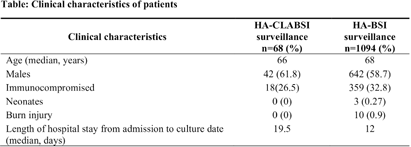
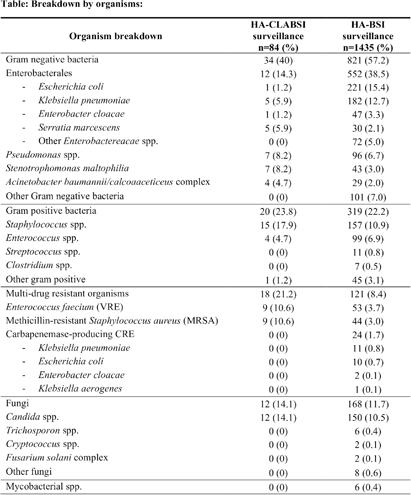
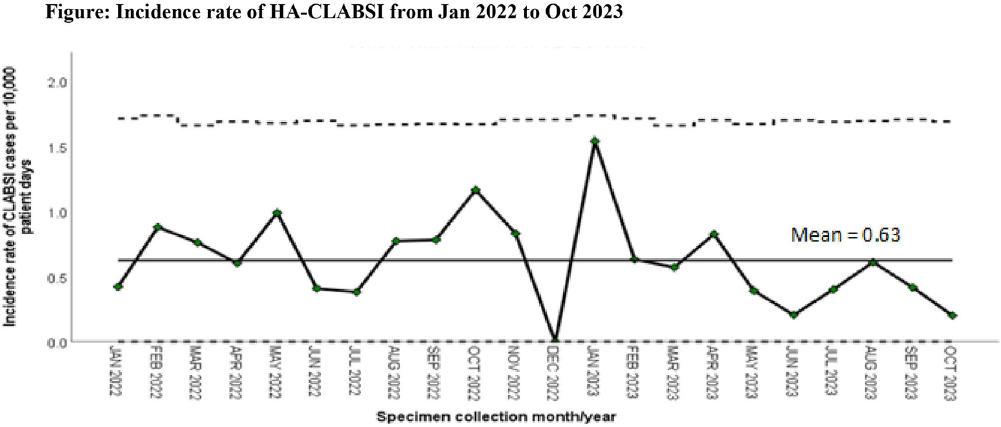
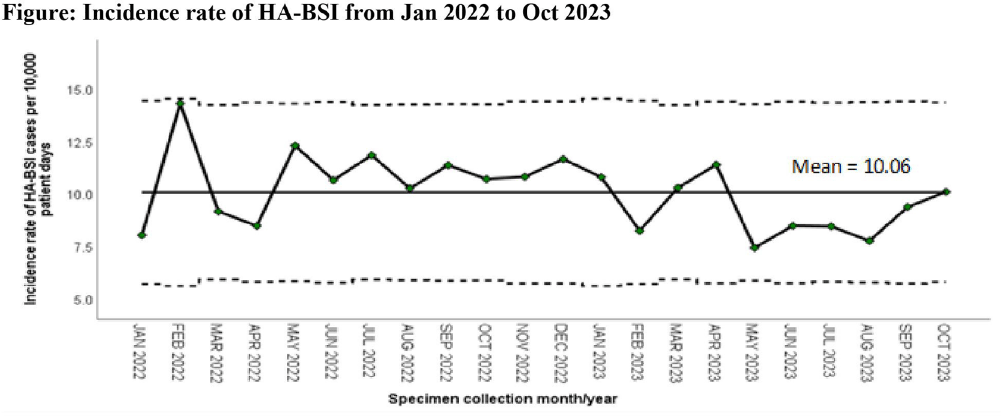
Background: Healthcare-associated central line associated bloodstream infection (HA-CLABSI) surveillance is important for monitoring healthcare-associated infections (HAIs) and evaluating effectiveness of infection prevention (IP) measures. However, implementing it is a laborious and time-consuming approach. Exclusive focus on central lines neglects HAI risk due to peripheral vascular catheters. This study aimed to assess whether HA-CLABSI incidence could be inferred from HA-bloodstream infection (BSI) trends and explore shift to HA-BSI surveillance. Methods: The study was performed in a Singaporean tertiary care hospital. Electronic medical records review was performed to determine whether positive blood cultures met Centers for Disease Control/National Health Safety Network (CDC/NHSN) definitions for HA-CLABSI and HA-BSI. Incident episodes of HA-BSI were included (excluding positive cultures repeated within 14 days). Incident organisms were explored to identify common causative pathogens (excluding same organisms isolated from cultures repeated within 14 days). CLABSI and BSI occurring ≥72hrs after admission were considered healthcare-associated. Patients under oncology or hematology service were considered immunocompromised. Incidence rates (IR) per 10,000 patient-days, patient characteristics and causative pathogens were compared between both indicators. Results: From January 2022 to October 2023, mean IR for HA-CLABSI was 0.63 (n=68) and for HA-BSI was 10.06 (n=1094). Median age of patients with HA-CLABSI was 66 years and HA-BSI was 68 years. HA-CLABSI and HA-BSI were more common in males (60.86% & 58.68%). Median duration between admission to HA-CLABSI was 20 days and to HA-BSI was 12 days. Median duration between central line insertion to HA-CLABSI was 16 days. Of 1094, 631 (57.7%) patients had vascular catheter(s) (i.e., IV cannula, port-a-cath, peripherally-inserted central catheter or central line) inserted at time of HA-BSI diagnosis, of whom 46 (7.3%) patients had CLABSI ±2days from positive blood culture. There was no significant correlation between monthly aggregate data from these indicators (Spearman’s correlation coefficient= 0.36, p-value=0.1). Predominant organisms causing HA-CLABSI and HA-BSI were gram negative bacteria (GNB, 40% & 57.21%), gram positive bacteria (24.71% & 22.23%), and fungi. Common GNB in CLABSI patients were Pseudomonas spp. and Stenotrophomonas maltophilia (8.24%), followed by Serratia marcescens and Klebsiella pneumoniae (5.88%). The frequent GNB in HA-BSI patients were Escherichia coli (15.4%), Klebsiella pneumonia (12.68%), and Pseudomonas spp. (6.69%). Common multi-drug resistant organisms were vancomycin-resistant Enterococcus faecium (10.59% & 3.69%) and methicillin-resistant Staphylococcus aureus (10.59% & 3.07%). Conclusion: HA-BSI did not correlate with HA-CLABSI. HA-BSI reflects heterogenous population outcomes. For utilization as surveillance indicator, further assessment on exclusion criteria is required to improve specificity.
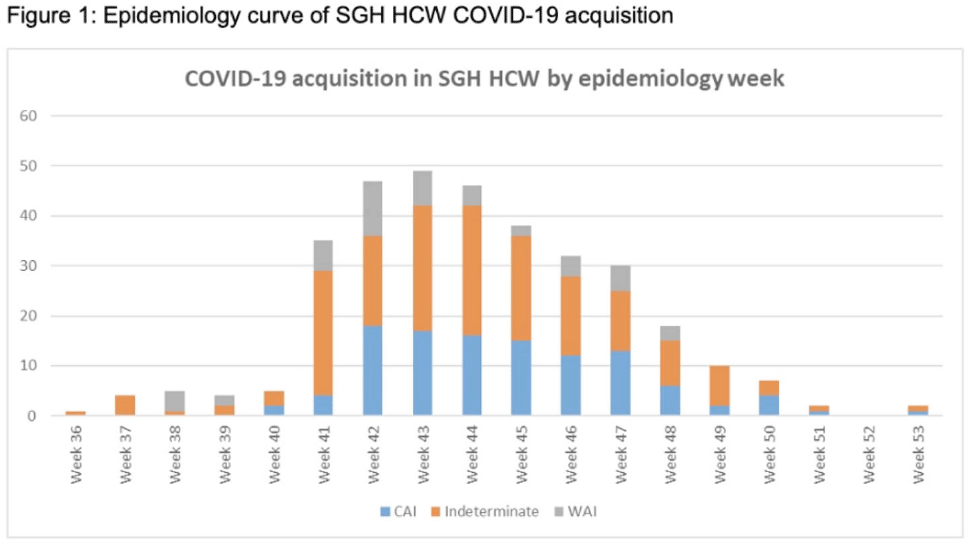
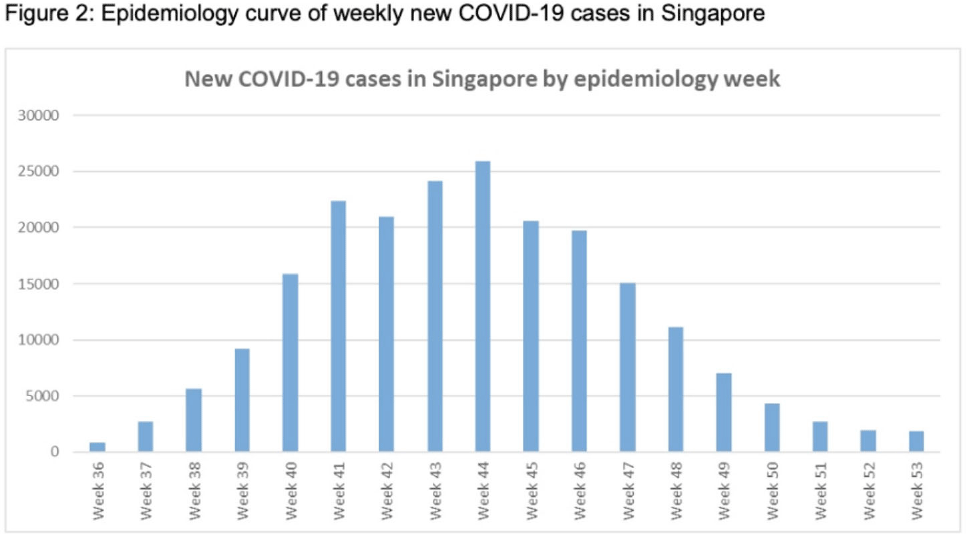
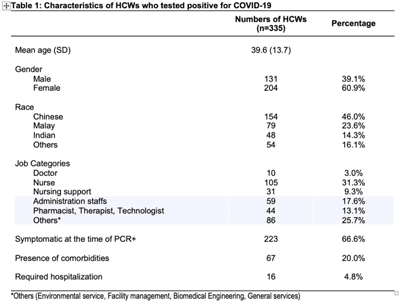
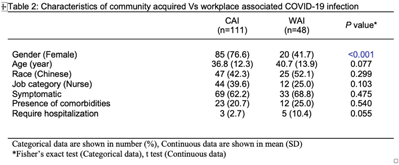
Background: Singapore General Hospital (SGH) is the largest acute tertiary-care hospital in Singapore. Healthcare workers (HCWs) are at risk of acquiring COVID-19 in both the community and workplaces. SGH has a robust exposure management process including prompt contact tracing, immediate ring fencing, lock down of affected cubicles or single room isolation for patient contacts, and home isolation orders for staff contacts of COVID-19 cases during the containment phase of the pandemic. Contacts were also placed on enhanced surveillance with PCR testing on days 1 and 4 as well as daily antigen rapid tests (ARTs) for 10 days after exposure. Here, we describe the characteristic of HCWs with COVID-19 during the third wave of the COVID-19 pandemic. Methods: This retrospective observational study included all SGH HCWs who acquired COVID-19 during the third wave (ie, the 18-week period from September 1 to December 31, 2021) of the COVID-19 pandemic. Univariate analysis was used to compare characteristics of work-associated infection (WAI) and community-acquired infection (CAI) among HCWs. Results: Among a workforce of >10,000 at SGH, 335 HCWs acquired COVID-19 during study period. CAI (exposure to known clusters or household contact) accounted for 111 HCW infections (33.1%). Also, 48 HCWs (14.3%) had a WAI (ie, acquired at their work places where there was no patient contact). Among WAsI, only 5 HCWs had hospital-acquired infection (confirmed by phylogenetic analysis). The sources of exposure for the remaining 176 HCWs were unknown. Weekly incidence of COVID-19 among HCWs was comparable to the epidemiology curve of all cases in Singapore (Fig. 1 and 2). The mean age of HCWs with COVID-19 was 39.6 years, and most were women. At the time of positive SARS-CoV-2 PCR test, 223 HCWs were symptomatic, and 67 (20.0%) of them had comorbidities. Only 16 HCWs (4.8%) required hospitalization, and all recovered fully with no mortality (Table 1). Being female was associated with community COVID-19 acquisition (OR, 4.6, P Conclusions: During the thrid wave of the COVID-19 pandemic, a higher percentage of HCWs at SGH acquired the infection from the community than from the workplace. Safe management measures, such as universal masking, social distancing, and robust exposure management processes including prompt contact tracing and environmental disinfection, can reduce the risk of COVID-19 in the hospital work environment.
Funding: None
Disclosures: None