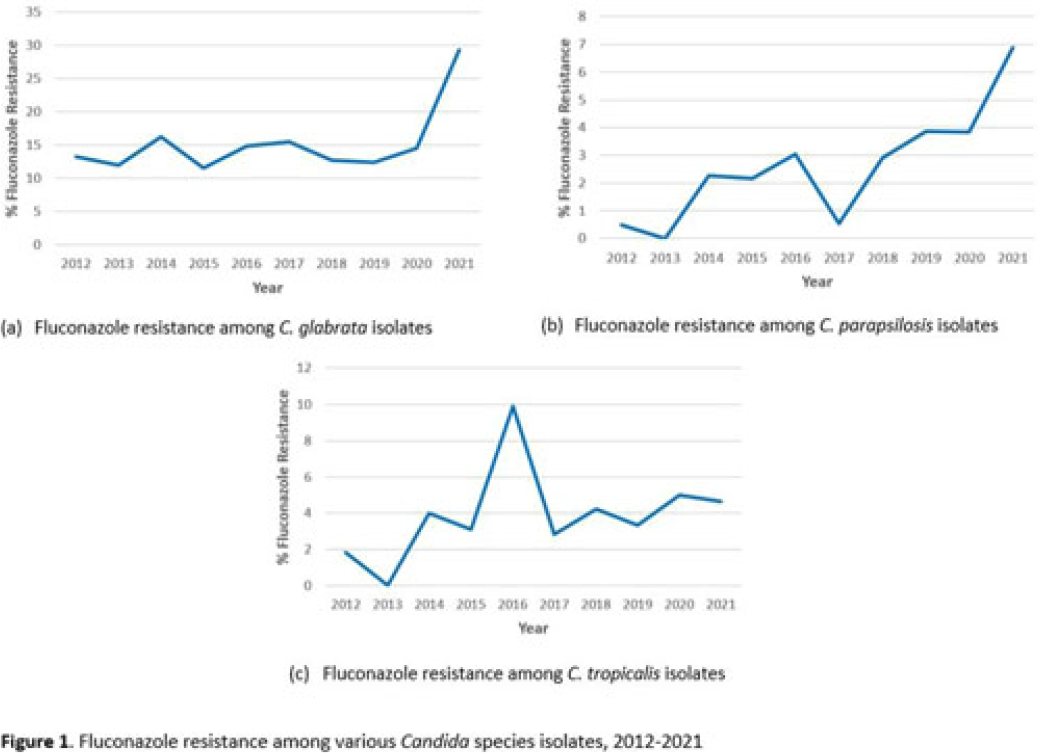
Background: Candida spp can cause a variety of infections known as candidiasis, ranging from severe invasive infections to superficial mucosal infections of the mouth and vagina. Fluconazole, a triazole antifungal, is commonly prescribed to treat candidiasis but increasing fluconazole resistance is a growing concern for several Candida spp. Although C. albicans has historically been the most common cause of candidiasis, other species are increasingly common and antifungal resistance is more prevalent in these non-albicans species, including C. glabrata, C. parapsilosis, and C. tropicalis, which were the focus of this analysis. Methods: We used the PINC AI healthcare data (PHD) database to examine fluconazole resistance for inpatient isolates between 2012 and 2021 from 187 US acute-care hospitals with at least 1 Candida spp culture with a fluconazole susceptibility result over the entire period. We calculated annual percentage fluconazole resistance for C. glabrata, C. tropicalis, and C. parapsilosis isolates using the clinical laboratory interpretation for resistance. Results: We identified 4,264 C. glabrata, 2,482 C. parapsilosis, and 2,283 C. tropicalis isolates between 2012 and 2021 with susceptibility results. The percentage of C. glabrata isolates resistant to fluconazole doubled between 2020 and 2021 (14.6% vs 29.3%) (Fig. 1a). The percentage of C. parapsilosis isolates resistant to fluconazole steadily increased since 2017 (Fig. 1b), with an 82% increase in 2021 compared with 2020 (3.8% in 2020 vs 6.9% in 2021). Fluconazole resistance among C. tropicalis isolates varied over the years, with a 0.3% decrease in 2021 from 2020 (Fig. 1c). Of hospitals reporting at least 1 result each year 2020–2021, 44% observed an increase in the proportion of C. glabrata isolates resistant to fluconazole in 2021 compared to 2020. Conclusions: Our analysis highlights a concerning increase in fluconazole resistance among C. glabrata and C. parapsilosis isolates in 2021 compared with previous years. Further investigation of the observed increases in fluconazole resistance among these Candida spp could provide further insight on potential drivers of resistance or limitations in reported results from large databases. More analyses are needed to understand rates, sites of Candida infections, and risk factors (eg, antifungal exposure) associated with resistance.
Disclosures: None

