Refine listing
Actions for selected content:
1416829 results in Open Access
P169: IMPROVING THE MENTAL HEALTH CARE NEEDS OF OLDER ADULTS IN NEPAL.
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 142
-
- Article
-
- You have access
- Export citation
Cross-sector learning collaboratives can improve post-diagnosis care integration for people with young onset dementia
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 8-9
-
- Article
-
- You have access
- Export citation
P57: The ENGAGED study: dementia prevention co-design for people living with depression
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 116-117
-
- Article
-
- You have access
- Export citation
P170: Safety and Tolerability of Brexpiprazole for the Treatment of Agitation in Alzheimer’s Dementia: Pooled Results From Three Phase III Trials
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 259-260
-
- Article
-
- You have access
- Export citation
FC16: Memory Services National Accreditation Programme (MSNAP), United Kingdom The Royal College of Psychiatrists, UK
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 78-79
-
- Article
-
- You have access
- Export citation
P103: Middle Cerebral Artery Stenosis is Associated with Severity of Depression in Elderly Patients: Magnetic Resonance Angiography (MRA) Findings
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 168-169
-
- Article
-
- You have access
- Export citation
FC23: Dementia and Triadic (Doctor-Patient-Carer) Interactions in Primary Care
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 84-85
-
- Article
-
- You have access
- Export citation
FC18: Can rehabilitation improve functional independence of older people with dementia? A pragmatic randomized controlled trial (RCT) of the Interdisciplinary Home-bAsed Reablement Program (I-HARP)
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 80-81
-
- Article
-
- You have access
- Export citation
Blended web-based Acceptance and Commitment Therapy for Informal Caregivers of people with dementia (ACT-IC study): Result of social health aspects
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 4
-
- Article
-
- You have access
- Export citation
Social connections and risk of incident mild cognitive impairment, dementia, and mortality in 13 longitudinal cohort studies of ageing
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 16-17
-
- Article
-
- You have access
- Export citation
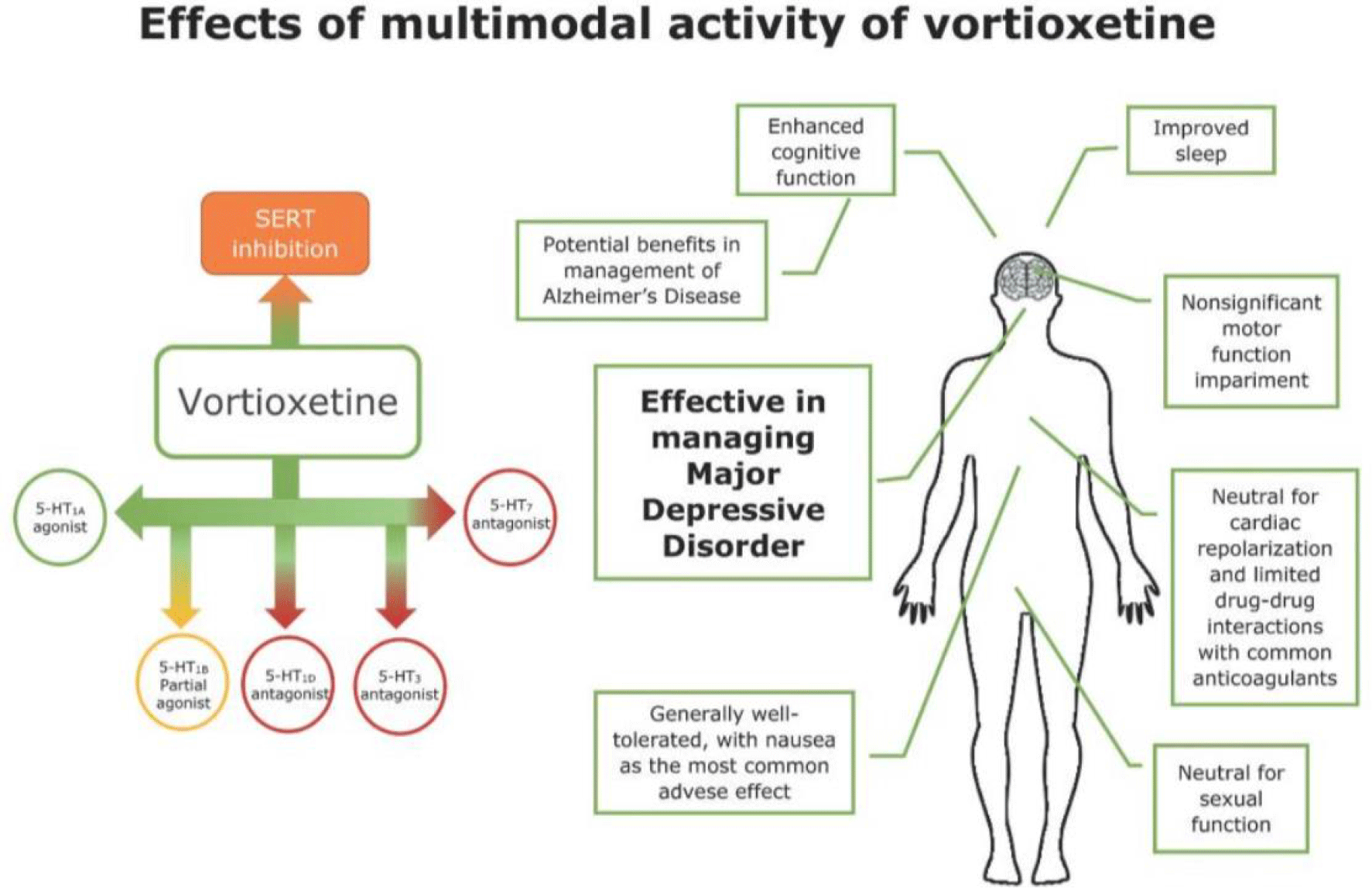
P149: Chronic fatigue syndrome and its response to the use of a multimodal antidepressant
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 216-217
-
- Article
-
- You have access
- Export citation
-
Objective:
We present a case that shows a very favourable response of the antidepressant vortioxetine in the functional and cognitive recovery in a patient with Chronic Fatigue Syndrome and its role as a pain modulator.
Methods:This is an observational study using a clinical case. An 80-year-old female patient admitted to the Postacute care unit for recovering her functional baseline following surgical intervention for a hip fracture. On admission, the main symptom was residual pain at the level of the operated lower limb, as well as allodynia and a tingling sensation, which did not subside with conventional analgesia. During admission she also presented, insomnia, daytime hypersomnolence, bradypsychia, and emotional instability in the form of easy crying. It is worth mentioning that prior to admission the patient presented with multiple nonspecific somatic complaints, such as fatigue, headache, myalgia, and arthralgia, adding over time, great difficulty in planning and performing household tasks. The functional progress of the patient during admission was very slow, mainly due to the combination of lack of engagement, together with episodes of irritability, restlessness and suffering from fear of falling syndrome. Given the suspicion of previously undiagnosed Chronic Fatigue Syndrome, exacerbated by the decline in her functional baseline after surgery, treatment was started with vortioxetine in addition to non-pharmacological measures and psychotherapy, obtaining excellent results in approximately 4 weeks.
Results:Great effectiveness of vortioxetine in the treatment of Chronic Fatigue Syndrome and in the control of concomitant pain (despite that indication is not included in the molecule's data sheet). The patient followed a very favourable evolution achieving, on discharge, an ad integrum recovery of her functional state.
Conclusion:As presented in this case, treatment with multimodal antidepressant treatment (vortioxetine) could have positive impact for patients with Chronic Fatigue Syndrome, achieving improvements in the affective-cognitive aspect and controlling the pain related to this syndrome, avoiding polypharmacy.

Descriptive anatomy and three-dimensional reconstruction of the skull of the tetrapod Eoherpeton watsoni Panchen, 1975 from the Carboniferous of Scotland
-
- Journal:
- Earth and Environmental Science Transactions of The Royal Society of Edinburgh , First View
- Published online by Cambridge University Press:
- 02 February 2024, pp. 1-21
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Virtual reality to provide caregiver skill development and problem solving
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 42-43
-
- Article
-
- You have access
- Export citation
Cost-effectiveness of a tablet-based intervention to support social health in dementia: results from the FindMyApps randomized controlled trial
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 3
-
- Article
-
- You have access
- Export citation
FC37: Prevalence of depressive symptoms and its association with probable sarcopenia, disability, frailty and comorbidities among older adults.
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 100
-
- Article
-
- You have access
- Export citation
P92: Risk Assessment in People living with Dementia: A Systematic Review
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 208
-
- Article
-
- You have access
- Export citation
Collective learning as means to improve quality of long-term care
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 55-56
-
- Article
-
- You have access
- Export citation
P153: The CIMA-Q and CompAS cohort studies on factors associated with Alzheimer's disease (AD): Exploring sociodemographic, health and neuropsychological profile of Subjective Cognitive Decline (SCD) participants from two culturally differentiated samples.
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 269-272
-
- Article
-
- You have access
- Export citation
P13: Supporting physical health for mental health consumers, in a community setting
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 193-194
-
- Article
-
- You have access
- Export citation
Digital technologies in ISupport implementation in Russia
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 59-60
-
- Article
-
- You have access
- Export citation
