Refine search
Actions for selected content:
48204 results in Zoology
Causal associations of tea consumption on risk of pancreatic adenocarcinoma and the mediating role of vascular endothelial growth factor D levels – CORRIGENDUM
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 12 / 28 December 2024
- Published online by Cambridge University Press:
- 16 December 2024, p. 1698
- Print publication:
- 28 December 2024
-
- Article
-
- You have access
- HTML
- Export citation
Longitudinal trajectories of plasma polyunsaturated fatty acids and associations with psychosis-spectrum outcomes in early adulthood
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue OCE4 / November 2024
- Published online by Cambridge University Press:
- 16 December 2024, E278
-
- Article
-
- You have access
- Export citation
A photovoice study exploring perceptions of healthy eating, nutrition and healthy ageing in older Black African adults in the United Kingdom
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue OCE4 / November 2024
- Published online by Cambridge University Press:
- 16 December 2024, E266
-
- Article
-
- You have access
- Export citation
Community cafés as a response to food insecurity: what is their impact?
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue OCE4 / November 2024
- Published online by Cambridge University Press:
- 16 December 2024, E448
-
- Article
-
- You have access
- Export citation
Body composition, body mass index, waist circumference and perimenopausal symptoms in women living in Ireland
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue OCE4 / November 2024
- Published online by Cambridge University Press:
- 16 December 2024, E366
-
- Article
-
- You have access
- Export citation
Effect of specific nutrients or dietary patterns on mental health outcomes in adults; A systematic review and meta-analyses of nutrition interventions
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue OCE4 / November 2024
- Published online by Cambridge University Press:
- 16 December 2024, E277
-
- Article
-
- You have access
- Export citation
BJN volume 132 issue 11 Cover and Back matter
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 11 / 14 December 2024
- Published online by Cambridge University Press:
- 20 December 2024, pp. b1-b2
- Print publication:
- 14 December 2024
-
- Article
-
- You have access
- Export citation
BJN volume 132 issue 11 Cover and Front matter
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 11 / 14 December 2024
- Published online by Cambridge University Press:
- 20 December 2024, pp. f1-f2
- Print publication:
- 14 December 2024
-
- Article
-
- You have access
- Export citation
Reply to the letter on ‘Meat intake and type 2 diabetes among Japanese workers’
-
- Journal:
- British Journal of Nutrition / Volume 133 / Issue 3 / 14 February 2025
- Published online by Cambridge University Press:
- 13 December 2024, p. 333
- Print publication:
- 14 February 2025
-
- Article
-
- You have access
- HTML
- Export citation
Digging deep for nutrients and metabolites derived from high dietary protein intake and their potential functions in metabolic health
-
- Journal:
- Nutrition Research Reviews / Volume 38 / Issue 2 / December 2025
- Published online by Cambridge University Press:
- 13 December 2024, pp. 586-598
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Nutrient digestion efficiency: a comparison between broiler chickens and growing pigs fed maize, barley and oats-based diets with an emphasis on starch
-
- Journal:
- British Journal of Nutrition / Volume 133 / Issue 2 / 28 January 2025
- Published online by Cambridge University Press:
- 13 December 2024, pp. 182-193
- Print publication:
- 28 January 2025
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
An investigation of diet quality across racial groups in the United Kingdom and United States considering nutritional adequacy, disease risk, and environmental sustainability: a secondary analysis of NDNS and NHANES datasets
-
- Journal:
- Journal of Nutritional Science / Volume 13 / 2024
- Published online by Cambridge University Press:
- 13 December 2024, e93
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Turkish version of the renal inpatient nutrition screening tool: validity and reliability for haemodialysis patients
-
- Journal:
- British Journal of Nutrition / Volume 133 / Issue 2 / 28 January 2025
- Published online by Cambridge University Press:
- 13 December 2024, pp. 231-238
- Print publication:
- 28 January 2025
-
- Article
-
- You have access
- Open access
- HTML
- Export citation

Tryptophan regulates food intake in growing pigs by modulating hypothalamic AMPK–mTOR signalling pathway
-
- Journal:
- British Journal of Nutrition / Volume 133 / Issue 2 / 28 January 2025
- Published online by Cambridge University Press:
- 13 December 2024, pp. 269-276
- Print publication:
- 28 January 2025
-
- Article
-
- You have access
- HTML
- Export citation
Effect of egg consumption on early childhood development: evidence from Un Oeuf study
-
- Journal:
- Public Health Nutrition / Volume 28 / Issue 1 / 2025
- Published online by Cambridge University Press:
- 12 December 2024, e10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
Objective:
Recent studies have shown that inclusion of eggs in young children’s diet can help meet nutritional requirements associated with cognitive development. This study aims to investigate the effect of egg consumption on early childhood development using Ages and Stages Questionnaire-3 in Burkina Faso.
Design:The study presented here uses data collected during a follow-up of the Un Oeuf-a three-arm clustered randomised controlled trial (RCT), conducted roughly 4 months after the end of the RCT.
Setting:This research was conducted in eighteen rural villages within the Kaya Department of the Sanmatenga Province in Burkina Faso.
Participants:Participants of this study include a total of 244 children aged between 18 and 33 months, with seventy-eight children in the full intervention group, eighty-three in the partial group, and eighty-three in the control group.
Results:Results show that children with consistent egg consumption (in all months) had a lower odd of falling below the cut-off scores in gross motor (
 ${\rm{OR}} = {\rm 0\!\cdot\!13},{\it P} = \rm{0\!\cdot\!02}$) and personal social skills (
${\rm{OR}} = {\rm 0\!\cdot\!13},{\it P} = \rm{0\!\cdot\!02}$) and personal social skills ( ${\rm{OR}} = 0\!\cdot\!34,{\it P} =0 \!\cdot\!05$). And a dose–response was established; for each additional egg/week, a 1·9 % increase in scores for problem-solving skills was observed.Conclusions:
${\rm{OR}} = 0\!\cdot\!34,{\it P} =0 \!\cdot\!05$). And a dose–response was established; for each additional egg/week, a 1·9 % increase in scores for problem-solving skills was observed.Conclusions:Findings from this study contribute to a growing body of evidence that increasing egg consumption among children in low- and middle-income countries (LMIC) can improve growth and development. The study highlights the need for additional research in LMIC to better understand the multifactorial relationship between diet and childhood development.


Characterising the extent and nature of digital food and beverage marketing in Singapore: a descriptive study
-
- Journal:
- Public Health Nutrition / Volume 28 / Issue 1 / 2025
- Published online by Cambridge University Press:
- 12 December 2024, e14
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Testing a proposed mathematical model of weight loss in women enrolled on a commercial weight-loss programme: the LighterLife study
-
- Journal:
- Journal of Nutritional Science / Volume 13 / 2024
- Published online by Cambridge University Press:
- 12 December 2024, e92
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
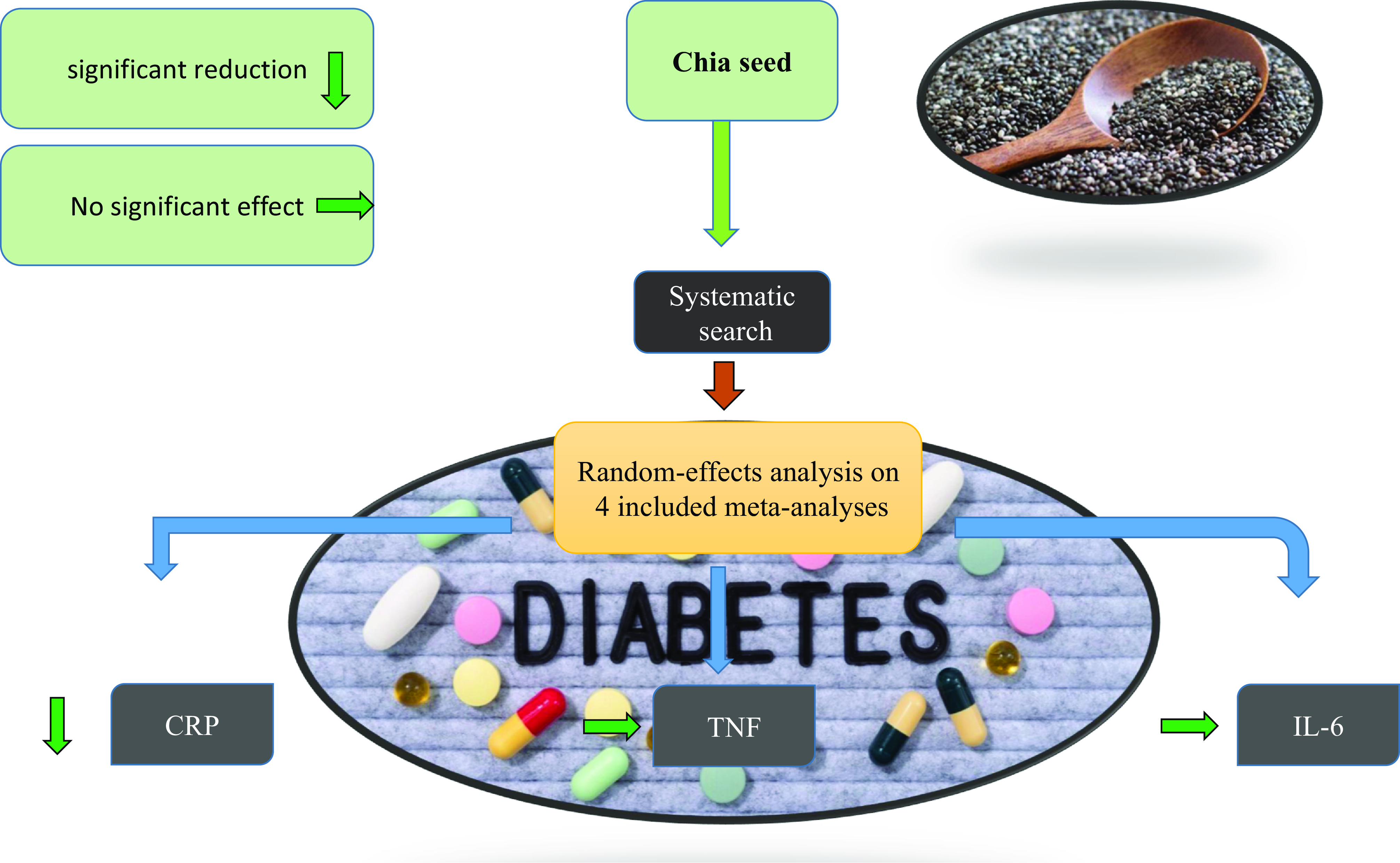
Chia seed supplementation and inflammatory biomarkers: a systematic review and meta-analysis
-
- Journal:
- Journal of Nutritional Science / Volume 13 / 2024
- Published online by Cambridge University Press:
- 11 December 2024, e91
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
High-dose cholecalciferol supplementation to obese infertile men is sufficient to reach adequate vitamin D status – ERRATUM
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 11 / 14 December 2024
- Published online by Cambridge University Press:
- 10 December 2024, pp. 1553-1554
- Print publication:
- 14 December 2024
-
- Article
-
- You have access
- HTML
- Export citation
Methodological and reporting recommendations for clinical trials in Nutritional Psychiatry: Guidelines from the International Society for Nutritional Psychiatry Research
-
- Journal:
- British Journal of Nutrition / Volume 135 / Issue 6 / 28 March 2026
- Published online by Cambridge University Press:
- 10 December 2024, pp. 608-620
- Print publication:
- 28 March 2026
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
