Introduction
The Appearance Anxiety Inventory (AAI; Veale et al., Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2013) is a 10-item measure used to assess cognitive processes and behaviours characteristic of body dysmorphic disorder (BDD). The The AAI is derived from the cognitive behavioural model of BDD (Veale, Reference Veale2004) and measures appearance anxiety as it relates to this model. In this context, appearance anxiety refers to the responses to perceived flaws and shame about one’s appearance (e.g., the way attention is self-focussed, the comparing, ruminating, checking and avoidance behaviour) (Roberts et al., Reference Roberts, Zimmer-Gembeck, Lavell, Miyamoto, Gregertsen and Farrell2018; Veale et al., Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2013). The AAI has recently become more widely used in clinical research and is sensitive to change as an outcome measure in adults (Veale et al., Reference Veale, Anson, Miles, Pieta, Costa and Ellison2014) and adolescents (Gumpert et al., Reference Gumpert, Rautio, Monzani, Jassi, Krebs and Fernández de la Cruz2024; Mataix-Cols et al., Reference Mataix-Cols, Fernández de la Cruz, Isomura, Anson, Turner and Monzani2015), and in research (Flygare et al., 2020).
Development
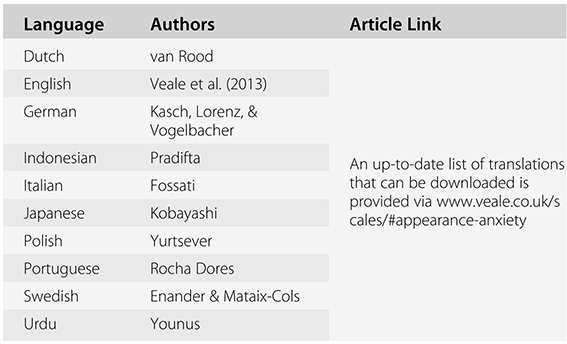
The AAI was developed in response to the lack of measures available to track the cognitive processes and behaviours that might mediate the outcome of treatment in people with BDD (Veale et al., Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2013). Items for the AAI were drawn from a cognitive-behavioural model of the maintenance of BDD (Veale, Reference Veale2004) and the literature on trans-diagnostic processes that occur in mental disorders (Harvey et al., Reference Harvey, Shafran, Watkins and Mansell2004). This model is linked to the experience of the self as an aesthetic object and highlights the responses to a distorted self-image and associated shame. In this vein, the AAI seeks to assist clinicians and clients to establish which processes to focus on during therapy in adults (Veale et al., Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2013). Since its development, the AAI has been translated into nine languages (i.e., Dutch, German, Indonesian, Italian, Japanese, Polish, Portuguese, Swedish, Urdu).
Administration and Timing
The AAI can be administered online or in person to adolescents and adults. The AAI takes approximately two to three minutes to complete.
Factor Structure and Invariance
Exploratory factor analysis of the AAI in a clinical sample identified two factors: avoidance and threat monitoring (Veale et al., Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2013). Six items loaded onto avoidance and four items on threat monitoring. Despite finding two factors, the 10 items were considered as a single factor and accounted for 60.3% of the variance in the items (Veale et al., Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2013). Gumpert et al. (Reference Gumpert, Rautio, Monzani, Jassi, Krebs and Fernández de la Cruz2024) however identified three factors in a sample of adolescents with BDD, namely ‘threat monitoring’, ‘camouflaging’ and ‘avoidance’, explaining 48.15% of the variance. However, a study of a non-clinical sample of adolescents and university students indicated that nine AAI items loaded highly on a single factor with the tenth item relating to checking behaviours being excluded due to its loading highly on a second factor (Roberts et al., Reference Roberts, Zimmer-Gembeck, Lavell, Miyamoto, Gregertsen and Farrell2018). Roberts et al. (Reference Roberts, Zimmer-Gembeck, Lavell, Miyamoto, Gregertsen and Farrell2018) also found that the age invariance of the AAI loadings was supported.
Evidence of Reliability
The original AAI was found to have good internal consistency in a clinical (α = .86) and community sample (α = .91, Veale et al., Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2013), and had good test–retest reliability after 1 week with an intra-class correlation of .87 (p < .001) (Veale et al., Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2013). The Polish translation of the AAI demonstrated an identical Cronbach’s alpha coefficient to the original AAI validation (Yurtsever et al., Reference Yurtsever, Matusiak, Szepietowska, Veale and Szepietowski2021). It has also demonstrated good internal consistency in adolescents with BDD (McDonald’s omega = .83) (Gumpert et al., Reference Gumpert, Rautio, Monzani, Jassi, Krebs and Fernández de la Cruz2024).
Evidence of Validity
The AAI has accrued much convergent validity support. The AAI has been significantly correlated with several other measures, including the BDD-YBOCS (Yale Brown Obsessive Compulsive Scale Modified for Body Dysmorphic Disorder). Veale et al. (Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2013) also demonstrated that the AAI was highly correlated with measures of social anxiety and appearance-based rejection, as well as showing a moderate negative correlation with the quality of life affected by body image (BIQLI; Body Image Quality of Life Inventory). These findings suggest that higher scores on the AAI are associated with more negative beliefs about appearance, resulting in a greater negative impact of body image on a person’s quality of life. There is also convergent validity data in adolescents (Mastro et al., Reference Mastro, Zimmer-Gembeck, Webb, Farrell and Waters2016; Roberts et al., Reference Roberts, Zimmer-Gembeck, Lavell, Miyamoto, Gregertsen and Farrell2018) and on the BDD-YBOCS for adolescents with BDD (Gumpert et al., Reference Gumpert, Rautio, Monzani, Jassi, Krebs and Fernández de la Cruz2024). The AAI is sensitive to change during cognitive behaviour therapy in adults (Veale et al., Reference Veale, Anson, Miles, Pieta, Costa and Ellison2014) and adolescents (Gumpert et al., Reference Gumpert, Rautio, Monzani, Jassi, Krebs and Fernández de la Cruz2024; Mataix-Cols et al., Reference Mataix-Cols, Fernández de la Cruz, Isomura, Anson, Turner and Monzani2015). The Polish validation of the AAI also demonstrated convergent validity of the AAI and Cosmetic Procedure Screening Questionnaire for the severity of BDD symptoms (Yurtsever et al., Reference Yurtsever, Matusiak, Szepietowska, Veale and Szepietowski2021).
Scale Instructions and Items
Instructions: ‘Please tick the box that best describes the way you have felt about the appearance of a specific feature over the past week, including today.’
1. I compare aspects of my appearance to others.
2. I check my appearance (e.g., in mirrors, by touching with my fingers, or by taking photos of myself).
3. I avoid situations or people because of my appearance.
4. I brood about past events or reasons to explain why I look the way I do.
5. I think about how to camouflage or alter my appearance.
6. I am focussed on how I feel I look, rather than on my surroundings.
7. I avoid reflective surfaces, photos, or videos of myself.
8. I discuss my appearance with others or question them about it.
9. I try to camouflage or alter aspects of my appearance.
10. I try to prevent people from seeing aspects of my appearance within situations (e.g., by changing my posture, avoiding bright lights).
Scoring
The AAI total score is obtained by summing all the items. The maximum score is 40, and higher scores reflect greater frequency of a process. A reliable change score is 7 or above. Caseness for BDD is a score of 19 or above. No items are reverse scored (Veale et al., Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2013).
Cost
There is no cost associated with the use of the AAI. The measure is free to use in any setting.
Translations (Table 3.1)

Permissions
Scholars (e.g., researchers, faculty, students) and clinicians have permission to use the AAI if they do not modify any item or change the nature of the scale (e.g., shorten it). If scholars wish to modify the individual scale items or the items composing the scale, they should seek permission from David Veale (david.veale@kcl.ac.uk) and provide a rationale. Scholars who wish to translate the AAI into another language should also contact David Veale for permission and facilitate back translations. Scholars are encouraged to follow best practices for scale translation and validation (see Swami & Barron, 2019; Swami, Todd, & Barron, 2021).
Copyright
Copyright for the AAI is owned by David Veale et al. (Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2013).