Refine listing
Actions for selected content:
1418337 results in Open Access
91 Agent Orange Exposure and Mild Cognitive Impairment in U.S. Vietnam Era Veterans
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 392-393
-
- Article
-
- You have access
- Export citation
80 Ecological Momentary Assessment of the Fluctuations in Cognitive Performance and Contextual States of Community-Dwelling Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 483-484
-
- Article
-
- You have access
- Export citation
87 Examining the use of the Embedded Performance Validity Test in the Brief Visuospatial Memory Test-Revised Among Spanish-Speaking Patients
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 760-761
-
- Article
-
- You have access
- Export citation
20 The Influence of Brain Injury Severity, Anxiety, and Depression on Objective and Subjective Prospective Memory Problems
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 129-130
-
- Article
-
- You have access
- Export citation
92 Validation of Coin-in-Hand Procedure in a Veteran Population
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 764-765
-
- Article
-
- You have access
- Export citation
11 Contributions of Cardiovascular Burden, Peripheral Inflammation, and Brain Integrity on Digital Clock Drawing Performance in Non-Demented Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 325-326
-
- Article
-
- You have access
- Export citation
29 Vascular Burden Mediates the Relationship Between ADHD and Cognition in Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 637-638
-
- Article
-
- You have access
- Export citation
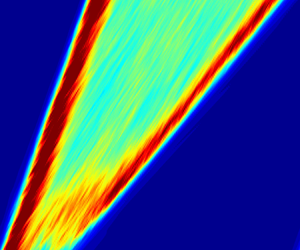
Scaling and mechanism of the propagation speed of the upstream turbulent front in pipe flow
-
- Journal:
- Journal of Fluid Mechanics / Volume 977 / 25 December 2023
- Published online by Cambridge University Press:
- 21 December 2023, R4
-
- Article
- Export citation
45 Gender Differences in Mathematics and its Cognitive and Non-Cognitive Predictors in Community College Students.
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 651-652
-
- Article
-
- You have access
- Export citation
58 Hippocampal Subregions Predict Executive Function Across the Adult Lifespan
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 466-467
-
- Article
-
- You have access
- Export citation
Invited Symposium 3: Pediatric Neuropsychology Medical Advances and Life Span Outcomes
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 665-666
-
- Article
-
- You have access
- Export citation
87 Virtual Driving Relates to Real-World Risky Driving
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 489-490
-
- Article
-
- You have access
- Export citation
36 Exploring Neuropsychological Care for Pediatric Patients in Neurocritical Care and Outpatient Follow-Up
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 143-144
-
- Article
-
- You have access
- Export citation
BEYOND LINGUISTIC INTERPRETATION IN THEORY COMPARISON
- Part of
-
- Journal:
- The Review of Symbolic Logic / Volume 17 / Issue 3 / September 2024
- Published online by Cambridge University Press:
- 21 December 2023, pp. 819-859
- Print publication:
- September 2024
-
- Article
- Export citation
DEMOCRATIC STATE, AUTOCRATIC METHOD: THE REFORM OF HUMAN RIGHTS LAW IN THE UNITED KINGDOM
-
- Journal:
- International & Comparative Law Quarterly / Volume 73 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 21 December 2023, pp. 1-27
- Print publication:
- January 2024
-
- Article
- Export citation
40 Educational Quality vs Years of Education is More Strongly Associated with Neuropsychological Test Performance
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 720-721
-
- Article
-
- You have access
- Export citation
33 Does Comorbid Depression Impact Executive Functioning (EF) in Adults Diagnosed with ADHD?: A Comparison of EF Across Diagnoses in Clinically-Referred Individuals
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 640-641
-
- Article
-
- You have access
- Export citation
6 Exercise Induced Growth Factor Increases Directly and Indirectly Reduce Systemic Vascular Risk Parameters: Translational Project Amongst Midlife Human and Animal Models of Preclinical Alzheimer’s disease and Vascular Dementia
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 218-219
-
- Article
-
- You have access
- Export citation
1 Sex Differences in Associations Between APOE ε2 and Longitudinal Cognitive Decline
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 405-406
-
- Article
-
- You have access
- Export citation
3 Two Dominant Post-COVID Subtypes in Patients Seeking Treatment for “Brain Fog” Through a Post-COVID Treatment Clinic
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 876-877
-
- Article
-
- You have access
- Export citation
