Refine search
Actions for selected content:
48214 results in Zoology
Development of novel low- and high-emulsifier diets for trial in Crohn's disease management
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E131
-
- Article
-
- You have access
- HTML
- Export citation
Evaluating front-of-pack environmental sustainability messaging for meat and meat alternative products
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E115
-
- Article
-
- You have access
- HTML
- Export citation
Thinking globally, acting locally: Supporting systems change within communities to enhance food security action
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E47
-
- Article
-
- You have access
- HTML
- Export citation
The association between dairy foods and the risk of cardiovascular diseases: a concern in middle age?
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E49
-
- Article
-
- You have access
- HTML
- Export citation
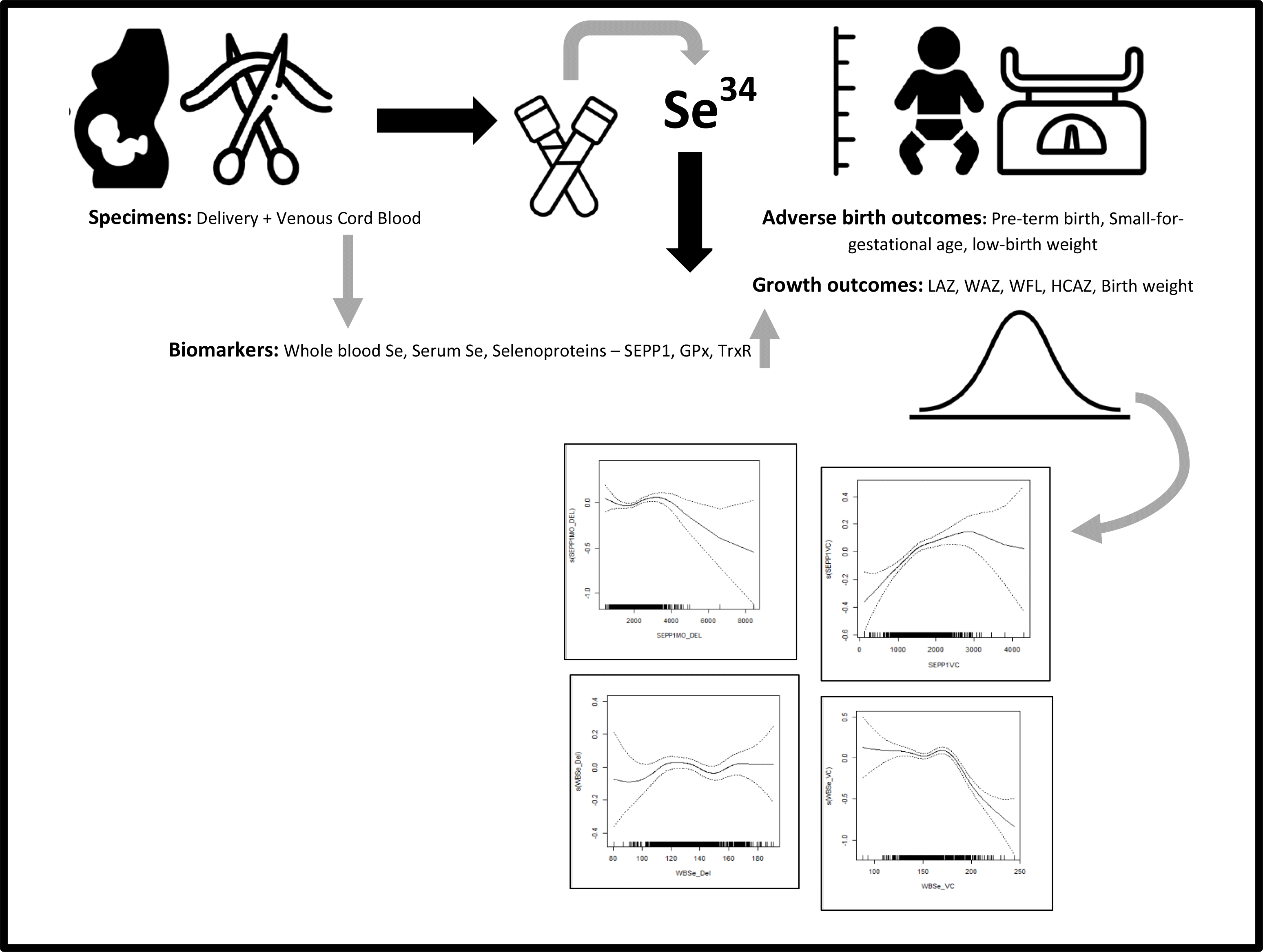
Associations between maternal and infant selenium status and child growth in a birth cohort from Dhaka, Bangladesh
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 9 / 14 November 2023
- Published online by Cambridge University Press:
- 22 March 2023, pp. 1558-1572
- Print publication:
- 14 November 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Effects of DNA-based recommendations on health-related behaviour changes
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E200
-
- Article
-
- You have access
- HTML
- Export citation
Comparison of food group intakes at eating occasion by diet quality: findings from a nationally representative study of Australian adults
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E150
-
- Article
-
- You have access
- HTML
- Export citation
Enabling students to ‘taste their soup before serving it to guests’: Inclusion of formative assessments within a re-designed dietary assessment assignment
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E144
-
- Article
-
- You have access
- HTML
- Export citation
A snapshot of school children's lunchboxes in South Australia through a food and sustainability lens
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E164
-
- Article
-
- You have access
- HTML
- Export citation
FTO: a critical role in obesity and obesity-related diseases
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 10 / 28 November 2023
- Published online by Cambridge University Press:
- 22 March 2023, pp. 1657-1664
- Print publication:
- 28 November 2023
-
- Article
-
- You have access
- HTML
- Export citation
Anthocyanin intake is associated with improved memory in older adults with Mild Cognitive Impairment
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E70
-
- Article
-
- You have access
- HTML
- Export citation
Flavonoid provision to 2–3-year-old children in 30 long day care centres across metropolitan Perth, Western Australia
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E146
-
- Article
-
- You have access
- HTML
- Export citation
Consumer perceptions of nutrient content claims in the Australian food supply: a qualitative study
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E92
-
- Article
-
- You have access
- HTML
- Export citation
Nutritional care approaches and outcomes of health care professionals managing alcohol withdrawal patients post hospital discharge: a scoping review
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E143
-
- Article
-
- You have access
- HTML
- Export citation
Excess visceral adipose tissue is associated with poorer lung function and increased airway inflammation in adults with asthma
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E192
-
- Article
-
- You have access
- HTML
- Export citation
Exploring the physiological barriers to weight management in women with polycystic ovary syndrome: a scoping review
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E130
-
- Article
-
- You have access
- HTML
- Export citation
Identification of starchy flavour attributes and characterization of distinctive sensory profiles of corn, potato, rice and waxy rice starches
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E178
-
- Article
-
- You have access
- HTML
- Export citation
The environmental sustainability of food provision in Australian childcare
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E89
-
- Article
-
- You have access
- HTML
- Export citation
COVID-19 lockdown: friend or foe? A systematic literature review of its impacts on eating patterns, physical activity, body weight and food security
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E127
-
- Article
-
- You have access
- HTML
- Export citation
Shifting adolescents’ interest and motivation in health and healthy eating to promote a healthy and sustainable lifestyle
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue OCE2 / 2023
- Published online by Cambridge University Press:
- 22 March 2023, E103
-
- Article
-
- You have access
- HTML
- Export citation
