Refine search
Actions for selected content:
106117 results in Materials Science
30 - Tooth development and regeneration
- from Part V - Animal models and clinical applications
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 555-569
-
- Chapter
- Export citation
29 - Models of composite bone and soft-tissue limb trauma
- from Part V - Animal models and clinical applications
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 534-554
-
- Chapter
- Export citation

Synthesis and design of PSf/TiO2 composite membranes for reduction of chromium (VI): Stability and reuse of the product and the process
-
- Journal:
- Journal of Materials Research / Volume 29 / Issue 14 / 28 July 2014
- Published online by Cambridge University Press:
- 24 July 2014, pp. 1537-1545
- Print publication:
- 28 July 2014
-
- Article
- Export citation
Part IV - Biological factor delivery
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 375-376
-
- Chapter
- Export citation
36 - Cardiac tissue regeneration in bioreactors
- from Part V - Animal models and clinical applications
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 640-668
-
- Chapter
- Export citation
33 - Hair follicle and skin regeneration
- from Part V - Animal models and clinical applications
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 590-602
-
- Chapter
- Export citation
34 - In-vitro blood vessel regeneration
- from Part V - Animal models and clinical applications
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 603-620
-
- Chapter
- Export citation

Tunability and enhancement of mechanical behavior with additively manufactured bio-inspired hierarchical suture interfaces
-
- Journal:
- Journal of Materials Research / Volume 29 / Issue 17 / 14 September 2014
- Published online by Cambridge University Press:
- 24 July 2014, pp. 1867-1875
- Print publication:
- 14 September 2014
-
- Article
- Export citation
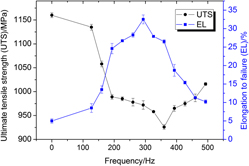
RETRACTED-Effect of electropulsing treatment on the microstructure, texture, and mechanical properties of cold-rolled Ti–6Al–4V alloy
-
- Journal:
- Journal of Materials Research / Volume 29 / Issue 14 / 28 July 2014
- Published online by Cambridge University Press:
- 24 July 2014, pp. 1500-1512
- Print publication:
- 28 July 2014
-
- Article
- Export citation
7 - Nanofibrous polymer scaffolds with designed pore structure for regeneration
- from Part II - Porous scaffolds for regenerative medicine
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 91-103
-
- Chapter
- Export citation
12 - Polymer/ceramic composite scaffolds for tissue regeneration
- from Part II - Porous scaffolds for regenerative medicine
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 203-214
-
- Chapter
- Export citation
Part V - Animal models and clinical applications
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 447-448
-
- Chapter
- Export citation
18 - Microfabricated gels for tissue engineering
- from Part III - Hydrogel scaffolds for regenerative medicine
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 317-331
-
- Chapter
- Export citation
Part II - Porous scaffolds for regenerative medicine
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 89-90
-
- Chapter
- Export citation
19 - Organ printing
- from Part III - Hydrogel scaffolds for regenerative medicine
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 332-374
-
- Chapter
- Export citation
16 - Fumarate-based hydrogels in regenerative medicine applications
- from Part III - Hydrogel scaffolds for regenerative medicine
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 279-294
-
- Chapter
- Export citation
9 - Biological scaffolds for regenerative medicine
- from Part II - Porous scaffolds for regenerative medicine
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 133-150
-
- Chapter
- Export citation
Index
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 680-703
-
- Chapter
- Export citation
27 - Advancing articular cartilage repair through tissue engineering: from materials and cells to clinical translation
- from Part V - Animal models and clinical applications
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 488-513
-
- Chapter
- Export citation
4 - Hematopoietic stem cells and their niches
- from Part I - Introduction to stem cells and regenerative medicine
-
-
- Book:
- Biomaterials and Regenerative Medicine
- Published online:
- 05 February 2015
- Print publication:
- 24 July 2014, pp 44-63
-
- Chapter
- Export citation
