals, societies and users and the lowest in the education and justice groups. The only differences found in the Action lines was for the Addiction line, with higher scores for societies, social services, professionals and users and lower in Associations and Justice (F:2.219; p=0,040)
Image:
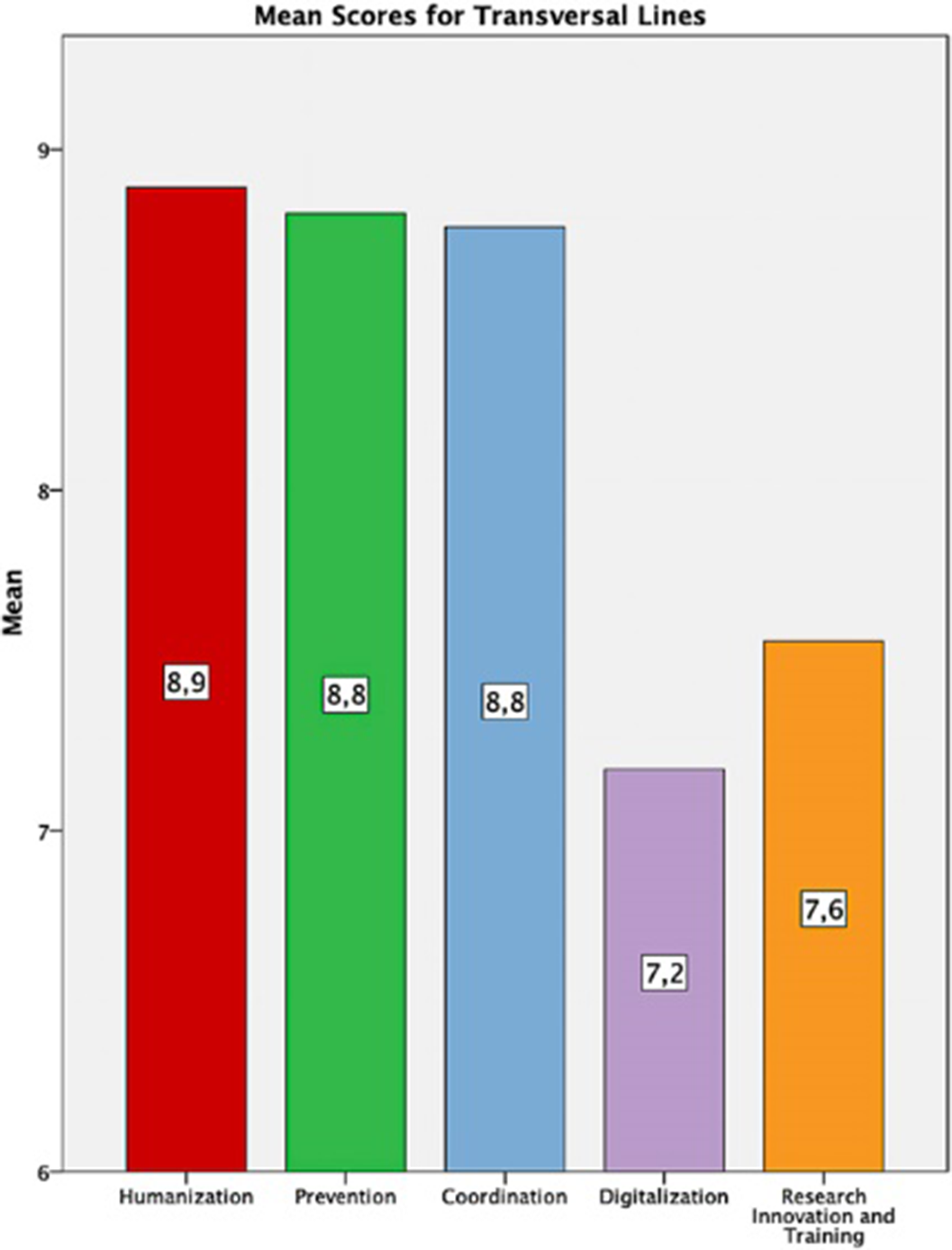
Image 2:
Highest transversal priority for the MH Strategy was Humanization of Mental Health Services, and the most critical action was Suicide prevention. Professionals, Scientific societies and Users considered more important research, innovation and training compared with other society groups, whereas the less important areas for the users were digitalization and prevention users. These priorities will help to design the implementation and schedule for the lines of the Mental Health Strategy in Castilla y León.
None Declared
Humanization in Mental Health is a concept that treat to conceal in the last decades the quality, efficiency and safety of care of complex diseases and conditions with individual values, needs and preferences and involves the patient and society in the decision-making priority.
to stablish and evaluate the priorities of different groups of interest in the development of a new humanization plan for mental health
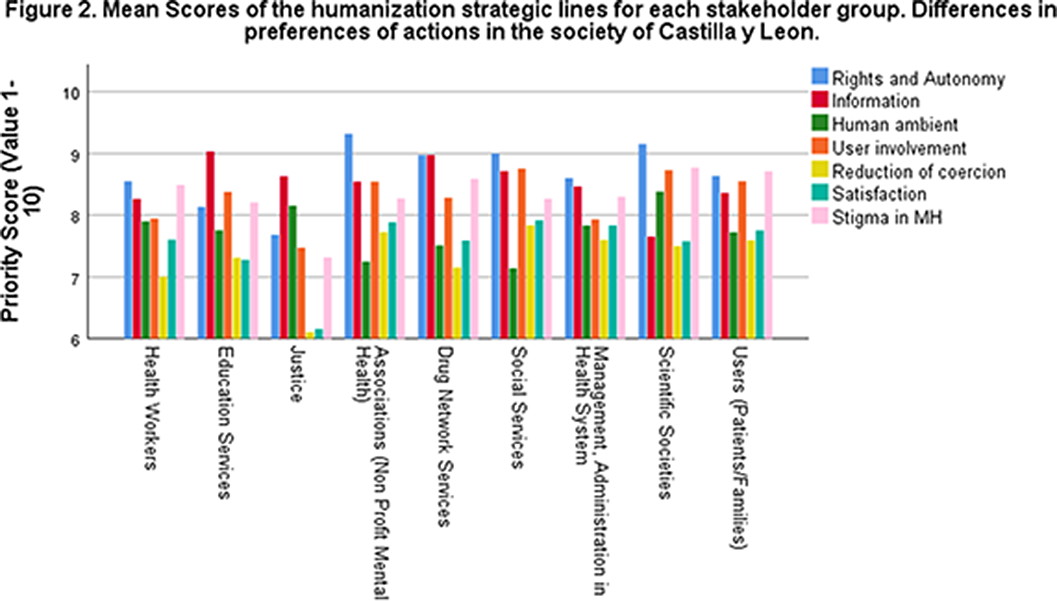
During 2022 a Humanization plan for the Spanish region of Castilla y Leon (2.400.000 habs) was developed with a Delphi model. Participants included 36 stakeholders including mental health services, administration, social services, associations, patients and families. They stablished 32 objectives distributed in 7 strategic lines: 1. “People First” (Rights, Autonomy and Information); 2. “From People to Services” (Participation of users in mental heal services); 3. “Person-Centered-Assistance” 4. “Processes sensible to change” (reduction of coercion); 5. “Human ambient” (Improvement of units, psychosocial interventions). 6. Innovation, training and climate (not evaluated here). 7. “People without marks” (battle against stigma).
Priorities in the lines were stablished by representatives from mental health and other healthcare professionals, social and educational stakeholders, scientific societies, patients and families. After agreeing to participate in the process, they had to answer an online survey. For each line, they have to score it from 0 to 10.
500 subjects participated (38.6% Healthcare workers, 14% Mental Health Care users, 9.8% Social Services, 8.8% Associations, 7.8% Drug Services 6% Management of Health System, 5.8% Education Services, 3.8 Justice). Humanization was the most appreciated plan within the mental health plan 2022-2026 in Castilla y Leon (8.81±1.43).
The Highest priority score was given to the Rights (8.68 + 1.54), Information (8.44 + 1.60) and Stigma (8.43 + 1.89) lines and the lowest were the evaluation of satisfaction (7.62 + 1.90) and Reduction of Coercion (7.29 + 2.12). Differences were found between groups. Scores in Rights and Autonomy (F:3.474; p<0.001) were highest in the Associations (9.32 +1.01) and lowest in the Justice group (7.68 + 1.67). In the information line the highest score (F:2.431; p=0,014) was in the Education Services (9.03 +0,94) compared to Scientific Societies (7,65 + 2,13). Highest score for Participation of Users (F:2,968; p=0,003) was in Social Services (8.76 +1.48) compared to Justice (7.47 +1.95). There were differences in the coercion reduction line (F:2.165; p=0,029) but no pairwise differences were found
Image:
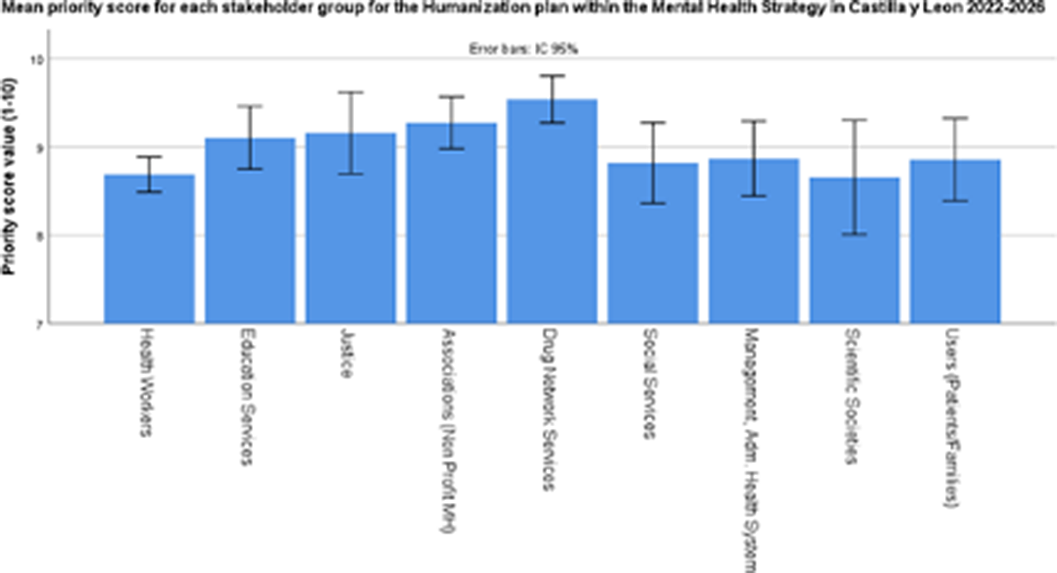
Image 2:
Humanization approaches are well appreciated by different stakeholders. Priorities in our region start with rights, information and integration and mental health users in the health system and society
None Declared

