Refine listing
Actions for selected content:
141818 results in Open Access
The Effect of the Apollo Neuro Device on Anxiety Among Participants who Underwent Ketamine Assisted Therapy
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S423
-
- Article
-
- You have access
- Open access
- Export citation
Assessing Personality Disorders of People Who Abuse Family Members
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S607-S608
-
- Article
-
- You have access
- Open access
- Export citation
Internalized Stigma in Patients with Bipolar Disorder: A Cross-sectional Study on Its Associations with Sociodemographic, Marital and Clinical Characteristics
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S79
-
- Article
-
- You have access
- Open access
- Export citation
Telehealth Treatment of Patients with Bipolar Depression during the COVID-19 Pandemic: Comparative Safety, Patient Satisfaction, and Effectiveness to Prepandemic In-person Treatment
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S219-S220
-
- Article
-
- You have access
- Open access
- Export citation
Haematological alterations in the context of olanzapine treatment
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S691-S692
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
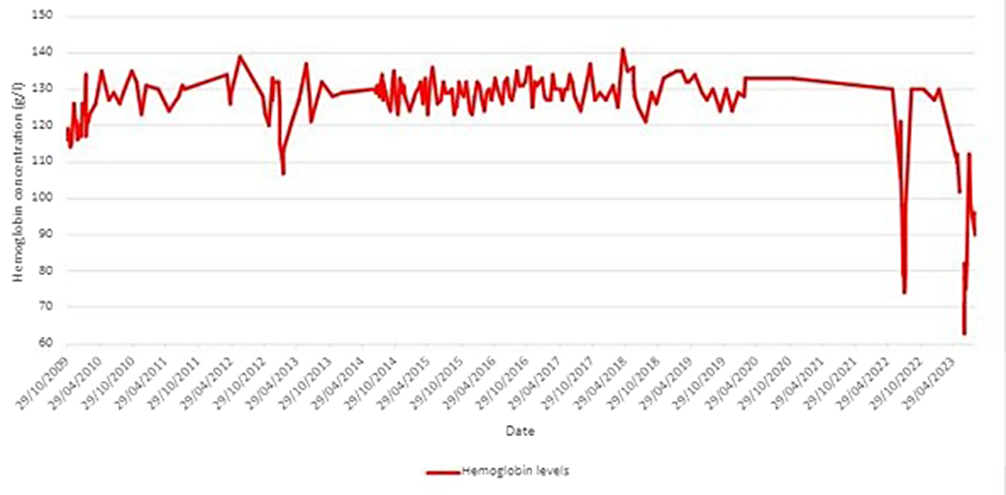
Haematological alterations, especially in the red blood cell series, are a rare adverse effect of olanzapine treatment. A 64-year-old female patient with a diagnosis of long-standing schizophrenia was admitted to the psychiatric room for psychotic decompensation and leukopenia in control laboratory tests. She had a history of mild psoriasis, allergy to sulphonamides and infectious bursitis nine years earlier secondary to neutropenia due to clozapine. On previous admission, episodes of anaemia and neutropenia related to increased doses of olanzapine were observed. On current admission, a new episode of anaemia and neutropenia occurred with doses of up to 20 mg/day of olanzapine, hemoglobin levels of 63g/L ann neutrophil count of 0,8*10^9 neutrophils/l were detected.
ObjectivesReport a very rare but serious adverse effect in patients treated with olanzapine.
MethodsHaematological analysis were periodically carried out from 2009 to 2023.
A complete study was carried out with parameters of haemolysis, autoimmunity, a pharmacogenetic study and a myelogram.
ResultsThe autoimmunity and haemolysis study excluded an autoimmune or haematological illness that could justify the haematological alterations.
The myelogram showed normal cellularity.
The pharmacogenetic study showed no relevant alterations.
Image:
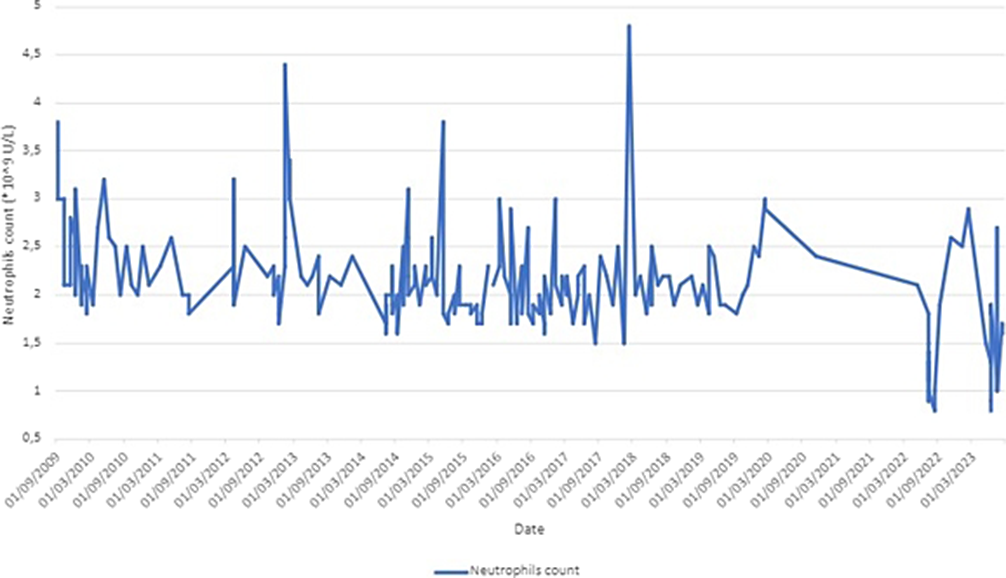
Image 2:
 Conclusions
ConclusionsThe case was classified as a non-immune haemolytic anaemia secondary to olanzapine and improved with withdrawal of the drug.
Disclosure of InterestNone Declared


Habit Learning in OCD: Preliminary Data from a Spanish Sample
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S356
-
- Article
-
- You have access
- Open access
- Export citation
Screening the dysfunctional grief and its associated factors due to a death from covid-19 in Tunisia
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S503-S504
-
- Article
-
- You have access
- Open access
- Export citation
Psychiatric disorders in professional drivers and fitness for work
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S573-S574
-
- Article
-
- You have access
- Open access
- Export citation
I smell something weird - Ictal olfactory hallucinations in patients with primary brain tumors
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S317
-
- Article
-
- You have access
- Open access
- Export citation
Non-Adaptive Defense Mechanisms and Their Relationship to Psychosomatic Disorders among a Sample of University Students
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S422
-
- Article
-
- You have access
- Open access
- Export citation
Modifying Conventional Psychiatric Practice to Serve Indigenous People
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S526
-
- Article
-
- You have access
- Open access
- Export citation
Factors influencing the health-related quality of life among persons with lower limb amputation wearing a prosthesis
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S205
-
- Article
-
- You have access
- Open access
- Export citation
Paraphrenia – current psychopathological and diagnoses landmarks
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S470
-
- Article
-
- You have access
- Open access
- Export citation
Potential Neurobiological and clinical markers in Extreme Weight Conditions: from Anorexia to Obesity
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S5
-
- Article
-
- You have access
- Open access
- Export citation
Fecal Microbiota Transplantaion in the treatement of mood disorders : A literature review
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S319-S320
-
- Article
-
- You have access
- Open access
- Export citation
Drug repurposing as add-on treatment strategy for mania and bipolar depression: systematic synthesis and qualitative appraisal of the existing meta-analytic evidence
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S323-S324
-
- Article
-
- You have access
- Open access
- Export citation
Chronic and transient loneliness in western countries: risk factors and association with depression. A follow-up study.
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S334
-
- Article
-
- You have access
- Open access
- Export citation
Insight and cognitive complaints in stabilized outpatients with schizophrenia
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S756
-
- Article
-
- You have access
- Open access
- Export citation
The Influence of Gender Roles on Eating Attitudes: A Study Among Female College Students
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S198
-
- Article
-
- You have access
- Open access
- Export citation
A pragmatic randomised controlled non-inferiority trial of open-door policy versus treatment as usual in urban psychiatric inpatient wards
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S62
-
- Article
-
- You have access
- Open access
- Export citation
