Refine listing
Actions for selected content:
1416804 results in Open Access
FC2: The effect of Maintenance phase of Transcranial Direct Current Stimulation (tDCS) in Alzheimer’s Dementia
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 65-66
-
- Article
-
- You have access
- Export citation
P51: Correlation between skin conductance and anxiety in virtual reality
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 154-155
-
- Article
-
- You have access
- Export citation
Chinese caregivers’ experiences in an iSupport intervention program in Australia and China
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 58-59
-
- Article
-
- You have access
- Export citation
FC5: The Maintain Your Brain online multidomain intervention for dementia risk reduction: qualitative exploration of lifestyle changes made, continued, or declined, and why
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 68
-
- Article
-
- You have access
- Export citation
P209: Psychological therapies for depression in older adults residing in long-term care settings: Are they effective?
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 267
-
- Article
-
- You have access
- Export citation
Keynote Lecture: Emerging Concepts in Combating Ageism, Protecting and Promoting Human Rights and Mental Health of Older Persons
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 13
-
- Article
-
- You have access
- Export citation
FC40: Social health and subsequent cognitive capability: examining the potential mediating roles of depression symptoms and inflammatory biomarker
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 102-103
-
- Article
-
- You have access
- Export citation
P66: A systematic review of measures of social connection for people living in long-term care homes
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 118-119
-
- Article
-
- You have access
- Export citation
FC9: Ethno-racial identity and cognitive impairment: A population-based study
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 71-72
-
- Article
-
- You have access
- Export citation
S18: Newcomers to euthanasia and assisted suicide: challenges for Psychogeriatrics with a focus on Spain and Portugal
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 52-53
-
- Article
-
- You have access
- Export citation
ON THE LIMIT SET OF A COMPLEX HYPERBOLIC TRIANGLE GROUP
- Part of
-
- Journal:
- Bulletin of the Australian Mathematical Society / Volume 110 / Issue 2 / October 2024
- Published online by Cambridge University Press:
- 02 February 2024, pp. 338-345
- Print publication:
- October 2024
-
- Article
- Export citation
-
Let
 $\Gamma =\langle I_{1}, I_{2}, I_{3}\rangle $ be the complex hyperbolic
$\Gamma =\langle I_{1}, I_{2}, I_{3}\rangle $ be the complex hyperbolic  $(4,4,\infty )$ triangle group with
$(4,4,\infty )$ triangle group with  $I_1I_3I_2I_3$ being unipotent. We show that the limit set of
$I_1I_3I_2I_3$ being unipotent. We show that the limit set of  $\Gamma $ is connected and the closure of a countable union of
$\Gamma $ is connected and the closure of a countable union of  $\mathbb {R}$-circles.
$\mathbb {R}$-circles.





RECOLLECTIONS OF MY TIME AT THE HISTORY OF ECONOMICS SOCIETY
-
- Journal:
- Journal of the History of Economic Thought / Volume 46 / Issue 4 / December 2024
- Published online by Cambridge University Press:
- 02 February 2024, pp. 585-589
- Print publication:
- December 2024
-
- Article
- Export citation
FC12: Ageism and mental health stigma: key barriers to accessing mental health services among Peruvian older adults
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 75
-
- Article
-
- You have access
- Export citation
P204: Heart rate variability in patients with dementia or neurocognitive disorders: A systematic review and meta-analysis
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 190
-
- Article
-
- You have access
- Export citation
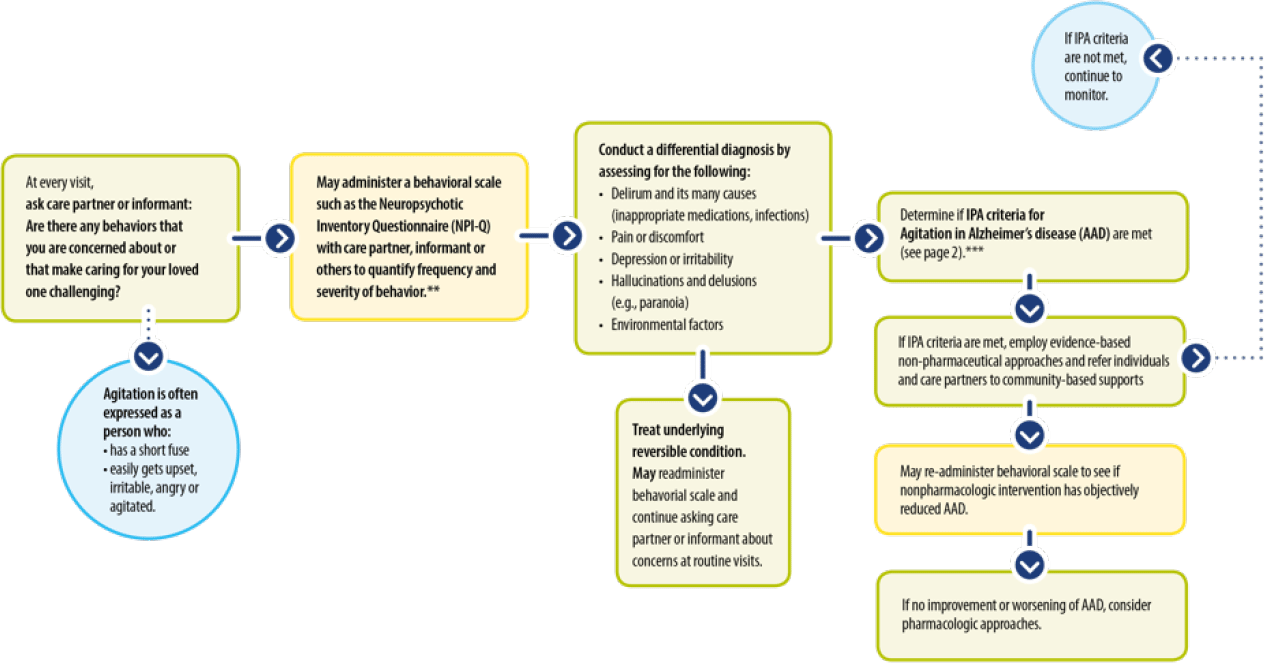
P62: Agitation in Alzheimer’s Disease (AAD): A Decision Tree for Healthcare Providers
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 205-206
-
- Article
-
- You have access
- Export citation
-
Developed by THE GERONTOLOGIC SOCIETY OF AMERICA
Supported by an unrestricted educational grant from Avanir
The prevalence of agitation in Alzheimer’s Disease (AAD) approaches 80%. Patients with AAD have more severe behavioral,depressive, and frontal lobe symptoms and are at increased risk for hospitalization and nursing home placement.
Early agitation is a robust predictor of accelerated progression and mortality and is distressing and dangerous for patients and care partners.
This presentation was recently developed by the Gerontologic Society of America (GSA) which convened an expert AD Working Group to develop a “Decision Tree” for healthcare providers relative to the assessment of AAD and the employment of Non-Pharmacologic and Pharmacologic treatment options

P95: Caregiver Perspectives on the Meaningful Change in Agitation Behaviors Measured by the Cohen-Mansfield Agitation Inventory
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 209
-
- Article
-
- You have access
- Export citation
S5: COGNISANCE: Co-Designing Dementia Diagnosis And Post Diagnostic Care
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 28
-
- Article
-
- You have access
- Export citation
P128: The Valladolid Multicentre Study: Delirium characteristics in patients attended in seven liaison psychiatry services in Spain.
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 133
-
- Article
-
- You have access
- Export citation
Description of Acromoldavicus xerophilus n. sp. (Nematoda, Rhabditida, Elaphonematidae) from the southern Iberian Peninsula, including a key to species of the genus
-
- Journal:
- Journal of Helminthology / Volume 98 / 2024
- Published online by Cambridge University Press:
- 02 February 2024, e14
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Factors associated with older adults’ quality of life
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 22-23
-
- Article
-
- You have access
- Export citation
