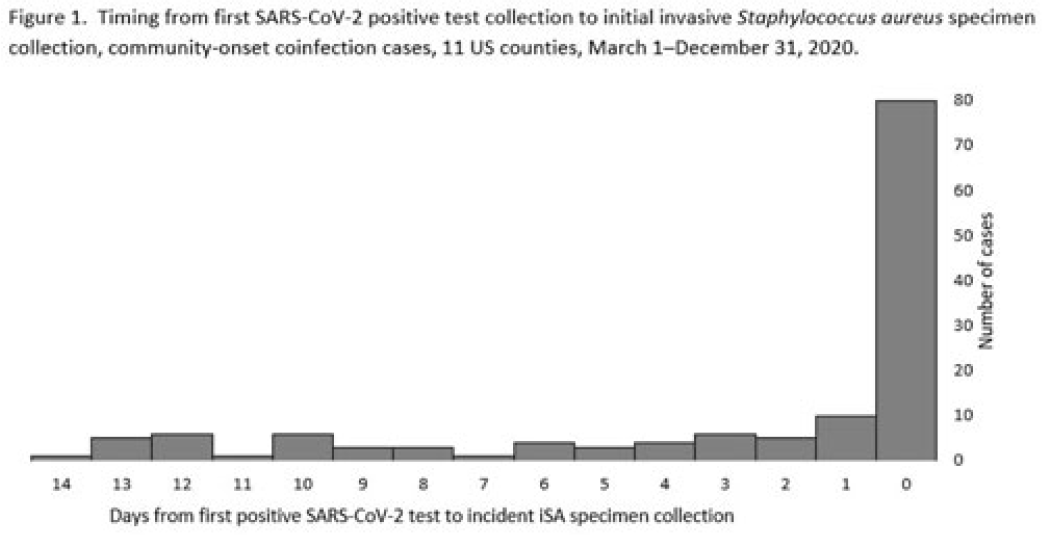
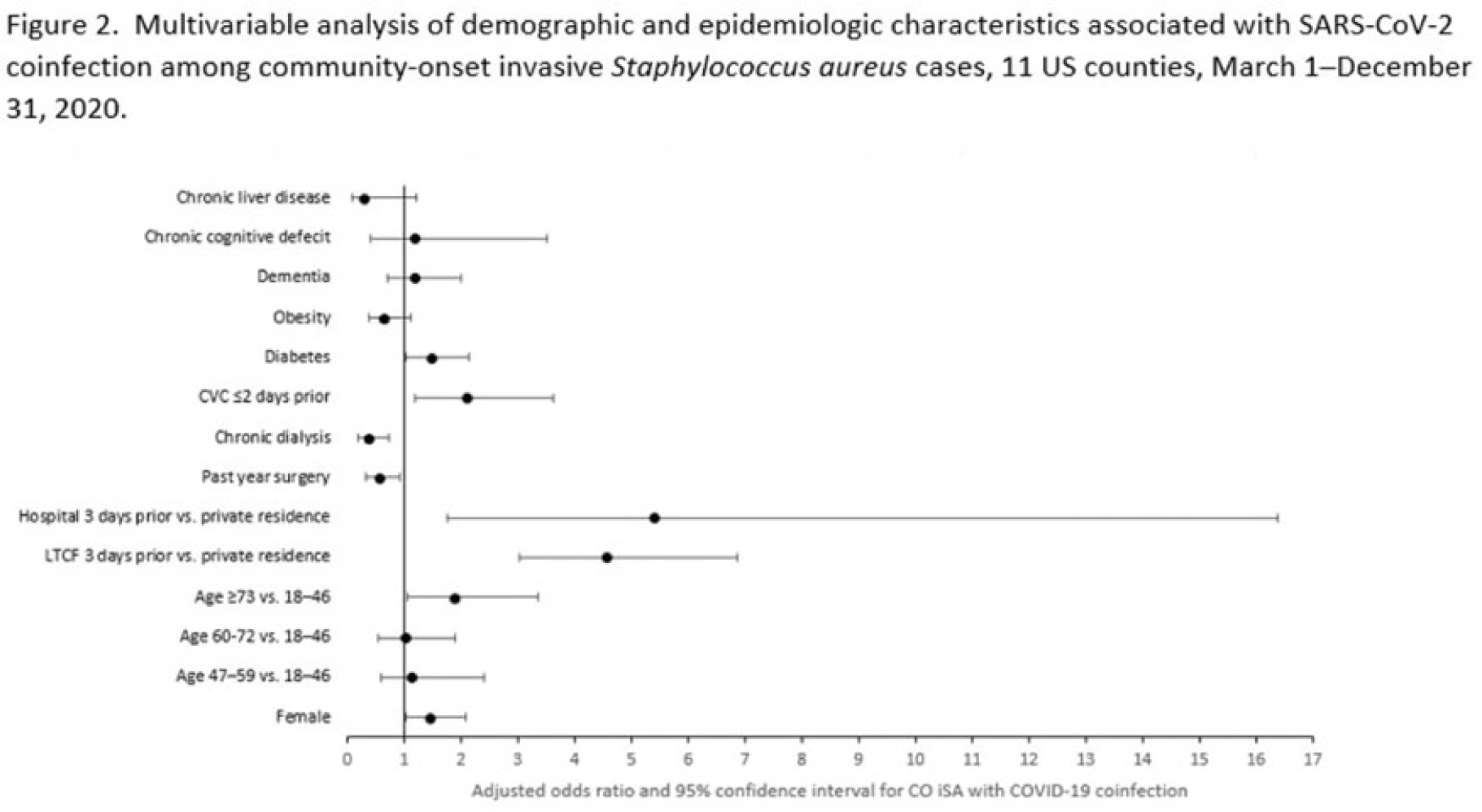
Background: Previous analyses describing the relationship between SARS-CoV-2 infection and Staphylococcus aureus have focused on hospital-onset S. aureus infections occurring during COVID-19 hospitalizations. Because most invasive S. aureus (iSA) infections are community-onset (CO), we characterized CO iSA cases with a recent positive SARS-CoV-2 test (coinfection). Methods: We analyzed CDC Emerging Infections Program active, population- and laboratory-based iSA surveillance data among adults during March 1–December 31, 2020, from 11 counties in 7 states. The iSA cases (S. aureus isolation from a normally sterile site in a surveillance area resident) were considered CO if culture was obtained <3 days after hospital admission. Coinfection was defined as first positive SARS-CoV-2 test ≤14 days before the initial iSA culture. We explored factors independently associated with SARS-CoV-2 coinfection versus no prior positive SARS-CoV-2 test among CO iSA cases through a multivariable logistic regression model (using demographic, healthcare exposure, and underlying condition variables with P<0.25 in univariate analysis) and examined differences in outcomes through descriptive analysis. Results: Overall, 3,908 CO iSA cases were reported, including 138 SARS-CoV-2 coinfections (3.5%); 58.0% of coinfections had iSA culture and the first positive SARS-CoV-2 test on the same day (Fig. 1). In univariate analysis, neither methicillin resistance (44.2% with coinfection vs 36.5% without; P = .06) nor race and ethnicity differed significantly between iSA cases with and without SARS-CoV-2 coinfection (P = .93 for any association between race and ethnicity and coinfection), although iSA cases with coinfection were older (median age, 72 vs 60 years , P<0.01) and more often female (46.7% vs 36.3%, P=0.01). In multivariable analysis, significant associations with SARS-CoV-2 coinfection included older age, female sex, previous location in a long-term care facility (LTCF) or hospital, presence of a central venous catheter (CVC), and diabetes (Figure 2). Two-thirds of co-infection cases had ≥1 of the following characteristics: age > 73 years, LTCF residence 3 days before iSA culture, and/or CVC present any time during the 2 days before iSA culture. More often, iSA cases with SARS-CoV-2 coinfection were admitted to the intensive care unit ≤2 days after iSA culture (37.7% vs 23.3%, P<0.01) and died (33.3% vs 11.3%, P<0.01). Conclusions: CO iSA patients with SARS-CoV-2 coinfection represent a small proportion of CO iSA cases and mostly involve a limited number of factors related to likelihood of acquiring SARS-CoV-2 and iSA. Although CO iSA patients with SARS-CoV-2 coinfection had more severe outcomes, additional research is needed to understand how much of this difference is related to differences in patient characteristics.
Disclosures: None
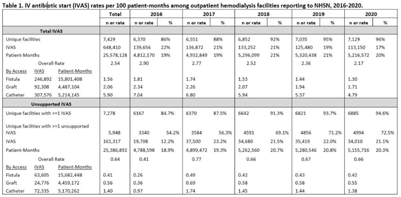
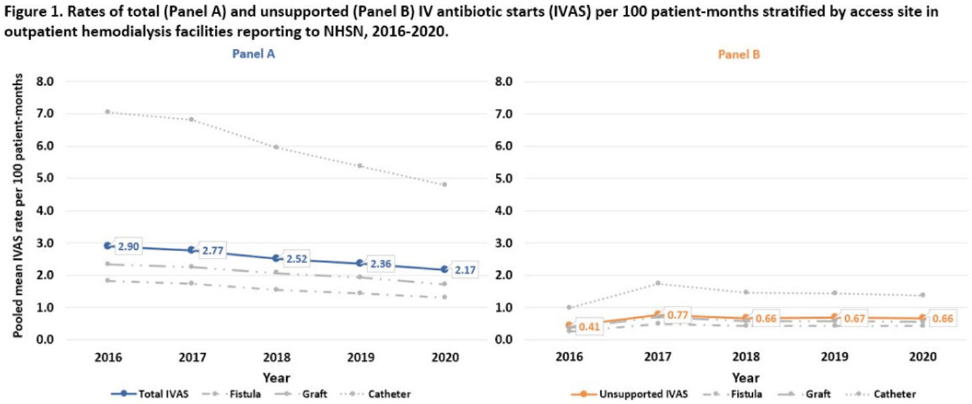
Background: Nearly one-third of patients on hemodialysis receive intravenous (IV) antibiotics annually, but national data characterizing antibiotic use in this population are limited. Using NHSN surveillance data for outpatient dialysis facilities, we estimated temporal changes in the rate of IV antibiotic starts (IVAS) among hemodialysis patients as well as the proportion of IVAS that were not supported by a reported clinical indication. Methods: IVAS events were obtained from the NHSN Dialysis Event module between 2016 and 2020, excluding patients who were out of network, receiving peritoneal or home dialysis, or with unspecified vascular access. IVAS unsupported by documentation were defined as new IVAS without a collected or positive blood culture, pus, redness or swelling event, or an associated clinical symptom. Pooled mean rates of total and unsupported IVAS were estimated per 100 patient months yearly and stratified by vascular access type. Differences in IVAS rates by year were estimated with negative binomial regression. Results: Between 2016 and 2020, 7,278 facilities reported 648,410 IVAS events; 161,317 (25%) were unsupported by documentation (Table 1). In 2016, 3,340 (54%) facilities with ≥1 IVAS event reported an IVAS unsupported by documentation, which increased to 4,994 (73%) in 2020. Total IVAS rates decreased by an average of 8.2% annually (95% CI, 7.1%–9.3%; P < .001). The average annual percentage decrease did not differ significantly by vascular access site. The total IVAS rate was lowest in 2020 (2.17 per 100 patient months; 95% CI, 2.18–2.17). IVAS rates in 2020 were greatest for patients with catheter access (4.79 per 100 patient months; 95% CI, 4.75–4.83), followed by graft (1.71 per 100 patient months; 95% CI, 1.68–1.73), and lowest for patients with fistulas (1.30 per 100 patient months; 95% CI, 1.29–1.31). The overall pooled mean rate of unsupported IVAS was 0.64 per 100 patient months (95% CI, 0.63–0.64), which did not significantly change by year (Fig. 1). Conclusions: Total IVAS rates among outpatient hemodialysis patients have decreased since 2016, and rates among catheter patients remain highest compared to patients with fistulas or grafts. However, unsupported IVAS rates did not change, and the proportion of facilities reporting an unsupported IVAS increased annually. Targeted efforts to engage facilities with unsupported IVAS may help improve accurate reporting and prescribing practices.
Funding: None
Disclosures: None