Refine listing
Actions for selected content:
1416799 results in Open Access
P106: Palliative care for people with advanced dementia
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 251-252
-
- Article
-
- You have access
- Export citation
P73: Clinical Psychology of Ageing: The Italian Manifesto
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 161-162
-
- Article
-
- You have access
- Export citation
P60: Development of a participant-driven dementia learning program by people living with dementia
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 243-244
-
- Article
-
- You have access
- Export citation
Co-Designing Dementia Diagnosis And Post Diagnostic Care, The Cognisance Project: Forward with Dementia (FWD)
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 28-29
-
- Article
-
- You have access
- Export citation
P10: Feasibility of a Longitudinal Audiovisual Observation Protocol to Characterize EL in Advanced AD/ADRD
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 110
-
- Article
-
- You have access
- Export citation
P91: Symptoms of Anxiety and Depression after stroke – a follow up study in outpatients followed in a rehabilitation recovery unit
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 248-249
-
- Article
-
- You have access
- Export citation
P187: A patient with early-onset Alzheimer’s disease presenting with a unique form of Capgras syndrome
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 143-144
-
- Article
-
- You have access
- Export citation
P137: Cost Considerations of Untreated Agitation: Direct, Indirect, and Intangible
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 215
-
- Article
-
- You have access
- Export citation
P32: Effects of vitamin D3 and marine omega-3 fatty acids supplementation on indicated and selective prevention of depression in older adults: results from the clinical center sub-cohort of the VITamin D and OmegA-3 TriaL
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 152-153
-
- Article
-
- You have access
- Export citation
P70: Development and validation study of the suicide screening questionnaire-observer rating (SSQ-OR)
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 161
-
- Article
-
- You have access
- Export citation

Streamwise dispersion of soluble matter in solvent flowing through a tube
-
- Journal:
- Journal of Fluid Mechanics / Volume 980 / 10 February 2024
- Published online by Cambridge University Press:
- 02 February 2024, A33
-
- Article
- Export citation
QUA volume 117 Cover and Front matter
-
- Journal:
- Quaternary Research / Volume 117 / January 2024
- Published online by Cambridge University Press:
- 02 February 2024, pp. f1-f4
-
- Article
-
- You have access
- Export citation
P202: Post-COVID syndrome presented with psychomotor change and suicidal ideations: a geriatric case report
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 229-230
-
- Article
-
- You have access
- Export citation
P88: Individuals with Mild Cognitive Impairment (MCI) have poorer social networks than cognitively normal individuals from rural India
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 165-166
-
- Article
-
- You have access
- Export citation
S14: The use of advanced data and sensortechnology in dementia: innovation and implementation
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 43-44
-
- Article
-
- You have access
- Export citation
P122: Differences of the treatment needs of patients with dementia with Lewy bodies and their caregivers with duration after diagnosis
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 173-175
-
- Article
-
- You have access
- Export citation
-
Objective:
We have reported parkinsonism and psychiatric symptoms were the most important treatment needs of patients with dementia with Lewy bodies (DLB) and their caregivers, respectively 1). However, the frequency presenting clinical symptoms and the onset time vary among patients. We investigated the impact of the disease duration on clinical symptoms, prescribed medication and treatment needs of patients and their caregivers.
Methods:Disease duration was defined as time after diagnosis with DLB. Patient-caregiver pairs were classified into two groups; one with a disease duration <24 months (S-group) and the other with a disease duration ≥24 months (L-group). Comparisons were made between two groups regarding background characteristics and treatment needs of patients and caregivers. Treatment needs were defined as symptom domains most distressing to patients and caregivers.
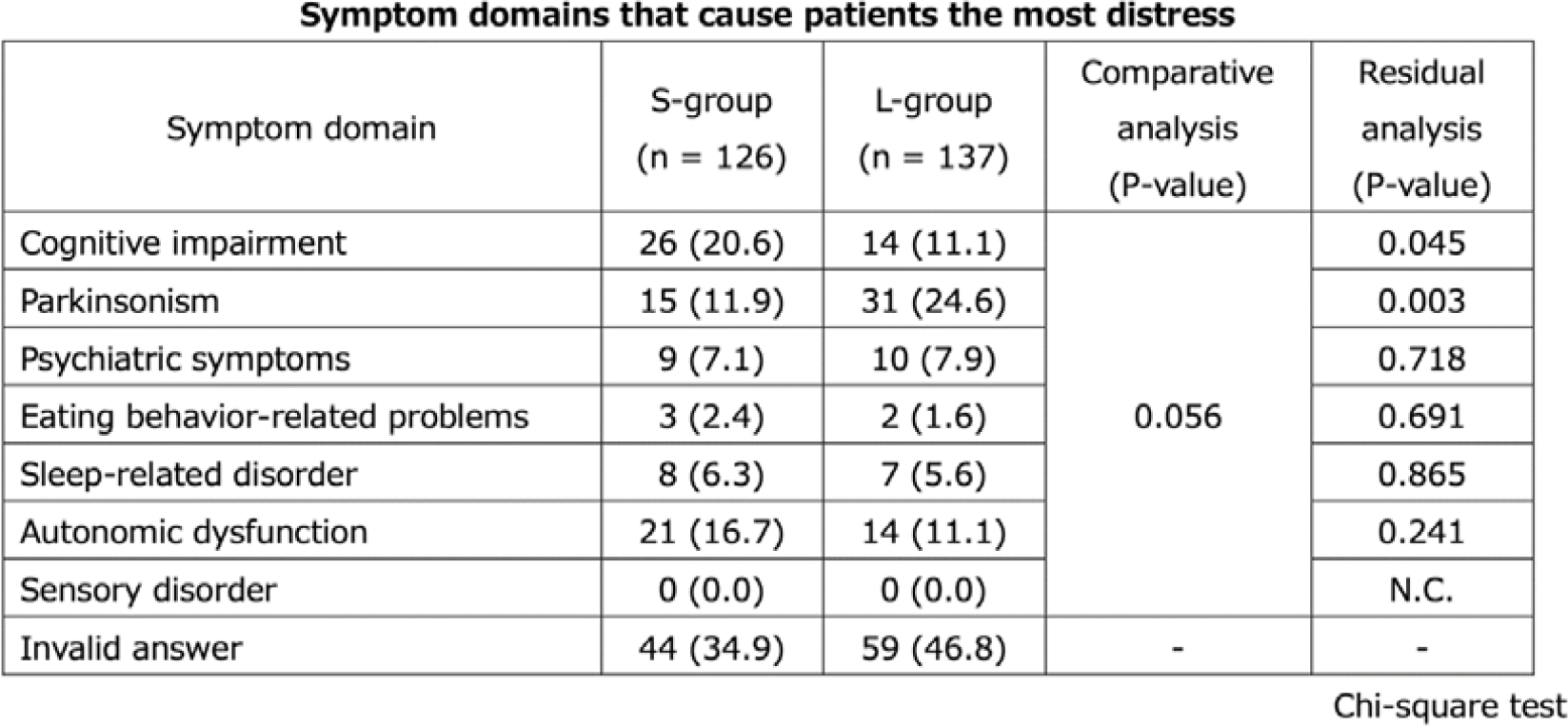
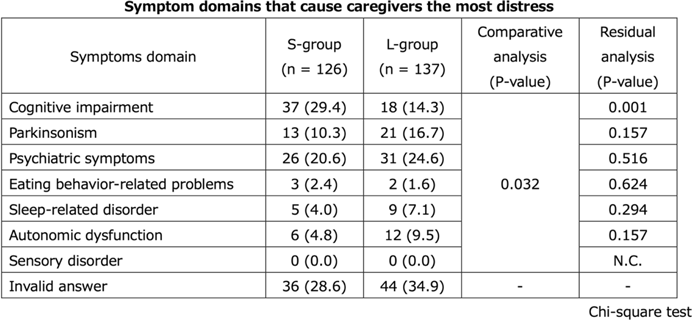
Results:S-group and L-group were consisted of 126 and 137 pairs of patients and their caregivers, respectively. Regarding patientsʼ current symptoms, parkinsonism and autonomic dysfunction were significantly higher in L-group than S-group. MDS-UPDRS Part III total score and the frequency of prescription for memantine and antiparkinsonian were also significantly higher in L-group than in S- group. The treatment needs most frequently selected by patients was cognitive impairment (20.6%) followed by autonomic dysfunction (16.7%) and parkinsonism (11.9%) in S-group, and parkinsonism (24.6%), followed by cognitive impairment and autonomic dysfunction (11.1% each) in L-group, suggesting no significant difference in the tendency of symptom domains to desire treatment between groups (P=0.056). However, residual analysis showed that patients in S-group were more likely to select cognitive impairment than in L-group (P=0.045), and those in L-group were more likely to select parkinsonism than in S-group (P=0.003). The treatment needs most frequently selected by caregivers in S-group was cognitive impairment (29.4%) followed by psychiatric symptoms (20.6%) and parkinsonism (10.3%) in S-group, and psychiatric symptoms (24.6%), followed by parkinsonism (16.7%) and cognitive impairment (14.3%) in L-group, suggesting significant difference in the tendency of patientsʼ symptom domains to desire treatment between groups (P=0.032). Dara from the onset will be added at the poster presentation.
Conclusion:It was suggested that the treatment needs of patients and their caregivers might change with duration after diagnosis.


Research agenda for antibiotic stewardship within the Veterans’ Health Administration, 2024–2028
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 8 / August 2024
- Published online by Cambridge University Press:
- 02 February 2024, pp. 923-929
- Print publication:
- August 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Plenary Session 4: Disease-Modified Drug
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, p. 14
-
- Article
-
- You have access
- Export citation
FC34: Cognitive reserve and depressive burden in older adults: variation according to reserve measurement
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 97-98
-
- Article
-
- You have access
- Export citation
P161: Heterogeneity and Clinical Uncertainty of BPSD Therapeutics
-
- Journal:
- International Psychogeriatrics / Volume 35 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 02 February 2024, pp. 221-222
-
- Article
-
- You have access
- Export citation
