Refine listing
Actions for selected content:
141818 results in Open Access
The Effect of Physical Activity on Postural Abilities in Menopausal Women
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S713
-
- Article
-
- You have access
- Open access
- Export citation
Use of long-acting treatments in adult social care. Experience of an Acute Inpatient Mental Health Unit
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S574-S575
-
- Article
-
- You have access
- Open access
- Export citation
Sexual Experiences and Sexuality of Forensic Mental Health Patients - A Theoretical Framework
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S156
-
- Article
-
- You have access
- Open access
- Export citation
Determinants of Burnout syndrome among healthcare workers in Sahloul hospital, Tunisia: A cross sectional study
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S593-S594
-
- Article
-
- You have access
- Open access
- Export citation
The risk for inflammatory joint disease in patients with severe or treatment-resistant depression: population-based cohort study in Sweden
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S534
-
- Article
-
- You have access
- Open access
- Export citation
Psychological understanding of Anorexia nervosa gained from combined clinical care
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S556
-
- Article
-
- You have access
- Open access
- Export citation
Suicidality and social cognition: the association between hypomentalizing and suicide lethality
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S183
-
- Article
-
- You have access
- Open access
- Export citation
Deliberate self-harm and suicide in people with immigrant background: how can reason for immigration and country of origin differentiate the risks?
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S58
-
- Article
-
- You have access
- Open access
- Export citation
Correlations between Clinic Preferences and Alcohol Use Disorder: an Alcohol Cohort Study in Northern Taiwan in 2022
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S410-S411
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Chronic alcoholism can result in severe liver conditions such as fatty liver disease and cirrhosis, potentially leading to life-threatening complications and premature death.
ObjectivesThis study investigated the age-sex distribution of patients with alcohol addiction and aimed to identify differences in clinic department preferences based on their principal and additional diagnoses in Taiwan, in 2022.
MethodsWe conducted a comprehensive analysis of the diagnostic patterns of 334 patients with alcohol addiction from the Taoyuan General Hospital, Ministry of Health and Welfare.
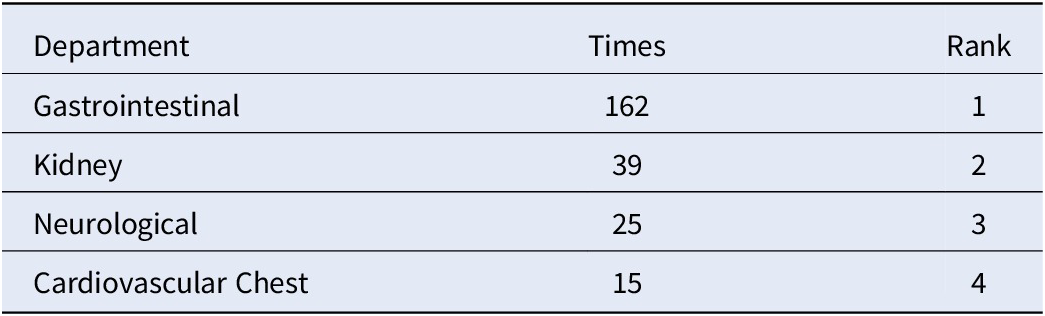
ResultsFigure 1 depicts patient demographics, highlighting 297 male and 37 female patients with alcohol-related disorders. Males aged 41-60 years were particularly dominant, as shown in Figure 2. Principal diagnoses, including alcoholic liver disease and acute pancreatitis, are detailed in Table 1. Additional diagnoses, such as chronic pancreatitis and esophageal varices, are presented in Table 2. For departmental preferences, Table 3 reveals the Gastrointestinal (GI) department as the top choice, followed by Kidney, Neurological, and Cardiovascular/Chest.
Table 1. Top 5 Principal Diagnoses of Alcohol Addiction Patients.
ICD-10-CM Principle diagnosis Times Rank K70 Alcoholic liver disease 43 1 K85 Acute pancreatitis 27 2 F10 Alcohol related disorders 18 3 A41 Other sepsis 14 4 K86 Other chronic pancreatits 11 5 Table 2. Top 5 Additional Diagnoses of Alcohol Addiction Patients.
ICD-10-CM Additional diagnosis Times Rank F10 Alcohol related disorders 40 1 K86 Other chronic pancreatits 18 2 I85 Esophageal varices 16 3 K70 Other sepsis 16 E87 Other disorders of fluid, electrolyte and acid-base balance 15 4 R65 Symptoms and signs specifically associated with systemic inflammation and infection 10 5 Table 3. Top 5 Departments for Alcoholism Patient Presentation.
Department Times Rank Gastrointestinal 162 1 Kidney 39 2 Neurological 25 3 Cardiovascular Chest 15 4 Image:
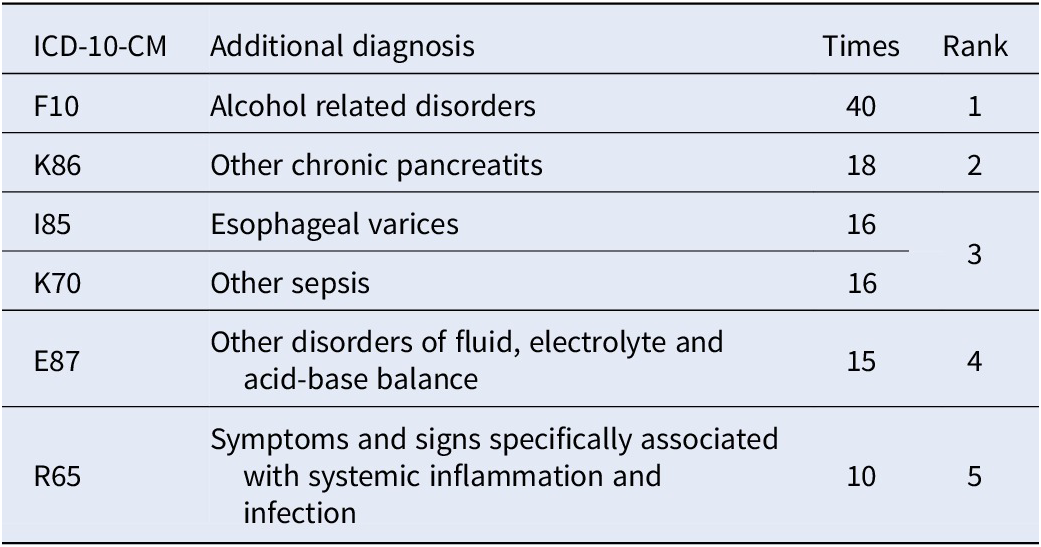
Image 2:
 Conclusions
ConclusionsThe study revealed that patients with alcohol addiction often delay seeking psychiatric help instead of presenting for medical care only after liver or gastrointestinal complications occur. This underscores the crucial need for better health education regarding the relationship between alcohol addiction and liver disease. Prompt recognition and early intervention for substance addiction can significantly reduce these risks and improve patient outcomes.
Disclosure of InterestNone Declared


Syndrome of Irreversible Lithium-Effectuated Neurotoxicity: Silent, but not innocent
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S694-S695
-
- Article
-
- You have access
- Open access
- Export citation
Mental Health Policy Name: War and mental health (Croatian experience)
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S15-S16
-
- Article
-
- You have access
- Open access
- Export citation
Recovery among people with mental health challenges and alcohol and drug use issues in the Northern Territory, Australia
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S113-S114
-
- Article
-
- You have access
- Open access
- Export citation
Exploring Burnout: A Study on Psychiatric Nurses in Tunisia
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S340
-
- Article
-
- You have access
- Open access
- Export citation
The Reductions in Phenomenology - A Comparison Across Main Authors
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S661
-
- Article
-
- You have access
- Open access
- Export citation
Exploring The Impact of Positive Behaviour Support Plans on Adult Acute Mental Health Staff Practice
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S598-S599
-
- Article
-
- You have access
- Open access
- Export citation
PTSD, dissociative experiences, and depressive symptoms in a clinical sample of women who featured in pornographic productions
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S306-S307
-
- Article
-
- You have access
- Open access
- Export citation
Psychological struggles in tunisian Infertile couples: A gender Perspective
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S157-S158
-
- Article
-
- You have access
- Open access
- Export citation
Hydroxychloroquine in systemic lupus erythematosus and psychosis. A case report
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S748-S749
-
- Article
-
- You have access
- Open access
- Export citation
Resilience and burden in family caregivers of patients with severe mental disorders
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S604-S605
-
- Article
-
- You have access
- Open access
- Export citation
Validation of the rating scales for negative symptoms: new strategies
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S18
-
- Article
-
- You have access
- Open access
- Export citation
