We present the serendipitous radio-continuum discovery of a likely Galactic supernova remnant (SNR) G305.4–2.2. This object displays a remarkable circular symmetry in shape, making it one of the most circular Galactic SNRs known. Nicknamed Teleios due to its symmetry, it was detected in the new Australian Square Kilometre Array Pathfinder (ASKAP) Evolutionary Map of the Universe (EMU) radio–continuum images with an angular size of 1 320 $^{\prime\prime}$
$^{\prime\prime}$ $\times$1 260
$\times$1 260 $^{\prime\prime}$ and PA = 0
$^{\prime\prime}$ and PA = 0 $^\circ$. While there is a hint of possible H
$^\circ$. While there is a hint of possible H $\alpha$ and gamma-ray emission, Teleios is exclusively seen at radio–continuum frequencies. Interestingly, Teleios is not only almost perfectly symmetric, but it also has one of the lowest surface brightnesses discovered among Galactic SNRs and a steep spectral index of
$\alpha$ and gamma-ray emission, Teleios is exclusively seen at radio–continuum frequencies. Interestingly, Teleios is not only almost perfectly symmetric, but it also has one of the lowest surface brightnesses discovered among Galactic SNRs and a steep spectral index of  $\alpha$=–0.6
$\alpha$=–0.6 $\pm$0.3. Our best estimates from Hi studies and the
$\pm$0.3. Our best estimates from Hi studies and the  $\Sigma$–D relation place Teleios as a type Ia SNR at a distance of either
$\Sigma$–D relation place Teleios as a type Ia SNR at a distance of either  $\sim$2.2 kpc (near-side) or
$\sim$2.2 kpc (near-side) or  $\sim$7.7 kpc (far-side). This indicates two possible scenarios, either a young (under 1 000 yr) or a somewhat older SNR (over 10 000 yr). With a corresponding diameter of 14/48 pc, our evolutionary studies place Teleios at the either early or late Sedov phase, depending on the distance/diameter estimate. However, our modelling also predicts X-ray emission, which we do not see in the present generation of eROSITA images. We also explored a type Iax explosion scenario that would point to a much closer distance of
$\sim$7.7 kpc (far-side). This indicates two possible scenarios, either a young (under 1 000 yr) or a somewhat older SNR (over 10 000 yr). With a corresponding diameter of 14/48 pc, our evolutionary studies place Teleios at the either early or late Sedov phase, depending on the distance/diameter estimate. However, our modelling also predicts X-ray emission, which we do not see in the present generation of eROSITA images. We also explored a type Iax explosion scenario that would point to a much closer distance of  $\lt$1 kpc and Teleios size of only
$\lt$1 kpc and Teleios size of only  $\sim$3.3 pc, which would be similar to the only known type Iax remnant SN1181. Unfortunately, all examined scenarios have their challenges, and no definitive Supernova (SN) origin type can be established at this stage. Remarkably, Teleios has retained its symmetrical shape as it aged even to such a diameter, suggesting expansion into a rarefied and isotropic ambient medium. The low radio surface brightness and the lack of pronounced polarisation can be explained by a high level of ambient rotation measure (RM), with the largest RM being observed at Teleios’s centre.
$\sim$3.3 pc, which would be similar to the only known type Iax remnant SN1181. Unfortunately, all examined scenarios have their challenges, and no definitive Supernova (SN) origin type can be established at this stage. Remarkably, Teleios has retained its symmetrical shape as it aged even to such a diameter, suggesting expansion into a rarefied and isotropic ambient medium. The low radio surface brightness and the lack of pronounced polarisation can be explained by a high level of ambient rotation measure (RM), with the largest RM being observed at Teleios’s centre.
The coronavirus disease 2019 (COVID-19) pandemic continues to cause significant morbidity and mortality worldwide. Since a large portion of the world’s population is currently unvaccinated or incompletely vaccinated and has limited access to approved treatments against COVID-19, there is an urgent need to continue research on treatment options, especially those at low cost and which are immediately available to patients, particularly in low- and middle-income countries. Prior in vitro and observational studies have shown that fluoxetine, possibly through its inhibitory effect on the acid sphingomyelinase/ceramide system, could be a promising antiviral and anti-inflammatory treatment against COVID-19.
The aim of this sudy was to test the potential antiviral and anti-inflammatory activities of fluoxetine against SARS-CoV-2 in a K18-hACE2 mouse model of infection, and against several variants of concern in vitro, and test the hypothesis of the implication of ceramides and/or their derivatives hexosylceramides.
We evaluated the potential antiviral and anti-inflammatory activities of fluoxetine in a K18-hACE2 mouse model of SARS-CoV-2 infection, and against variants of concern in vitro, i.e., SARS-CoV-2 ancestral strain, Alpha B.1.1.7, Gamma P1, Delta B1.617 and Omicron BA.5.
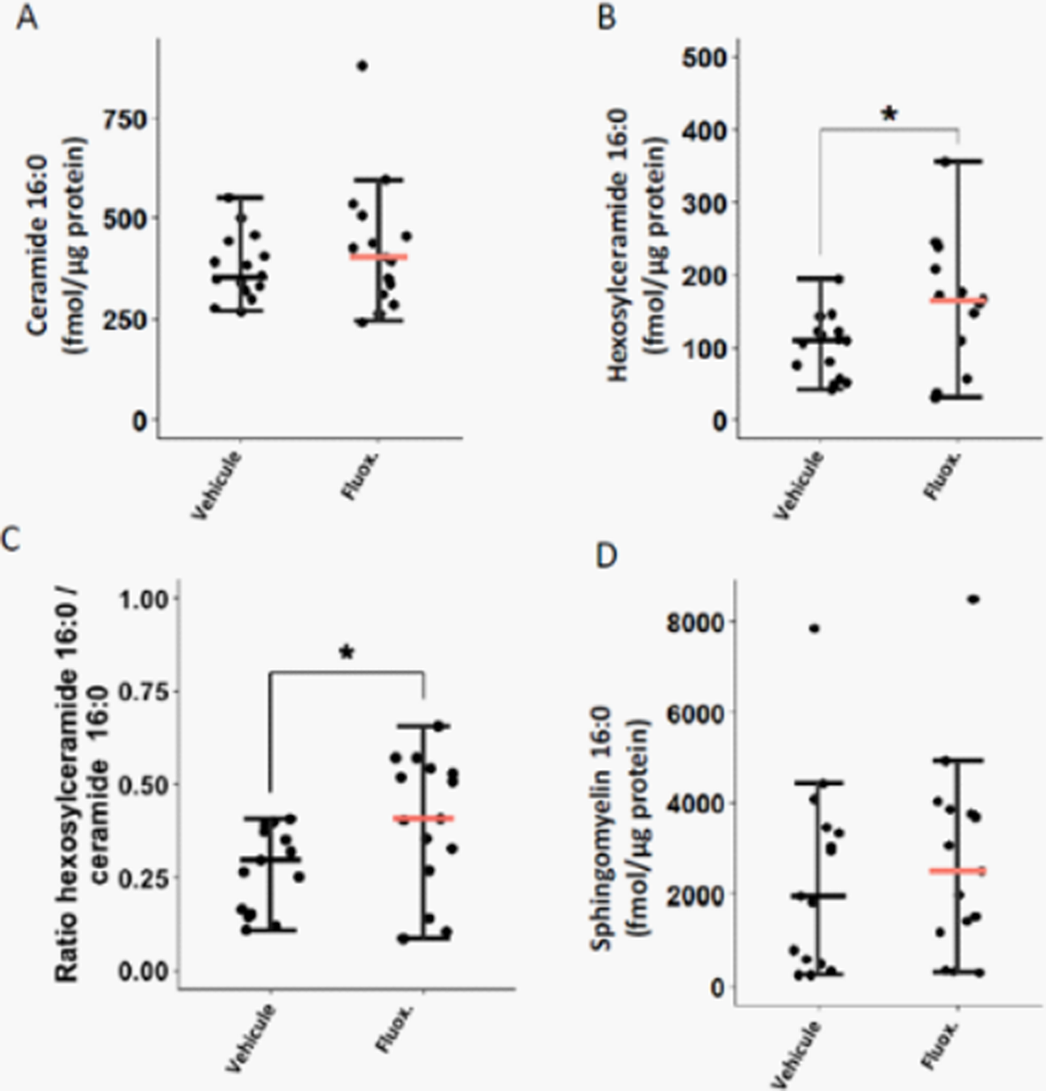
Fluoxetine, administrated after SARS-CoV-2 infection, significantly reduced lung tissue viral titres (Figure 1) and expression of several inflammatory markers (i.e., IL-6, TNFα, CCL2 and CXCL10) (Figure 2). It also inhibited the replication of all variants of concern in vitro. A modulation of the ceramide system in the lung tissues, as reflected by the increase in the ratio HexCer 16:0/Cer 16:0 in fluoxetine-treated mice, may contribute to explain these effects (Figure 3).
Image:
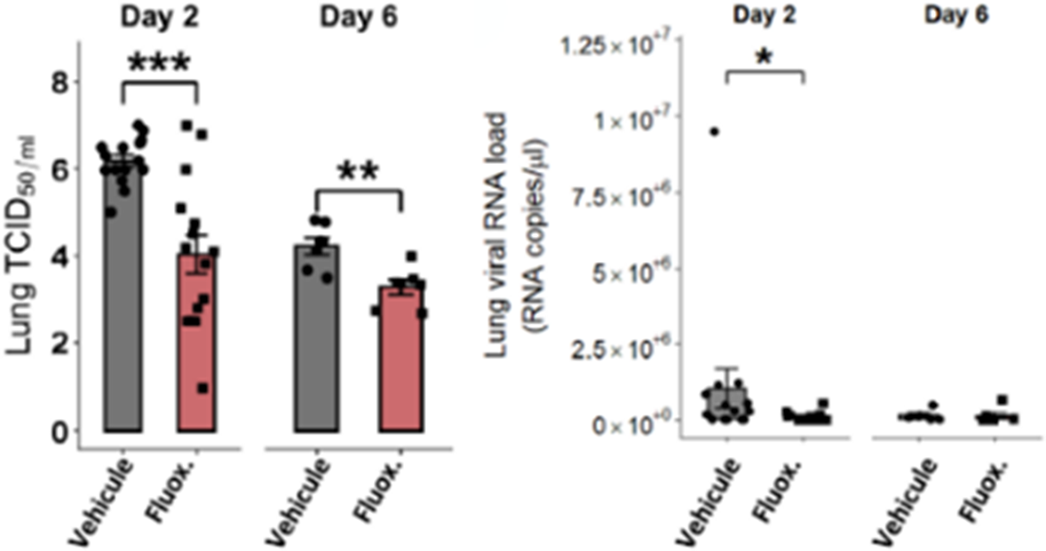
Image 2:
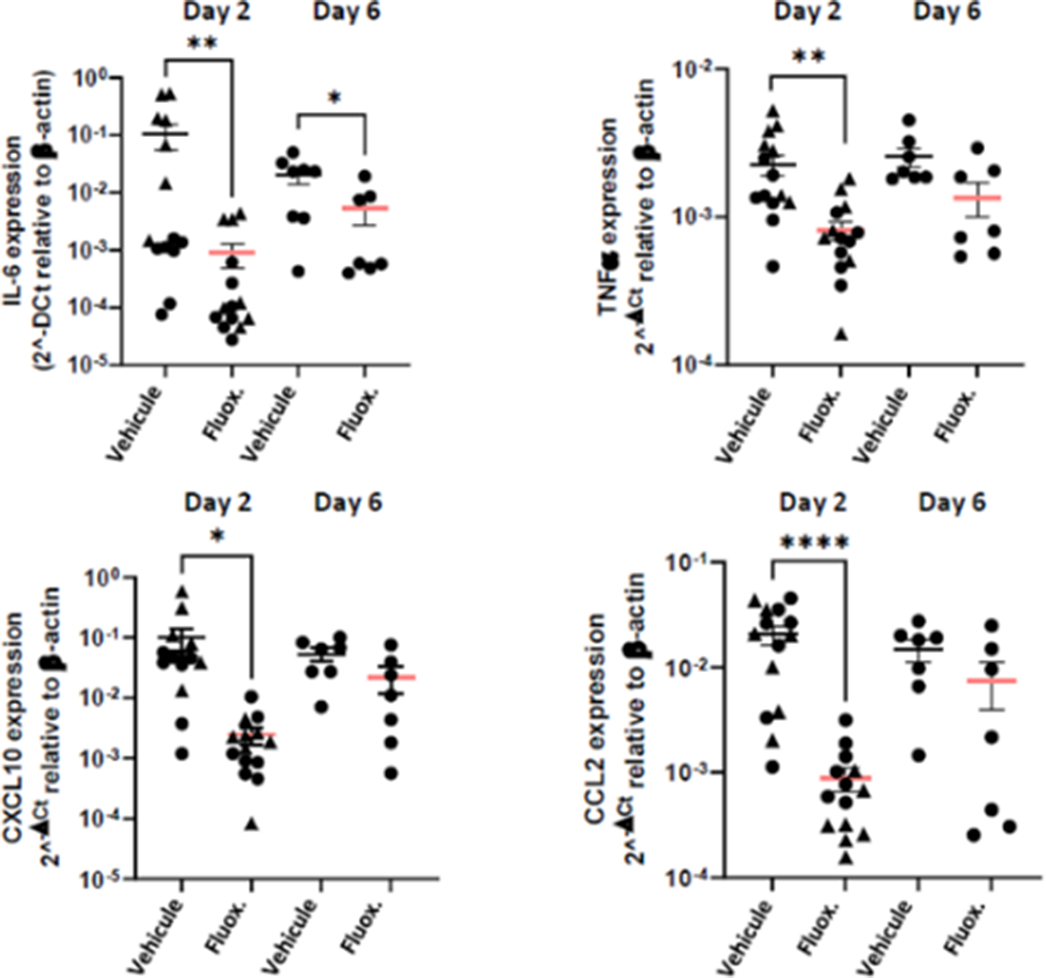
Image 3:
Our findings demonstrate the antiviral and anti-inflammatory properties of fluoxetine in a K18-hACE2 mouse model of SARS-CoV-2 infection, and its in vitro antiviral activity against variants of concern, establishing fluoxetine as a very promising candidate for the prevention and treatment of SARS-CoV-2 infection and disease pathogenesis.
None Declared
To reduce Coronavirus Disease 2019 (COVID-19)-related mortality and morbidity, widely available oral COVID-19 treatments are urgently needed. Certain antidepressants, such as fluvoxamine or fluoxetine, may be beneficial against COVID-19.
The main objective was two-fold: (i) to test the hypothesis that the prevalence of antidepressant use in patients hospitalized with COVID-19 would be lower than in patients with similar characteristics hospitalized without COVID-19, and (ii) to examine, among patients hospitalized with COVID-19, whether antidepressant use is associated with reduced 28-day mortality. Our secondary aim was to examine whether this potential association could only concern specific antidepressant classes or molecules, is dose-dependent, and/or only observed beyond a certain dose threshold.
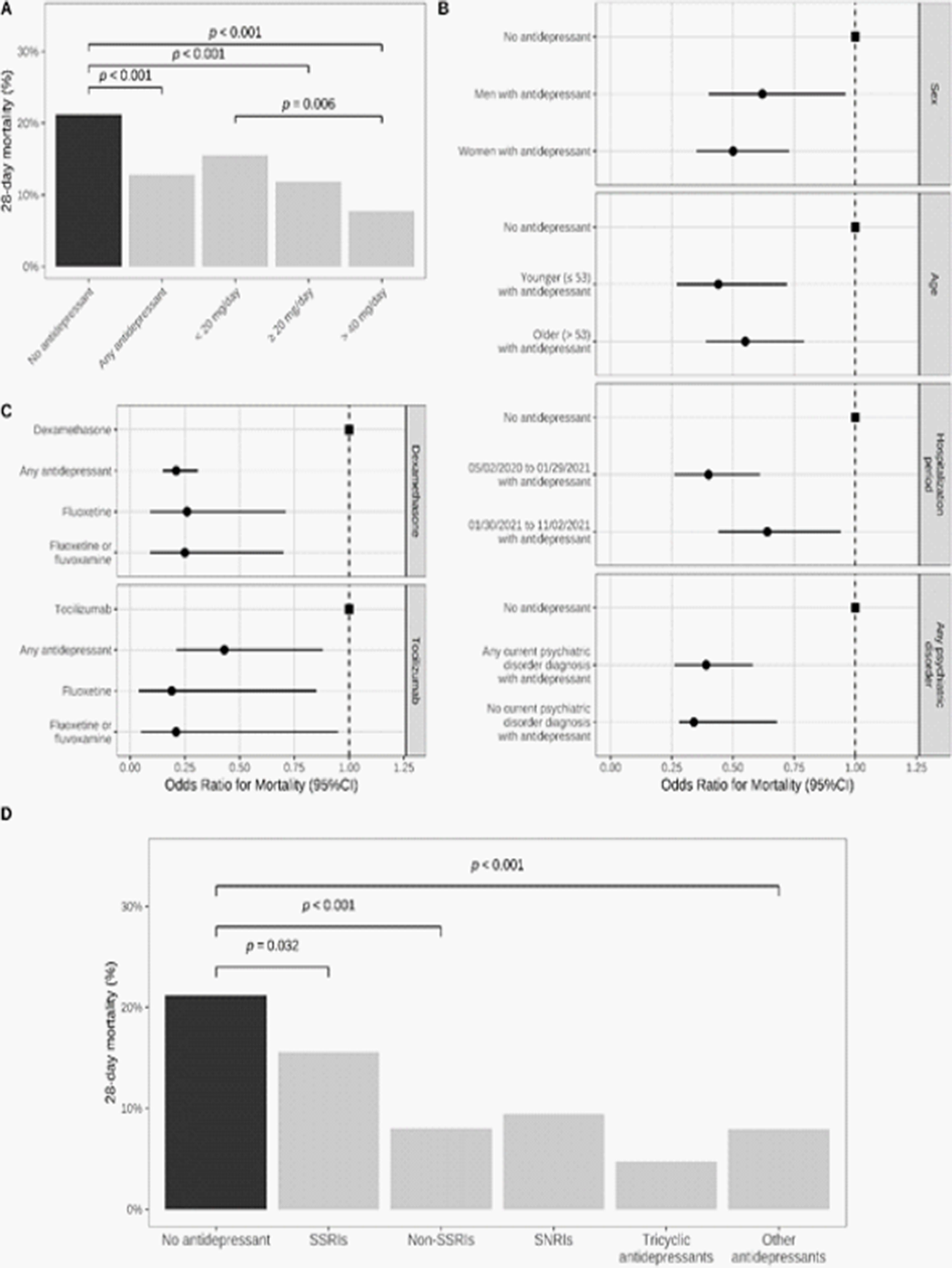
We included 388,945 adult inpatients who tested positive for SARS-CoV-2 at 36 AP–HP (Assistance Publique–Hôpitaux de Paris) hospitals from 2 May 2020 to 2 November 2021. We compared the prevalence of antidepressant use at admission in a 1:1 ratio matched analytic sample with and without COVID-19 (N = 82,586), and assessed its association with 28-day all-cause mortality in a 1:1 ratio matched analytic sample of COVID-19 inpatients with and without antidepressant use at admission (N = 1482) (Figure 1).
Antidepressant use was significantly less prevalent in inpatients with COVID-19 than in a matched control group of inpatients without COVID-19 (1.9% versus 4.8%; Odds Ratio (OR) = 0.38; 95%CI = 0.35–0.41, p < 0.001) (Figure 2). Antidepressant use was significantly associated with reduced 28-day mortality among COVID-19 inpatients (12.8% versus 21.2%; OR = 0.55; 95%CI = 0.41–0.72, p < 0.001), particularly at daily doses of at least 40 mg fluoxetine equivalents (Figure 3). Antidepressants with high FIASMA (Functional Inhibitors of Acid Sphingomyelinase) activity seem to drive both associations.
Image:
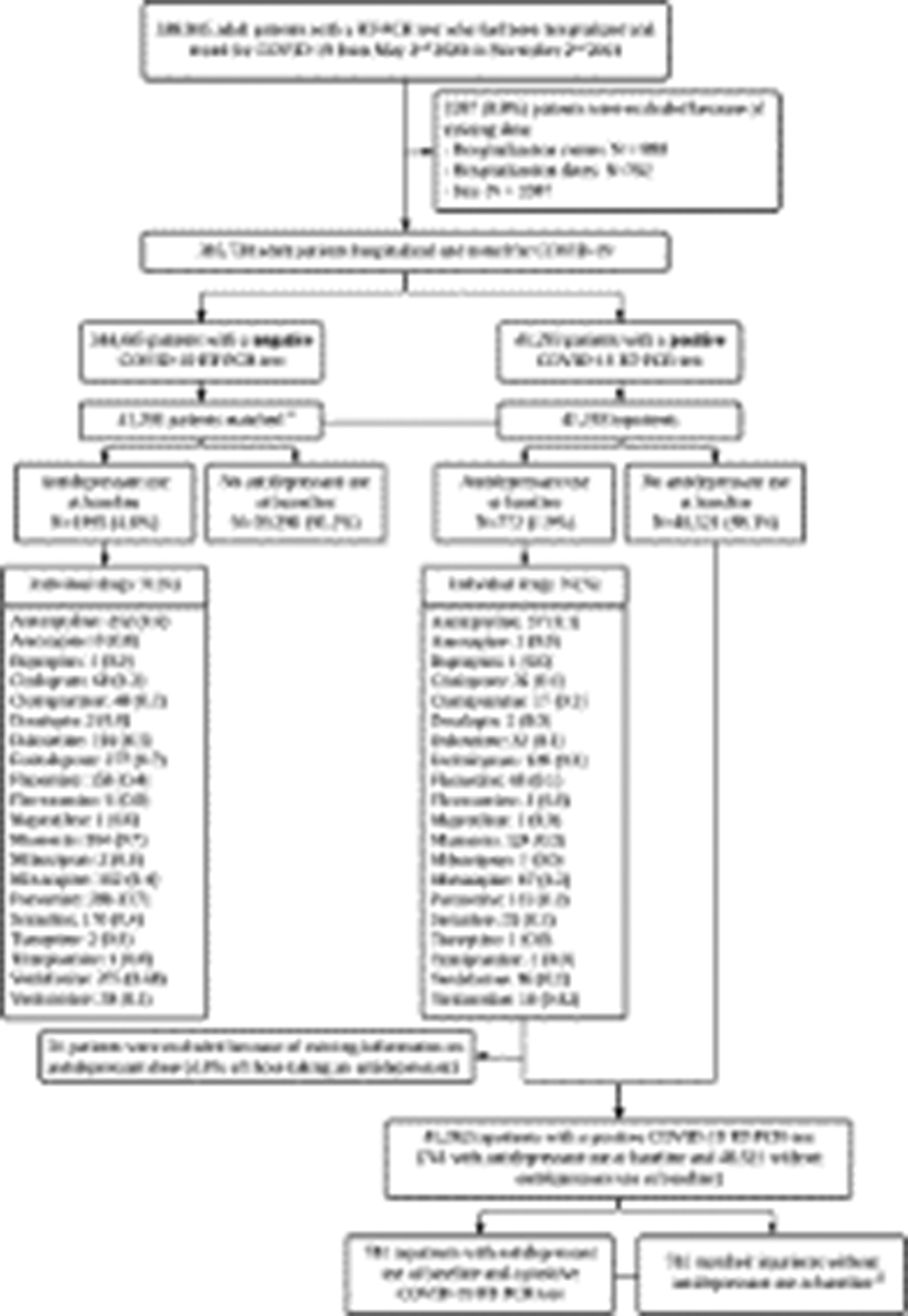
Image 2:
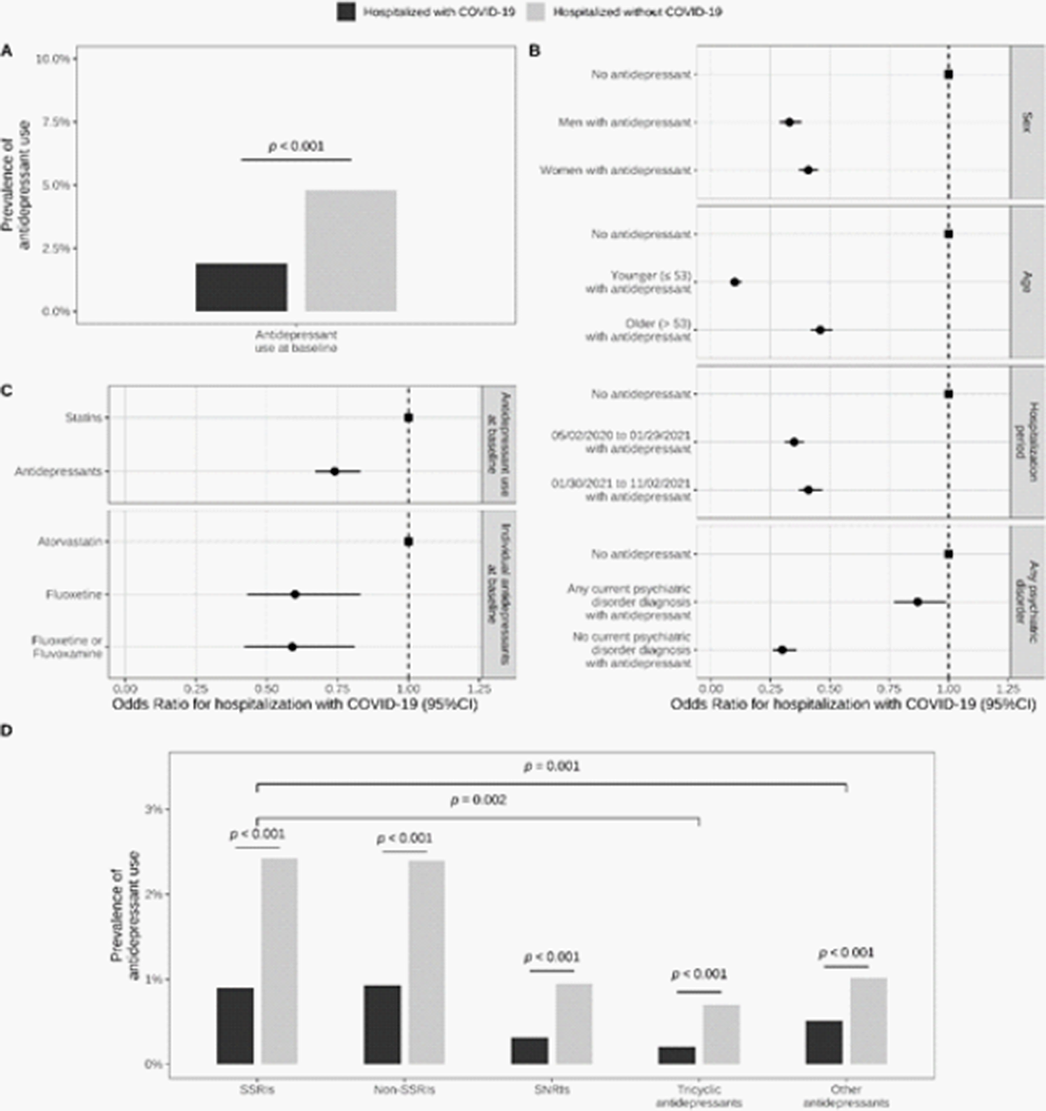
Image 3:
Antidepressant use is associated with a reduced likelihood of hospitalization in patients infected with SARS-CoV-2 and with a reduced risk of death in patients hospitalized with COVID-19. These associations were stronger for molecules with high FIASMA activity. These findings posit that prospective interventional studies of antidepressants with the highest FIASMA activity may be appropriate to help identify variant-agnostic, affordable, and scalable interventions for outpatient and inpatient therapy of COVID-19.
None Declared

