Refine listing
Actions for selected content:
1416829 results in Open Access
Visualization of Pain and Agitation by System Analysis Algorithms
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 38-39
-
- Article
-
- You have access
- Export citation
P107: Paranoid Ideation Without Psychosis Is Associated With Depression, Anxiety, and Suicide Attempts in General Population
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 169
-
- Article
-
- You have access
- Export citation
FC3: “Empowering Health & Social Service Providers in Addressing Social Isolation & Loneliness in Older Adults”
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 66
-
- Article
-
- You have access
- Export citation
P19: Effects of a Post-diagnostic Support Programme on self-efficacy among persons with dementia and family members
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 194-195
-
- Article
-
- You have access
- Export citation
P195: The evolution of a community mental health team in Singapore: Community Psychogeriatric Programme
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 228
-
- Article
-
- You have access
- Export citation
P72: Diagnostic pathways for people living with rare types of dementia
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 245
-
- Article
-
- You have access
- Export citation
P100: Education level is associated with neuropsychiatric symptoms in patients with amnestic-mild cognitive impairment
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 211
-
- Article
-
- You have access
- Export citation
P94: Co-design of a theory-based implementation plan for a digital holistic assessment and decision support framework for people with dementia in care homes
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 167
-
- Article
-
- You have access
- Export citation
P59: Associations Between Smoking, Alcohol Consumption, Physical Activity and Depression in Middle-Aged Premenopausal and Postmenopausal Women
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 156-157
-
- Article
-
- You have access
- Export citation
Evaluation of the Situations of Coping With Mental Trauma and Trauma in Emergency Service Personnel Who Medically Intervened to Earthquake Affected People in the 2020 Izmir Earthquake
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 18 / 2024
- Published online by Cambridge University Press:
- 02 February 2024, e17
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
FC10: Telehealth for Older Adults: Developing telehealth competencies to ensure access, quality and equity across the lifespan
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 72-73
-
- Article
-
- You have access
- Export citation
Transnational Echoes of Spenceanism: A Text-Mining Exploration in English-Language Newspapers (1790–1850)
-
- Journal:
- International Review of Social History / Volume 69 / Issue 1 / April 2024
- Published online by Cambridge University Press:
- 02 February 2024, pp. 67-97
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
P118: The Geriatric Psychiatry Fellowship Program in Mexico
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 172
-
- Article
-
- You have access
- Export citation
FC39: The influence of social constructivism on children and young adults perspectives of parental young onset dementia: A thematic analysis of the narratives
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 101-102
-
- Article
-
- You have access
- Export citation
P160: Electroconvulsive therapy for neuropsychiatric symptoms in dementia: survey among Dutch physicians
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 257-258
-
- Article
-
- You have access
- Export citation
FC22: Changes in inhibitory control in older adults: Diminished inhibitory efficiency or slowing of general processing speed?
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 83-84
-
- Article
-
- You have access
- Export citation
FC26: What have staff got to do with it? Untangling complex relationships between residential aged care staff, the quality of care they provide, and the quality of life of people with dementia
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 87-88
-
- Article
-
- You have access
- Export citation
-
Background:
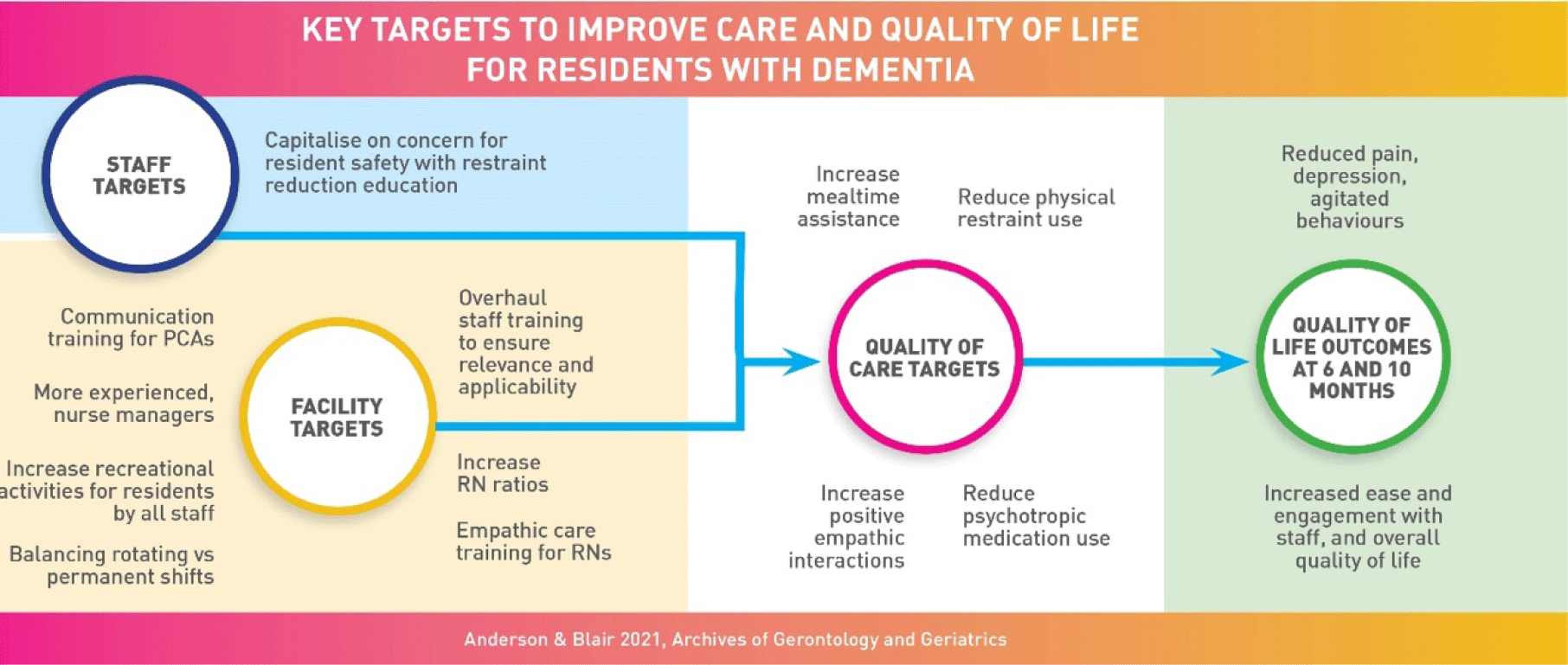
Despite the integral role long term residential care staff play in the lives of residents with dementia, the mechanisms for supporting staff to bring about good quality of care (QOC) and quality of life (QOL) are poorly understood. This study focused on establishing the key mechanisms to improve QOC and in turn QOL of residents with dementia.
Method:Over a 10-month period we followed: 247 older adults with dementia from 12 not-for-profit residential care facilities, their families/care partners (n=225), managers (n=12) and staff (n=232). Facilities ranged in size from 10 to 137 beds, located across remote, rural and metropolitan areas of south eastern Australia. Measures included: staff surveys, family member and resident interviews, resident file audits, live resident and staff observations and organisational audits. Multilevel Modelling or Generalised Estimating Equations analyses were conducted for each of the 12 QOC variables, with 22 staff and control variables as the predictors, and for each of the 11 QOL variables, with 20 QOC and control variables as predictors.
Results:Analyses established significant associations between a large number of staff and QOC variables and between QOC and QOL variables.
Conclusions:The quality of the care provided to residents has strong, widespread influences on the QOL of residents. The most promising areas for intervening with staff were: increasing the relevance and applicability of staff training and qualifications, upskilling staff in empathic care provision, communication, and restraint reduction, using a mixture of permanent and rotating shifts, prioritising recreational activity provision by all staff and increasing assistance with meals. patients with cognitive impairment in rural hospitals.

Plenary Session 1 : Healthy Ageing and the role of physical and social environments
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 13
-
- Article
-
- You have access
- Export citation
FC30: The relationships between neuroticism, social connection and cognition
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 92-94
-
- Article
-
- You have access
- Export citation
-
Background:
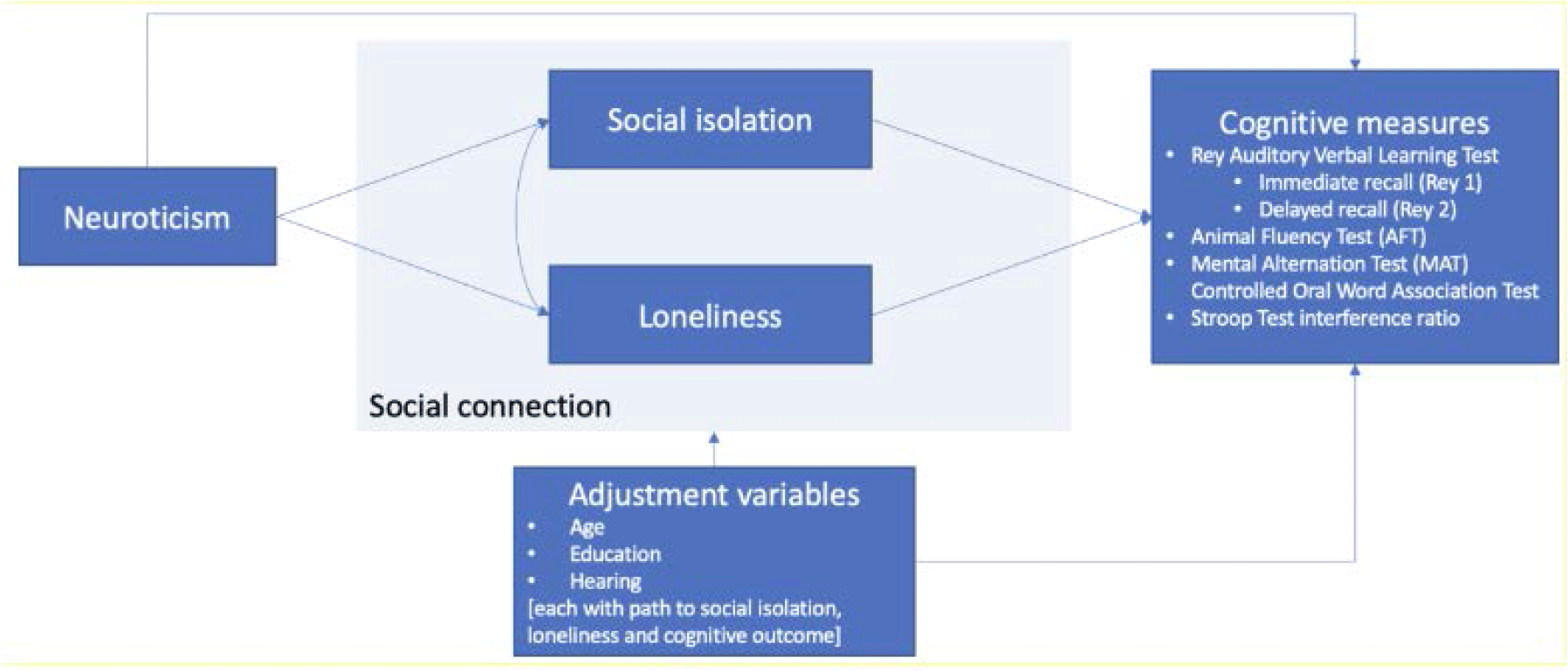
Social connection is associated with better health, including reduced risk of dementia. Personality traits are also linked to cognitive outcomes; neuroticism is associated with increased risk of dementia. Personality traits and social connection are also associated with each other. Taken together, evidence suggests the potential impacts of neuroticism and social connection on cognitive outcomes may be linked. However, very few studies have simultaneously examined the relationships between personality, social connection and health.
Research objective:We tested the association between neuroticism and cognitive measures while exploring the potential mediating roles of aspects of social connection (loneliness and social isolation).
Method:We conducted a cross-sectional study with a secondary analysis of the Canadian Longitudinal Study on Aging (CLSA) Comprehensive Cohort, a sample of Canadians aged 45 to 85 years at baseline. We used only self-reported data collected at the first follow-up, between 2015 and 2018 (n= 27,765). We used structural equation modelling to assess the association between neuroticism (exposure) and six cognitive measures (Rey Auditory Verbal Learning Test immediate recall and delayed recall, Animal Fluency Test, Mental Alternation Test, Controlled Oral Word Association Test and Stroop Test interference ratio), with direct and indirect effects (through social isolation and loneliness). We included age, education and hearing in the models and stratified all analyses by sex, females (n= 14,133) and males (n=13,632).
 Preliminary results of the ongoing study:
Preliminary results of the ongoing study:We found positive, statistically significant associations between neuroticism and social isolation (p<0.05) and loneliness (p<0.05), for both males and females. We also found inverse, statistically significant associations between neuroticism and all cognitive measures (p<0.05), except the Stroop Test interference ratio. In these models, there was consistent evidence of indirect effects (through social isolation and loneliness) and, in some cases, evidence of direct effects. We found sex differences in the model results.
Conclusion:Our findings suggest that the association between neuroticism and cognitive outcomes may be mediated by aspects of social connection and differ by sex. Understanding if and how modifiable risk factors mediate the association between personality and cognitive outcomes would help develop and target intervention strategies that improve social connection and brain health.

iSupport: the online support program for caregivers of people with dementia
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 32
-
- Article
-
- You have access
- Export citation
